Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5835)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Medication Template PrednisoneDocument5 pagesMedication Template PrednisoneJudith MeranvilNo ratings yet
- Active Cycle Breathing TechniqueDocument20 pagesActive Cycle Breathing TechniqueRAM100% (2)
- Efficacy of Steroidal Vs Non-Steroidal Agents in Oral Lichen Planus: A Randomised, Open-Label StudyDocument9 pagesEfficacy of Steroidal Vs Non-Steroidal Agents in Oral Lichen Planus: A Randomised, Open-Label StudyRetno ManggalihNo ratings yet
- Chung 2014Document6 pagesChung 2014Retno ManggalihNo ratings yet
- Migraine and Body Mass Index Categories: A Systematic Review and Meta-Analysis of Observational StudiesDocument14 pagesMigraine and Body Mass Index Categories: A Systematic Review and Meta-Analysis of Observational StudiesRetno ManggalihNo ratings yet
- 679 1364 1 SMDocument5 pages679 1364 1 SMRetno ManggalihNo ratings yet
- Houston2014Document5 pagesHouston2014Retno ManggalihNo ratings yet
- Extrapulmonary Tuberculosis: Key PointsDocument6 pagesExtrapulmonary Tuberculosis: Key PointsRetno ManggalihNo ratings yet
- J Gerontol A Biol Sci Med Sci-1997-Vitiello-M189-91Document3 pagesJ Gerontol A Biol Sci Med Sci-1997-Vitiello-M189-91Retno ManggalihNo ratings yet
- Kuesioner Kualitas HidupDocument9 pagesKuesioner Kualitas HidupRetno ManggalihNo ratings yet
- 1-Panadol Advance 6-Panadol Sinus 2-Panadol Extra 7-Panadol Night 3-Panadol Actifast 4-Panadol Joint 5-Panadol Cold and Flu and Their TypesDocument12 pages1-Panadol Advance 6-Panadol Sinus 2-Panadol Extra 7-Panadol Night 3-Panadol Actifast 4-Panadol Joint 5-Panadol Cold and Flu and Their TypesSulaiman AlqatfNo ratings yet
- 1628 6995 3 PBDocument32 pages1628 6995 3 PBPelayanan Tahanan Rutan KendariNo ratings yet
- Dilation and Evacuation (D&E)Document1 pageDilation and Evacuation (D&E)Rachel SissonNo ratings yet
- Betarie Anum Almira - RMIK (A) - Praktik KSPK 8Document9 pagesBetarie Anum Almira - RMIK (A) - Praktik KSPK 8Betarie Anum AlmiraNo ratings yet
- Telemetry Recognition WorkbookDocument29 pagesTelemetry Recognition WorkbookQueenNo ratings yet
- Service Learning Impact ReportDocument10 pagesService Learning Impact ReportLeisha J RohanNo ratings yet
- Aspectos Importantes de La Nutrición en Niños Con CáncerDocument11 pagesAspectos Importantes de La Nutrición en Niños Con CáncerNadia DonosoNo ratings yet
- LabyrinthitisDocument7 pagesLabyrinthitisChristie ZamoraNo ratings yet
- Attention Deficit/ Hyperactivity Disorder: Changes To The DisorderDocument2 pagesAttention Deficit/ Hyperactivity Disorder: Changes To The DisorderGemanDuenasNo ratings yet
- Emskfjek-Intravenous IV Fluid Prescribing in AdultsDocument14 pagesEmskfjek-Intravenous IV Fluid Prescribing in AdultsAli SemajNo ratings yet
- Durolane BV Physician Brochure 2013 EnglishDocument2 pagesDurolane BV Physician Brochure 2013 EnglishJohn BeveridgeNo ratings yet
- Hematology Terms and DefinitionsDocument9 pagesHematology Terms and DefinitionsLovely B. AlipatNo ratings yet
- What Is HypothermiaDocument4 pagesWhat Is HypothermiaSulin CruzNo ratings yet
- Atopic DermatitisDocument26 pagesAtopic DermatitisninarizkiNo ratings yet
- First Aid Part 2Document34 pagesFirst Aid Part 2teachkhimNo ratings yet
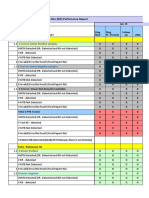
- GeneXpert - Monthly - Report - JAN, FEB, MARCH 2019 (GIMS) GAMBAT)Document12 pagesGeneXpert - Monthly - Report - JAN, FEB, MARCH 2019 (GIMS) GAMBAT)shakeelNo ratings yet
- Case ApplicationDocument2 pagesCase ApplicationRed Angela DinsonNo ratings yet
- Nystagmus: Dr. Enny Lestari, M. Biomed, SP.SDocument39 pagesNystagmus: Dr. Enny Lestari, M. Biomed, SP.SPuji Yunisyah100% (1)
- Acute Complications of Diabetes MellitusDocument1 pageAcute Complications of Diabetes MellitusGerardLum100% (1)
- Basic Principles of Wound MGMT - Poengki DP-ilovepdf-compressedDocument38 pagesBasic Principles of Wound MGMT - Poengki DP-ilovepdf-compressednugrahaNo ratings yet
- Heat Tolerance Test PDFDocument7 pagesHeat Tolerance Test PDFMonica LapusNo ratings yet
- Gastritis and Peptic UlcerDocument30 pagesGastritis and Peptic UlcerKareem DawoodNo ratings yet
- DHQ Flowcharts v2 1 Prep Pep ArtDocument49 pagesDHQ Flowcharts v2 1 Prep Pep ArtNatasha MendozaNo ratings yet
- The Graviola Tree - Cancer KillerDocument5 pagesThe Graviola Tree - Cancer KillerdeejayNo ratings yet
- Influenza FormDocument2 pagesInfluenza FormDipendra PoudelNo ratings yet
- Chapter 20 With Comments - Acinetobacter - StenotrophomonasDocument13 pagesChapter 20 With Comments - Acinetobacter - StenotrophomonasGordon JamesonNo ratings yet
- HomicideDocument22 pagesHomicideniraj_sdNo ratings yet
- Daily UrduDocument4 pagesDaily UrduFurqanAftabNo ratings yet