Download as pdf or txt
You might also like
- The Smoothie Diet 21 Day Rapid Weight LoDocument10 pagesThe Smoothie Diet 21 Day Rapid Weight LoKutemukan JodohkuNo ratings yet
- Ld. Ld. Bui Bui: Approved by Renee Mcgregor Approved by Renee McgregorDocument79 pagesLd. Ld. Bui Bui: Approved by Renee Mcgregor Approved by Renee McgregorMaryam RizwanNo ratings yet
- Biochemistry of Vitamin CDocument24 pagesBiochemistry of Vitamin CAurelia HernandezNo ratings yet
- Ascorbic Acid-Vitamin C Brochure PDFDocument8 pagesAscorbic Acid-Vitamin C Brochure PDFl10n_ass50% (2)
- Vitamin CDocument10 pagesVitamin Capi-308025929No ratings yet
- SE) During The Low-Protein To 5.4 0.4 Mmol/d During The High-Protein Diet)Document10 pagesSE) During The Low-Protein To 5.4 0.4 Mmol/d During The High-Protein Diet)lindashikuNo ratings yet
- Chem Inv ProjDocument15 pagesChem Inv Projsundaram kvNo ratings yet
- Vitamin C and Kidney StonesDocument6 pagesVitamin C and Kidney StonesasaaguurNo ratings yet
- Sunrise Vitamins White Paper-07 14-En-AllDocument22 pagesSunrise Vitamins White Paper-07 14-En-Allapi-302657321No ratings yet
- 783.full Calcium Bioav Absorption AllenDocument26 pages783.full Calcium Bioav Absorption Allenadrip234No ratings yet
- Update On The Effects of Vitamins A, C, and E and Selenium On Carcinogenesis - Cure HunterDocument3 pagesUpdate On The Effects of Vitamins A, C, and E and Selenium On Carcinogenesis - Cure HunterUtopiaawaitsNo ratings yet
- Symposium: Prooxidant Effects of Antioxidant VitaminsDocument4 pagesSymposium: Prooxidant Effects of Antioxidant VitaminsJelena AcimovicNo ratings yet
- Laporan Vit CDocument17 pagesLaporan Vit CAinin ZahratunNo ratings yet
- Vit C ToxicityDocument6 pagesVit C ToxicityGideon MukalaziNo ratings yet
- Vitamin C - Ascorbic AcidDocument7 pagesVitamin C - Ascorbic AcidasdaNo ratings yet
- Supernutrition News: Vitamins & MineralsDocument2 pagesSupernutrition News: Vitamins & MineralsferminegroNo ratings yet
- Vitaminsfinal HamrickCountsDocument43 pagesVitaminsfinal HamrickCountsĐặng Huy HoàngNo ratings yet
- Class 12th Chemistry Project On EsDocument30 pagesClass 12th Chemistry Project On Esdan jose skNo ratings yet
- Vivek Chem PRJCTDocument29 pagesVivek Chem PRJCTkeshavjain7No ratings yet
- Vit CDocument10 pagesVit C3/2 no.34 สรัญญากร สีหาราชNo ratings yet
- 10 Chat PDFDocument10 pages10 Chat PDFWill TohallinoNo ratings yet
- Original Investigation Total, Dietary, and Supplemental Vitamin C Intake and Risk of Incident Kidney StonesDocument8 pagesOriginal Investigation Total, Dietary, and Supplemental Vitamin C Intake and Risk of Incident Kidney StonesSoloview ModelingNo ratings yet
- Calcium and Vitamin D For VegansDocument14 pagesCalcium and Vitamin D For VegansDisha TNo ratings yet
- Dr. H.L. NEWBOLD Vitamin ADocument4 pagesDr. H.L. NEWBOLD Vitamin ATEIUSANUNo ratings yet
- Vitamin C and The Common Cold.Document14 pagesVitamin C and The Common Cold.xupei386No ratings yet
- Effect of Daily Intake of Yoghurt and Bread Enriched With Biologically Active Substances On Blood Lipids and Vitamin A in Adolescents and Young AdultsDocument9 pagesEffect of Daily Intake of Yoghurt and Bread Enriched With Biologically Active Substances On Blood Lipids and Vitamin A in Adolescents and Young AdultsEsmeralda SantillanNo ratings yet
- Hypercalcemia and Metastatic Calcification: 1 Vitamin D IntoxicationDocument55 pagesHypercalcemia and Metastatic Calcification: 1 Vitamin D IntoxicationF WoyenNo ratings yet
- Pharmacokinetics of Oral Vitamin C: I, II III IVDocument25 pagesPharmacokinetics of Oral Vitamin C: I, II III IVmarkuswolf11No ratings yet
