Download as docx, pdf, or txt
You might also like
- Davis Advantage For Maternal-Child Nursing Care, 3eDocument3,037 pagesDavis Advantage For Maternal-Child Nursing Care, 3eRemington Eckhardt100% (1)
- Mini Vet Guide Preview 1Document28 pagesMini Vet Guide Preview 1Mariana HiginoNo ratings yet
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtFrom EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtRating: 5 out of 5 stars5/5 (1)
- UW Path NoteDocument218 pagesUW Path NoteSophia Yin100% (4)
- What Is HomeoprophylaxisDocument6 pagesWhat Is HomeoprophylaxiswrestlerloverNo ratings yet
- CNA772 - Respiratory Failure in ARDSDocument8 pagesCNA772 - Respiratory Failure in ARDSAby ZuñigaNo ratings yet
- Veterinary Pathology Online: Coronary Arteriosclerosis With Myocardial Atrophy in A 13-Year-Old DogDocument4 pagesVeterinary Pathology Online: Coronary Arteriosclerosis With Myocardial Atrophy in A 13-Year-Old DogRais YunarkoNo ratings yet
- Congestive Heart Failure, Cardiomyopathy and Myocarditis I. Congestive Heart FailureDocument23 pagesCongestive Heart Failure, Cardiomyopathy and Myocarditis I. Congestive Heart Failurelovelyc95No ratings yet
- Topic 18. Rheumatic DiaseasesDocument8 pagesTopic 18. Rheumatic DiaseasesAdeleye John AdebolaNo ratings yet
- DR - Bushra Al-Tarawneh, MD: Cardiovascular SystemDocument37 pagesDR - Bushra Al-Tarawneh, MD: Cardiovascular SystemHamzehNo ratings yet
- ValvularHeartDisease Notes S5w4Document6 pagesValvularHeartDisease Notes S5w4razzletothedazzleNo ratings yet
- CardiomyopathDocument24 pagesCardiomyopathNasasira CosmasNo ratings yet
- Restrictive CardiomyopathyDocument29 pagesRestrictive CardiomyopathyAbnet WondimuNo ratings yet
- Pathophysiology of Atherosclerosis, Thrombosis and EmbolismDocument4 pagesPathophysiology of Atherosclerosis, Thrombosis and EmbolismKeshant Samaroo100% (1)
- PathologyDocument9 pagesPathologyGeorge MagedNo ratings yet
- Acute Rheumatic FeverDocument25 pagesAcute Rheumatic FeverNeeraj JoshiNo ratings yet
- General Pathology: Growth AdaptationsDocument93 pagesGeneral Pathology: Growth AdaptationsPrarthanaNo ratings yet
- Asda Discussion Final-2Document63 pagesAsda Discussion Final-2AmjadAnsariNo ratings yet
- ABS Cell PathologyDocument26 pagesABS Cell Pathologyarmin509No ratings yet
- Atherosclerosis in Parrots. A ReviewDocument12 pagesAtherosclerosis in Parrots. A ReviewSítio das CalopsitasNo ratings yet
- Pathology LectureDocument3 pagesPathology LectureAbdullahayad farouqNo ratings yet
- Histologically, The Chancre Is Characterised byDocument6 pagesHistologically, The Chancre Is Characterised byIsak ShatikaNo ratings yet
- Cardiovascular2006 Lecture NotesDocument31 pagesCardiovascular2006 Lecture NotescystanarisaNo ratings yet
- Disturbances of CirculationDocument10 pagesDisturbances of CirculationSuhan HasanNo ratings yet
- Heart PathologyDocument6 pagesHeart PathologyHelenCandyNo ratings yet
- Thromboembolism in The Cat - WSAVA2005 - VINDocument8 pagesThromboembolism in The Cat - WSAVA2005 - VINPet Anjo DiademaNo ratings yet
- Week 11 Revision SheetsDocument10 pagesWeek 11 Revision SheetscassandramacphersonNo ratings yet
- Cardiogenic ShockDocument11 pagesCardiogenic ShockSunil YadavNo ratings yet
- Felina Clinical Nutrition - Feline Cardiomyopathies - IVIS PDFDocument16 pagesFelina Clinical Nutrition - Feline Cardiomyopathies - IVIS PDFSofia ClaudinoNo ratings yet
