
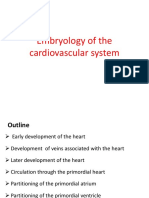
Conduction System of The Heart
Conduction System of The Heart
You might also like
- A. Cardiac Cycle: 1. Atrial Systole (Contraction of Atria) - 0.1sDocument6 pagesA. Cardiac Cycle: 1. Atrial Systole (Contraction of Atria) - 0.1sjasper haiNo ratings yet
- Embryology of Heart Year 2Document55 pagesEmbryology of Heart Year 2Amanuel MaruNo ratings yet
- Coarctation of The AortaDocument2 pagesCoarctation of The AortaDavid Cheng0% (1)
- Wind Tunnel Lab SafetyDocument2 pagesWind Tunnel Lab SafetyZ-B67% (3)
- Anatomy and Physiology of Blood VesselDocument3 pagesAnatomy and Physiology of Blood Vesselneleh grayNo ratings yet
- Cardiac CycleDocument12 pagesCardiac Cycleanupam manu100% (1)
- The Coronary CirculationDocument12 pagesThe Coronary CirculationJulia PutnikNo ratings yet
- Anatomy Heart and Great VesselsDocument54 pagesAnatomy Heart and Great VesselsRaviNo ratings yet
- Notes in Physiology 2nd PDFDocument37 pagesNotes in Physiology 2nd PDFDany SamuelNo ratings yet
- CARDIAC CYCLE - Part I PDFDocument55 pagesCARDIAC CYCLE - Part I PDFChirag Dagar100% (1)
- 05 Cardiovascular System PhysiologyDocument34 pages05 Cardiovascular System PhysiologyKaye Alyssa EnriquezNo ratings yet
- Cardiac Cycle - DR Rakesh JainDocument97 pagesCardiac Cycle - DR Rakesh JainEmmieNo ratings yet
- Respiratory PhysiologyDocument30 pagesRespiratory PhysiologyBarbara Sakura RiawanNo ratings yet
- Final Anatomy Exam Questions PRE MED: Yara AdeebDocument3 pagesFinal Anatomy Exam Questions PRE MED: Yara AdeebMadani TawfeeqNo ratings yet
- Physiology of RespirationDocument2 pagesPhysiology of RespirationIOSRjournalNo ratings yet
- Physiology of Heart in DetailDocument101 pagesPhysiology of Heart in Detailakanksha sharmaNo ratings yet
- Arterial Blood PressureDocument46 pagesArterial Blood PressureRupasi KathiravanNo ratings yet
- Lecture On Basics of ECG For 1st Year MBBS by Dr. RoomiDocument28 pagesLecture On Basics of ECG For 1st Year MBBS by Dr. RoomiMudassar Roomi100% (3)
- Cardiac CycleDocument31 pagesCardiac CycleAdwaitha KrNo ratings yet
- Cardiac Cycle: Prepared By: Mineshkumar Prajapati Roll No: 05 Biomedical Science (2021-22)Document21 pagesCardiac Cycle: Prepared By: Mineshkumar Prajapati Roll No: 05 Biomedical Science (2021-22)minesh prajapatiNo ratings yet
- Chapter - 036 Arrhythmias ClassDocument129 pagesChapter - 036 Arrhythmias ClassWisdomIsMiseryNo ratings yet
- Histology of LungsDocument30 pagesHistology of LungsShahir21No ratings yet
- Cardiovascular Examination:: General InspectionDocument6 pagesCardiovascular Examination:: General InspectionPhysician AssociateNo ratings yet
- Heart Muscle: The Heart As A Pump and FunctionDocument4 pagesHeart Muscle: The Heart As A Pump and Functionmcwnotes100% (1)
- Pulmonary CirculationDocument16 pagesPulmonary Circulationsajid_saiyad0% (1)
- Cardiac OutputDocument31 pagesCardiac OutputanojNo ratings yet
- Physiology - Rhythmical Excitation of Heart by Dr. Mudassar Ali RoomiDocument18 pagesPhysiology - Rhythmical Excitation of Heart by Dr. Mudassar Ali RoomiMudassar Roomi100% (2)
- Valvular Heart Disease 2Document46 pagesValvular Heart Disease 2Topea BogdanNo ratings yet