- Caffeine Bone CalciumDocument8 pagesCaffeine Bone CalciumHerpika DianaNo ratings yet
- Oxalate Intake and The Risk For Nephrolithiasis: Clinical ResearchDocument7 pagesOxalate Intake and The Risk For Nephrolithiasis: Clinical ResearchTara WandhitaNo ratings yet
- Skripsi GiziDocument95 pagesSkripsi GiziAulia Putri EvindraNo ratings yet
- Dietary Calcium Intake and Obesity: Sarina Schrager, MDDocument6 pagesDietary Calcium Intake and Obesity: Sarina Schrager, MDYenny PangaribuanNo ratings yet
- Vitamin C and Ascorbic AcidDocument33 pagesVitamin C and Ascorbic AcidKristina MilićevićNo ratings yet
- JCM 09 01616 v2Document12 pagesJCM 09 01616 v2kanishk luhachNo ratings yet
- Vitamin C For SepsisDocument3 pagesVitamin C For SepsissignaturebeatNo ratings yet
- Pharmacological MonographDocument4 pagesPharmacological MonographAlvaro CabezasNo ratings yet
- Vitamin C VC - Nz.sept.2010Document63 pagesVitamin C VC - Nz.sept.2010kishbudNo ratings yet
- K-Citrate Helps Maintain Bones in Older AdultsDocument2 pagesK-Citrate Helps Maintain Bones in Older AdultsRudolfGerNo ratings yet
- Vitamin CDocument3 pagesVitamin CMuhammad Haziq Fikri Bin Mohd Nazri J22A0134No ratings yet
- 6 - J PerinetalDocument6 pages6 - J PerinetaltaimoursultanNo ratings yet
- What To Know About Nitric Oxide SupplementsDocument6 pagesWhat To Know About Nitric Oxide SupplementsJhon Edinson Cabezas RodriguezNo ratings yet
- Vitamin C Supplements Review & Top PicksDocument21 pagesVitamin C Supplements Review & Top Picksmonjia.ridhaNo ratings yet
- Why and How To Implement SodiumDocument10 pagesWhy and How To Implement SodiumAdriana MadeiraNo ratings yet
- Sacn Iron and Health Report WebDocument374 pagesSacn Iron and Health Report WebwaitNo ratings yet
- Association of Kidney Stone Disease With Dietary FactorsDocument10 pagesAssociation of Kidney Stone Disease With Dietary Factorsrashid nuñezNo ratings yet
- 2017 Changes in Urinary Risk Profile After Shortterm Low Sodium and Low Calcium Diet inDocument9 pages2017 Changes in Urinary Risk Profile After Shortterm Low Sodium and Low Calcium Diet inNayaNo ratings yet
- Effect of Vitamin C On Malondialdehyde (Mda) in Pregnant Nigerian WomenDocument4 pagesEffect of Vitamin C On Malondialdehyde (Mda) in Pregnant Nigerian WomenocadaNo ratings yet
- Stroke.: Nutrition and Stroke PreventionDocument7 pagesStroke.: Nutrition and Stroke Preventionrandey92No ratings yet
- The Role of Micronutrients in Managing DiabetesDocument5 pagesThe Role of Micronutrients in Managing DiabetesYasmin Katherin HuillcaNo ratings yet
- Nihms 572580Document13 pagesNihms 572580Sina AryaNo ratings yet
- Tugas Metodelogi PenelitianDocument3 pagesTugas Metodelogi PenelitianlinidesfikaNo ratings yet
- Alimentatia Pacientului LitiazicDocument92 pagesAlimentatia Pacientului LitiazicRosca MarcelNo ratings yet
- Dietary Intake, Blood Pressure and Osteoporosis: Original ArticleDocument5 pagesDietary Intake, Blood Pressure and Osteoporosis: Original ArticleCorin Boice TelloNo ratings yet
- Hemochromatosis PDFDocument9 pagesHemochromatosis PDFMelotNo ratings yet
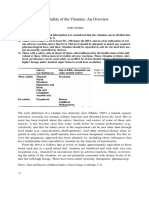
- The Safety of The Vitamins An OverviewDocument7 pagesThe Safety of The Vitamins An OverviewMonica CiorneiNo ratings yet
- Module 4 Reading Materials (Supplementary)Document4 pagesModule 4 Reading Materials (Supplementary)Luis MunozNo ratings yet
- In The Clinic: Prevention and Screening Diagnosis Treatment Practice Improvement CME QuestionsDocument16 pagesIn The Clinic: Prevention and Screening Diagnosis Treatment Practice Improvement CME QuestionsewbNo ratings yet