- Ventricular FibrillationDocument6 pagesVentricular FibrillationclubsanatateNo ratings yet
- R Valvular Heart DiseaseDocument77 pagesR Valvular Heart DiseaseAmanuel MaruNo ratings yet
- Lecture13 & 14aDocument5 pagesLecture13 & 14aIsak ShatikaNo ratings yet
- DB50 - Pa Tho Physiology and Pathology of ShockDocument4 pagesDB50 - Pa Tho Physiology and Pathology of ShockChelsea RoseNo ratings yet
- Main DivisionDocument61 pagesMain DivisionChadCowgillNo ratings yet
- Dơnload Zelensky The Unlikely Ukrainian Hero Who Defied Putin and United The World 1st Edition Andrew L Urban Chris Mcleod Full ChapterDocument25 pagesDơnload Zelensky The Unlikely Ukrainian Hero Who Defied Putin and United The World 1st Edition Andrew L Urban Chris Mcleod Full Chapterpotzcheou100% (3)
- Renal Tubular Acidosis Type IDocument7 pagesRenal Tubular Acidosis Type IAmber LiaqatNo ratings yet
- IntroductionDocument13 pagesIntroductionSiyara AntonyNo ratings yet
- Feline Hypertrophic Cardiomyopathy FHCMDocument8 pagesFeline Hypertrophic Cardiomyopathy FHCMClaritha TaopanNo ratings yet
- Non-Pharmacological Measures: PacemakerDocument11 pagesNon-Pharmacological Measures: PacemakerAlmendra Olenka LSNo ratings yet
- Acute StrokeDocument13 pagesAcute StrokeJoel CanenciaNo ratings yet
- REFERRAT Rabdomiolisis JOSDocument16 pagesREFERRAT Rabdomiolisis JOSAndaru Kusuma PrajaNo ratings yet
- Pathology of Myxomatous Mitral Valve Disease in The Dog: Philip R. Fox, DVM, MSCDocument24 pagesPathology of Myxomatous Mitral Valve Disease in The Dog: Philip R. Fox, DVM, MSCKrlÖz Ändrz Hërëdîa ÖpzNo ratings yet
- Patologia Aparatului CardiovascularDocument35 pagesPatologia Aparatului CardiovascularAndreea Cristina AndreeaNo ratings yet
- Cardiomyopathy and MyocarditisDocument8 pagesCardiomyopathy and Myocarditisoddone_out100% (1)
- Causes of Clubbing:: Cardiac Murmurs and Location Best HeardDocument3 pagesCauses of Clubbing:: Cardiac Murmurs and Location Best HeardMichelle De FreitasNo ratings yet
- Mitral Valve ProlapseDocument7 pagesMitral Valve ProlapsehracakNo ratings yet
- Mechanical AsphyxiaDocument73 pagesMechanical Asphyxiaapi-61200414No ratings yet
- Acute Myocardial InfarctionDocument14 pagesAcute Myocardial InfarctionJardee DatsimaNo ratings yet
- Cellular Injury & AdaptationDocument98 pagesCellular Injury & AdaptationFYMNo ratings yet
- To Remember The Four Causes of Cell InjuryDocument43 pagesTo Remember The Four Causes of Cell Injuryapi-3825096No ratings yet
- Topic 16. AtherosclerosisDocument6 pagesTopic 16. AtherosclerosisAdeleye John AdebolaNo ratings yet
- Acute Limb Ischemia 2017 - OKDocument21 pagesAcute Limb Ischemia 2017 - OKDiego RodriguesNo ratings yet
- Cardiac Sarcoidosis: Abdul R Doughan, Byron R WilliamsDocument7 pagesCardiac Sarcoidosis: Abdul R Doughan, Byron R WilliamsBhagya Narayan PanditNo ratings yet
- Master Plan Patho!Document94 pagesMaster Plan Patho!chiarastanziola01No ratings yet
- 1.2.3 Blood Loss, Hypovolaemic Shock, and Septic ShockDocument11 pages1.2.3 Blood Loss, Hypovolaemic Shock, and Septic ShockZayan SyedNo ratings yet
- Lab No.3 For 3 Stage: Irreversible Cell Injury (Necrosis)Document31 pagesLab No.3 For 3 Stage: Irreversible Cell Injury (Necrosis)medical.student.messiNo ratings yet
- ThrombosisDocument11 pagesThrombosisNobby Onist JuniorNo ratings yet
- Hemodynamic Disorders-RevisedDocument118 pagesHemodynamic Disorders-Revisedspringding0% (1)