- Physiology of The Cardiovascular System-CVSDocument56 pagesPhysiology of The Cardiovascular System-CVSAmanuel MaruNo ratings yet
- Lecture 3 Cardiovascular System 1Document54 pagesLecture 3 Cardiovascular System 1hafiz patah100% (1)
- Describe The Factors Affecting Cardiac OutputDocument6 pagesDescribe The Factors Affecting Cardiac OutputSis SukarnoNo ratings yet
- L3,4-Cardiac Cycle Mcqs Fre, XBN.DDocument7 pagesL3,4-Cardiac Cycle Mcqs Fre, XBN.DsajidNo ratings yet
- Lungs PDFDocument47 pagesLungs PDFAmna YousafNo ratings yet
- ECGDocument33 pagesECGTamia PutriNo ratings yet
- Key of SEQs Heart, Nerve and Muscle Revision TestDocument11 pagesKey of SEQs Heart, Nerve and Muscle Revision TestMudassar Roomi100% (2)
- Respiratory Physiology NoteDocument19 pagesRespiratory Physiology NotePeter Wong0% (1)
- Chapter 22 Notes Respiratory SystemDocument36 pagesChapter 22 Notes Respiratory SystemMarilia BonorinoNo ratings yet
- CVS Lect 6 Blood Pressure, PathophysiologyDocument13 pagesCVS Lect 6 Blood Pressure, PathophysiologySherwan R Shal100% (5)
- Tissues 4Document65 pagesTissues 4marianisie448100% (3)
- FBC Interpretation and Function of Blood ComponentsDocument7 pagesFBC Interpretation and Function of Blood ComponentsFrancesca LiNo ratings yet
- General Exam and Q&A For MBBS DR ShamolDocument320 pagesGeneral Exam and Q&A For MBBS DR Shamolmaybe100% (3)
- Circulatory System - Part 2 4-8-14 For BBDocument23 pagesCirculatory System - Part 2 4-8-14 For BBroman7dbNo ratings yet
- Cardiovascular SystemDocument22 pagesCardiovascular SystemAyu Yunita Jaury HR100% (1)
- Cardiac OutputDocument4 pagesCardiac OutputJubin JainNo ratings yet
- Anatomy of Cardiovascular SystemDocument23 pagesAnatomy of Cardiovascular SystemElvira Wisakhadewi100% (1)
- Quiz - Development of Human Cardiovascular SystemDocument7 pagesQuiz - Development of Human Cardiovascular Systemlucky mbaselaNo ratings yet
- Topic - Composition of BloodDocument18 pagesTopic - Composition of BloodChhavi SainiNo ratings yet
- DLC PracticalDocument6 pagesDLC PracticalAngoruz Gohain BaruahNo ratings yet
- Anatomy, Lecture 6, Pericardium and The Heart (Slides)Document22 pagesAnatomy, Lecture 6, Pericardium and The Heart (Slides)Ali Al-Qudsi100% (1)
- Valvular Heart DiseaseDocument71 pagesValvular Heart DiseaseChadi Alraies100% (9)
- Intro Head and NeckDocument74 pagesIntro Head and NeckAuza Moses Ibrahim100% (2)
- Cardiac CycleDocument30 pagesCardiac CycleCarrine Liew100% (2)
- Clinical Anatomy of ThoraxDocument4 pagesClinical Anatomy of ThoraxCeo MedCom100% (1)
- Cardiac Cycle FinalDocument37 pagesCardiac Cycle Finalindra_jeet2009No ratings yet
- Physiology Practical Measurement of Blood PressureDocument6 pagesPhysiology Practical Measurement of Blood PressureAli MohamedNo ratings yet
- Upper Extremities Ortho SG3Document119 pagesUpper Extremities Ortho SG3Nuhu Bankwhot100% (1)
- Cardiac CycleDocument38 pagesCardiac CycleKok HoongNo ratings yet
- Anatomy & Function of Conducting SystemDocument22 pagesAnatomy & Function of Conducting SystemhalayehiahNo ratings yet
- RRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRDocument2 pagesRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRSaginesh MkNo ratings yet
