Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5825)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- LVAD in An Hbo2 ChamberDocument5 pagesLVAD in An Hbo2 ChamberTony LeeNo ratings yet
- The Imitation GameDocument3 pagesThe Imitation GameLuis AlbertoNo ratings yet
- Naruto Shinden - Volume 02 - Itachi Shinden - Book of Midnight (VIZ) (CalibreV1DPC)Document178 pagesNaruto Shinden - Volume 02 - Itachi Shinden - Book of Midnight (VIZ) (CalibreV1DPC)Arno LexhardeNo ratings yet
- Anchors Away Sheet MusicDocument6 pagesAnchors Away Sheet MusicAngelo Pizarro100% (1)
- TID 164 A Steam Tug EbookDocument73 pagesTID 164 A Steam Tug Ebookmhammer_18100% (1)
- Convoy OperationsDocument20 pagesConvoy OperationsJacob MayoNo ratings yet
- Patton's Best RulesDocument20 pagesPatton's Best RulesMark Goss100% (2)
- Topical Oxygen Wound TherapyDocument9 pagesTopical Oxygen Wound TherapyTony LeeNo ratings yet
- Air Vs Oxygen in STEMPDocument8 pagesAir Vs Oxygen in STEMPTony LeeNo ratings yet
- Lactate Accumulation in Apneic SportsDocument9 pagesLactate Accumulation in Apneic SportsTony LeeNo ratings yet
- Hbo2 Abt SystemDocument7 pagesHbo2 Abt SystemTony LeeNo ratings yet
- Hbo2 and RedoxDocument9 pagesHbo2 and RedoxTony LeeNo ratings yet
- Transcutaneous Oximetry in Clin Practice - ConsensusDocument11 pagesTranscutaneous Oximetry in Clin Practice - ConsensusTony LeeNo ratings yet
- Waist Hip Ratio or CV RiskDocument1 pageWaist Hip Ratio or CV RiskTony LeeNo ratings yet
- WarriorDocument5 pagesWarriorluizquitoNo ratings yet
- Te Rise andDocument5 pagesTe Rise andEd ParnovNo ratings yet
- Director VP Business Development Capture Proposal Manager Resume in Washington DC VA MD - Zack SionakidesDocument3 pagesDirector VP Business Development Capture Proposal Manager Resume in Washington DC VA MD - Zack SionakidesZack SionakidesNo ratings yet
- 33 Conspiracy Theories That Turned Out To Be True-TheGlobalElite - Org-22Document22 pages33 Conspiracy Theories That Turned Out To Be True-TheGlobalElite - Org-22Keith Knight100% (3)
- Blitzscales 11 PDFDocument78 pagesBlitzscales 11 PDFMarkus Fabke100% (4)
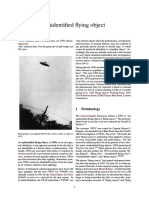
- Unidentified Flying ObjectDocument23 pagesUnidentified Flying Objecttheox2No ratings yet
- Fort Bliss HistoryDocument122 pagesFort Bliss HistoryCAP History LibraryNo ratings yet
- 120 150 PDFDocument30 pages120 150 PDFraoufluck4520No ratings yet
- Sinhala PB G-5Document144 pagesSinhala PB G-5Chamari PriyangikaNo ratings yet
- Warmachine - SuperiorityDocument209 pagesWarmachine - SuperiorityJimmy83% (6)
- Military Honours Committee 3Document16 pagesMilitary Honours Committee 3diethawkNo ratings yet
- 6 - EvansMichael - The Case Against MegacitiesDocument12 pages6 - EvansMichael - The Case Against MegacitiesMichele GiulianiNo ratings yet
- Mughal Emperor: Din-PanahDocument1 pageMughal Emperor: Din-PanahGul12No ratings yet
- Instructor: Capt Ab Respicio PN (GSC) Ret Former Deputy Commander Naval Construction BrigadeDocument21 pagesInstructor: Capt Ab Respicio PN (GSC) Ret Former Deputy Commander Naval Construction BrigademmabeeNo ratings yet
- Shire (Middle-Earth Strategy Battle Game) (83 Warriors, 800 Points, 21 Bow)Document8 pagesShire (Middle-Earth Strategy Battle Game) (83 Warriors, 800 Points, 21 Bow)Cyclone GrizzlyNo ratings yet
- $15 Mil To Idps in 2008: Dili WeeklyDocument20 pages$15 Mil To Idps in 2008: Dili WeeklyInternational Center for Journalists100% (3)
- Adeptus Arbites MMVIII 0711 Warhammer 40k 2nd EditionDocument32 pagesAdeptus Arbites MMVIII 0711 Warhammer 40k 2nd EditionJason Lark100% (2)
- Secretly Chipped ManDocument5 pagesSecretly Chipped Mandarius3777No ratings yet
- Marines at WarDocument260 pagesMarines at Warscribd userNo ratings yet
- Anger and HumiliationDocument3 pagesAnger and Humiliationapi-236492165No ratings yet
- Mil STD 45662aDocument13 pagesMil STD 45662askomlenNo ratings yet
- Review 130718Document5 pagesReview 130718ajayNo ratings yet
- Wars of The Roses - 2018-04-01 PDFDocument148 pagesWars of The Roses - 2018-04-01 PDFHallam Davis88% (8)
- BRAVO Chassis For Howa Installation InstructionsDocument2 pagesBRAVO Chassis For Howa Installation InstructionsDan WeaverNo ratings yet