- Bioquimica de La Isquemia y Reperfusion ArticuloDocument35 pagesBioquimica de La Isquemia y Reperfusion ArticulofelipeNo ratings yet
- Subiecte Rezolvate Sem 2Document46 pagesSubiecte Rezolvate Sem 2Gionea MadalinaNo ratings yet
- Ischemic Heart DiseasesDocument26 pagesIschemic Heart DiseasesFavourNo ratings yet
- Backup of Homeostatic ImbalancesDocument5 pagesBackup of Homeostatic ImbalancesDwi N.No ratings yet
- PancreatitisDocument23 pagesPancreatitissalmanhabeebekNo ratings yet
- Government of West BengalDocument5 pagesGovernment of West BengalNupur MandalNo ratings yet
- Barium SwallowDocument2 pagesBarium SwallowmameenNo ratings yet
- REAL in Nursing Journal (RNJ) : Relaksasi Autogenik Menurunkan Kadar Gula Darah Pasien Diabetes Melitus Tipe 2Document9 pagesREAL in Nursing Journal (RNJ) : Relaksasi Autogenik Menurunkan Kadar Gula Darah Pasien Diabetes Melitus Tipe 2gherice serumenaNo ratings yet
- Metabolic Aspects of Chronic Liver DiseaseDocument390 pagesMetabolic Aspects of Chronic Liver DiseaseAndre SamsungNo ratings yet
- VILLAMIN - Drug StudyDocument4 pagesVILLAMIN - Drug StudyAzizah VillaminNo ratings yet
- Acute Respiratory InfectionDocument15 pagesAcute Respiratory InfectionmNo ratings yet
- Cebu Doctors' University - College of Medicine Preventive and Social MedicineDocument14 pagesCebu Doctors' University - College of Medicine Preventive and Social MedicinefilchibuffNo ratings yet
- Ethnobotany of Medicinal Plants Used in Xalpatlahuac, Guerrero, MéxicoDocument7 pagesEthnobotany of Medicinal Plants Used in Xalpatlahuac, Guerrero, MéxicoEmmanuel Torre ArenasNo ratings yet
- General Examination of A ChildDocument4 pagesGeneral Examination of A ChildYasin KadriNo ratings yet
- Karnofsky Performance StatusDocument1 pageKarnofsky Performance Statusmu_crNo ratings yet
- Lesson 22: Diabetes Mellitus, Part 1 (Lesson Information) : Reading AssignmentDocument14 pagesLesson 22: Diabetes Mellitus, Part 1 (Lesson Information) : Reading AssignmentadaezeNo ratings yet
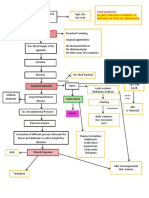
- CPC - Appendicitis (Flowchart)Document1 pageCPC - Appendicitis (Flowchart)Milet NacionalesNo ratings yet
- NCM103 12th Endoc IIDocument9 pagesNCM103 12th Endoc IIKamx MohammedNo ratings yet
- Hyperbaric Oxygen TherapyDocument7 pagesHyperbaric Oxygen Therapy18juni1995No ratings yet
- Toxicity: System of A DownDocument6 pagesToxicity: System of A DownKelson Daniel RodriguesNo ratings yet
- PPPD HandoutDocument5 pagesPPPD HandoutLeeNo ratings yet
- PTSD Checklist Civilian VersionDocument2 pagesPTSD Checklist Civilian VersionVVlynnNo ratings yet
- Cerebral Palsy: An Overview: The Centers For Disease ControlDocument8 pagesCerebral Palsy: An Overview: The Centers For Disease ControlAlma PradiftaNo ratings yet
- Ganotherapy The Miraculous King of HerbsDocument22 pagesGanotherapy The Miraculous King of HerbsCsikós Ilona100% (2)
- Health Is WealthDocument5 pagesHealth Is Wealthkanda71No ratings yet
- Cholesterol Lab ReportDocument9 pagesCholesterol Lab Reportapi-313510960No ratings yet
- 06 Psychiatry 25092019Document8 pages06 Psychiatry 25092019Sai RevanthNo ratings yet
- Purification of The Heart (Reading Packet) - OnlineDocument55 pagesPurification of The Heart (Reading Packet) - OnlineEram Haque100% (1)
- Salarsaeedimodule1 MicrobNOT COMPLETE 3 PDFDocument34 pagesSalarsaeedimodule1 MicrobNOT COMPLETE 3 PDFFatemeh BemanaNo ratings yet