- Vitamin C in Disease Prevention and Cure: An OverviewDocument15 pagesVitamin C in Disease Prevention and Cure: An Overviewfpm5948No ratings yet
- In-Vitro Anti-Urolithiatic Activity of Some Yemeni Medicinal Plants ExtractsDocument12 pagesIn-Vitro Anti-Urolithiatic Activity of Some Yemeni Medicinal Plants ExtractsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Glutathione: The Secret Antioxidant To Prevent Cancer, Aging, Dementia, And Heart DiseaseFrom EverandGlutathione: The Secret Antioxidant To Prevent Cancer, Aging, Dementia, And Heart DiseaseRating: 5 out of 5 stars5/5 (2)
- Plant - Based Milk NewDocument26 pagesPlant - Based Milk NewCARMELA LOLONGNo ratings yet
- Awareness Usage and Perception of Food Supplements PDFDocument9 pagesAwareness Usage and Perception of Food Supplements PDFGerlyn Lariosa Pag-ongNo ratings yet
- RabbitDocument32 pagesRabbitVetz clubNo ratings yet
- Pica PosterDocument1 pagePica Posterapi-273262206No ratings yet
- K To 12 AdvocacyDocument49 pagesK To 12 Advocacyjefferson pabloNo ratings yet
- UNICEF Nutrition Strategy 2020-2030Document110 pagesUNICEF Nutrition Strategy 2020-2030jacob100% (1)
- African Cuisine: Laboratory ExerciseDocument6 pagesAfrican Cuisine: Laboratory ExerciseVincalaine BalagotNo ratings yet
- AAP-Anaemia - Clinical Report-Diagnosis and Prevention of IronDocument13 pagesAAP-Anaemia - Clinical Report-Diagnosis and Prevention of Irondesai2kNo ratings yet
- E020167 FullDocument14 pagesE020167 FullDewi KilisuciNo ratings yet
- Develop A Business PlanDocument8 pagesDevelop A Business Planmolinatherabbit20No ratings yet
- Inmed Animal Health - XLSX SheetDocument27 pagesInmed Animal Health - XLSX SheetInmed AnimalNo ratings yet
- KFC Nutrition PDFDocument4 pagesKFC Nutrition PDFJody Ike LinerNo ratings yet
- Nutrition For RowingDocument113 pagesNutrition For RowingDarren MooreNo ratings yet
- FREE BARE Guide Taste Tester PDFDocument19 pagesFREE BARE Guide Taste Tester PDFOnny EllyNo ratings yet
- CHILDHOOD Nutrition in The Life CycleDocument38 pagesCHILDHOOD Nutrition in The Life Cyclerenz bartolomeNo ratings yet
- Smoothie Ebook v2Document79 pagesSmoothie Ebook v2Rodrigo RodriguesNo ratings yet
- The Tale of Angus Barbieri Who Fasted For More Than A Year - and Lost 21 Stone - Evening TelegraphDocument5 pagesThe Tale of Angus Barbieri Who Fasted For More Than A Year - and Lost 21 Stone - Evening TelegraphRobert Sullivan100% (1)
- Pre and PostDocument10 pagesPre and PostS SPEEDNo ratings yet
- Chapter 8 and 9 - Bread Making 2021Document29 pagesChapter 8 and 9 - Bread Making 2021Ain Natasya ZulfikreeNo ratings yet
- ConceptpaperDocument6 pagesConceptpaperDale LopezNo ratings yet
- Malaysia Isagenix TrainingDocument97 pagesMalaysia Isagenix TrainingMuaz YaidNo ratings yet
- NCSCDocument3 pagesNCSCMihirNo ratings yet
- By Lorenzo Pansini: Home: CorrespondenceDocument24 pagesBy Lorenzo Pansini: Home: CorrespondenceĐạt NguyễnNo ratings yet
- Project ProposalDocument2 pagesProject ProposalRosela Mae BaracaoNo ratings yet
- Nutr 335 Adime NoteDocument2 pagesNutr 335 Adime Noteapi-533845626No ratings yet
- MineralsDocument9 pagesMineralsDerek AtienzaNo ratings yet
- 3-MNIYCN DF - Nutritional Guidelines and IYCF Strategic Plan - 11sept2020Document19 pages3-MNIYCN DF - Nutritional Guidelines and IYCF Strategic Plan - 11sept2020d6smvtzjnbNo ratings yet
- Biological Molecules Assignment Worksheet: Due Date: 20/06/21Document11 pagesBiological Molecules Assignment Worksheet: Due Date: 20/06/21JS ManishNo ratings yet