- Notes 231213 134139-1Document14 pagesNotes 231213 134139-1idlydumpfvckNo ratings yet
- Final DraftDocument5 pagesFinal Draftapi-451064930No ratings yet
- Mix Design C 35A - 50%Document1 pageMix Design C 35A - 50%cecbNo ratings yet
- 1the Bean Bar 1-8Document62 pages1the Bean Bar 1-8Rey Mart PerezNo ratings yet
- FYP-I Report-Hybrid Electric VehicleDocument35 pagesFYP-I Report-Hybrid Electric VehicleM UsamaNo ratings yet
- PED 5 Heat ExchangersDocument74 pagesPED 5 Heat ExchangersDiogo EstevesNo ratings yet
- Why Integration Is The Key To Asia's Economic Progress? Explain Your AnswerDocument2 pagesWhy Integration Is The Key To Asia's Economic Progress? Explain Your AnswerQueeny JavierNo ratings yet
- Diseases of Lungs BLACKWOODDocument360 pagesDiseases of Lungs BLACKWOODG AnshuNo ratings yet
- Business Ethics ANSWERSDocument3 pagesBusiness Ethics ANSWERSMỹ HàNo ratings yet
- ELEMAN HSEMS - Safety Management System PDFDocument64 pagesELEMAN HSEMS - Safety Management System PDFZafar SiddiquiNo ratings yet
- Graduate Programs and CoursesDocument75 pagesGraduate Programs and CoursesDarwin Aldas BasquialNo ratings yet
- Farmakologi Dan Toksikologi 2022Document25 pagesFarmakologi Dan Toksikologi 2022Ghost TsushimaNo ratings yet
- 16HP Operators ManualDocument40 pages16HP Operators ManualPaul ArguinNo ratings yet
- Test Bank For Williams Basic Nutrition and Diet Therapy 14th Edition Staci NixDocument24 pagesTest Bank For Williams Basic Nutrition and Diet Therapy 14th Edition Staci Nixdavidjonescrjeagtnwp100% (38)
- Operator's Manual: Hydril K20-5000 Pulsation Dampener IAW PED 97/23/ECDocument16 pagesOperator's Manual: Hydril K20-5000 Pulsation Dampener IAW PED 97/23/ECAli Ali67% (3)
- MSSL Annual Report 19 20Document427 pagesMSSL Annual Report 19 20gayatri suryakanthanNo ratings yet
- Orif ReportDocument5 pagesOrif ReportduypalaNo ratings yet
- Yasnac J300 Connecting Manual (Type B)Document186 pagesYasnac J300 Connecting Manual (Type B)sunhuynh100% (1)
- Boundary Line: Plan of Gpuff Temporary JettyDocument1 pageBoundary Line: Plan of Gpuff Temporary Jettyshafiq_05No ratings yet
- 2021, Schuhmacher - Big Techs and Startups in Pharmaceutical R&D - A 2020 Perspective On Artificial IntelligenceDocument6 pages2021, Schuhmacher - Big Techs and Startups in Pharmaceutical R&D - A 2020 Perspective On Artificial Intelligencejeffrey EellisNo ratings yet
- d000523 Doseuse RemplisseuseDocument2 pagesd000523 Doseuse RemplisseuseEnzo QuatremareNo ratings yet
- Repair Processes of Experimental Root Fractures in Rat Molars Examined by Histopathological Techniques and 3D Micro-CT ImagingDocument8 pagesRepair Processes of Experimental Root Fractures in Rat Molars Examined by Histopathological Techniques and 3D Micro-CT ImagingAhmad Ulil AlbabNo ratings yet
- Crab Lab ReportDocument2 pagesCrab Lab Reportapi-397859183No ratings yet
- Writing Task 2Document50 pagesWriting Task 2Khanh Chi Pham100% (1)
- R410A Aqua Tempo Super Series Air Cooled Scroll Chiller Technical ManualDocument172 pagesR410A Aqua Tempo Super Series Air Cooled Scroll Chiller Technical ManualJuan Imas Del PuertoNo ratings yet
- Lab Manual Separation Tech Jan 2021Document43 pagesLab Manual Separation Tech Jan 2021Abdul QayyumNo ratings yet
- Minimum Wages CAE EssayDocument1 pageMinimum Wages CAE EssayAmalia SereaNo ratings yet
- English SentencesDocument27 pagesEnglish Sentencesvarkriszti100% (2)
- IFAS System Troubleshooting Guide DraftDocument18 pagesIFAS System Troubleshooting Guide Draftsoumya pattanaikNo ratings yet
- KatalogDocument3 pagesKatalogJosua Sahat Parulian SinagaNo ratings yet
























































































Download as docx, pdf, or txt
You might also like
- A. Cardiac Cycle: 1. Atrial Systole (Contraction of Atria) - 0.1sDocument6 pagesA. Cardiac Cycle: 1. Atrial Systole (Contraction of Atria) - 0.1sjasper haiNo ratings yet
- Embryology of Heart Year 2Document55 pagesEmbryology of Heart Year 2Amanuel MaruNo ratings yet
- Coarctation of The AortaDocument2 pagesCoarctation of The AortaDavid Cheng0% (1)
- Wind Tunnel Lab SafetyDocument2 pagesWind Tunnel Lab SafetyZ-B67% (3)
- Anatomy and Physiology of Blood VesselDocument3 pagesAnatomy and Physiology of Blood Vesselneleh grayNo ratings yet
- Cardiac CycleDocument12 pagesCardiac Cycleanupam manu100% (1)
- The Coronary CirculationDocument12 pagesThe Coronary CirculationJulia PutnikNo ratings yet
- Anatomy Heart and Great VesselsDocument54 pagesAnatomy Heart and Great VesselsRaviNo ratings yet
- Notes in Physiology 2nd PDFDocument37 pagesNotes in Physiology 2nd PDFDany SamuelNo ratings yet
- CARDIAC CYCLE - Part I PDFDocument55 pagesCARDIAC CYCLE - Part I PDFChirag Dagar100% (1)
- 05 Cardiovascular System PhysiologyDocument34 pages05 Cardiovascular System PhysiologyKaye Alyssa EnriquezNo ratings yet
- Cardiac Cycle - DR Rakesh JainDocument97 pagesCardiac Cycle - DR Rakesh JainEmmieNo ratings yet
- Respiratory PhysiologyDocument30 pagesRespiratory PhysiologyBarbara Sakura RiawanNo ratings yet
- Final Anatomy Exam Questions PRE MED: Yara AdeebDocument3 pagesFinal Anatomy Exam Questions PRE MED: Yara AdeebMadani TawfeeqNo ratings yet
- Physiology of RespirationDocument2 pagesPhysiology of RespirationIOSRjournalNo ratings yet
- Physiology of Heart in DetailDocument101 pagesPhysiology of Heart in Detailakanksha sharmaNo ratings yet
- Arterial Blood PressureDocument46 pagesArterial Blood PressureRupasi KathiravanNo ratings yet
- Lecture On Basics of ECG For 1st Year MBBS by Dr. RoomiDocument28 pagesLecture On Basics of ECG For 1st Year MBBS by Dr. RoomiMudassar Roomi100% (3)
- Cardiac CycleDocument31 pagesCardiac CycleAdwaitha KrNo ratings yet
- Cardiac Cycle: Prepared By: Mineshkumar Prajapati Roll No: 05 Biomedical Science (2021-22)Document21 pagesCardiac Cycle: Prepared By: Mineshkumar Prajapati Roll No: 05 Biomedical Science (2021-22)minesh prajapatiNo ratings yet
- Chapter - 036 Arrhythmias ClassDocument129 pagesChapter - 036 Arrhythmias ClassWisdomIsMiseryNo ratings yet
- Histology of LungsDocument30 pagesHistology of LungsShahir21No ratings yet
- Cardiovascular Examination:: General InspectionDocument6 pagesCardiovascular Examination:: General InspectionPhysician AssociateNo ratings yet
- Heart Muscle: The Heart As A Pump and FunctionDocument4 pagesHeart Muscle: The Heart As A Pump and Functionmcwnotes100% (1)
- Pulmonary CirculationDocument16 pagesPulmonary Circulationsajid_saiyad0% (1)
- Cardiac OutputDocument31 pagesCardiac OutputanojNo ratings yet
- Physiology - Rhythmical Excitation of Heart by Dr. Mudassar Ali RoomiDocument18 pagesPhysiology - Rhythmical Excitation of Heart by Dr. Mudassar Ali RoomiMudassar Roomi100% (2)
- Valvular Heart Disease 2Document46 pagesValvular Heart Disease 2Topea BogdanNo ratings yet
- Physiology of The Cardiovascular System-CVSDocument56 pagesPhysiology of The Cardiovascular System-CVSAmanuel MaruNo ratings yet
- Lecture 3 Cardiovascular System 1Document54 pagesLecture 3 Cardiovascular System 1hafiz patah100% (1)
- Describe The Factors Affecting Cardiac OutputDocument6 pagesDescribe The Factors Affecting Cardiac OutputSis SukarnoNo ratings yet
- L3,4-Cardiac Cycle Mcqs Fre, XBN.DDocument7 pagesL3,4-Cardiac Cycle Mcqs Fre, XBN.DsajidNo ratings yet
- Lungs PDFDocument47 pagesLungs PDFAmna YousafNo ratings yet
- ECGDocument33 pagesECGTamia PutriNo ratings yet
- Key of SEQs Heart, Nerve and Muscle Revision TestDocument11 pagesKey of SEQs Heart, Nerve and Muscle Revision TestMudassar Roomi100% (2)
- Respiratory Physiology NoteDocument19 pagesRespiratory Physiology NotePeter Wong0% (1)
- Chapter 22 Notes Respiratory SystemDocument36 pagesChapter 22 Notes Respiratory SystemMarilia BonorinoNo ratings yet
- CVS Lect 6 Blood Pressure, PathophysiologyDocument13 pagesCVS Lect 6 Blood Pressure, PathophysiologySherwan R Shal100% (5)
- Tissues 4Document65 pagesTissues 4marianisie448100% (3)
- FBC Interpretation and Function of Blood ComponentsDocument7 pagesFBC Interpretation and Function of Blood ComponentsFrancesca LiNo ratings yet
- General Exam and Q&A For MBBS DR ShamolDocument320 pagesGeneral Exam and Q&A For MBBS DR Shamolmaybe100% (3)
- Circulatory System - Part 2 4-8-14 For BBDocument23 pagesCirculatory System - Part 2 4-8-14 For BBroman7dbNo ratings yet
- Cardiovascular SystemDocument22 pagesCardiovascular SystemAyu Yunita Jaury HR100% (1)
- Cardiac OutputDocument4 pagesCardiac OutputJubin JainNo ratings yet
- Anatomy of Cardiovascular SystemDocument23 pagesAnatomy of Cardiovascular SystemElvira Wisakhadewi100% (1)
- Quiz - Development of Human Cardiovascular SystemDocument7 pagesQuiz - Development of Human Cardiovascular Systemlucky mbaselaNo ratings yet
- Topic - Composition of BloodDocument18 pagesTopic - Composition of BloodChhavi SainiNo ratings yet
- DLC PracticalDocument6 pagesDLC PracticalAngoruz Gohain BaruahNo ratings yet
- Anatomy, Lecture 6, Pericardium and The Heart (Slides)Document22 pagesAnatomy, Lecture 6, Pericardium and The Heart (Slides)Ali Al-Qudsi100% (1)
- Valvular Heart DiseaseDocument71 pagesValvular Heart DiseaseChadi Alraies100% (9)
- Intro Head and NeckDocument74 pagesIntro Head and NeckAuza Moses Ibrahim100% (2)
- Cardiac CycleDocument30 pagesCardiac CycleCarrine Liew100% (2)
- Clinical Anatomy of ThoraxDocument4 pagesClinical Anatomy of ThoraxCeo MedCom100% (1)
- Cardiac Cycle FinalDocument37 pagesCardiac Cycle Finalindra_jeet2009No ratings yet
- Physiology Practical Measurement of Blood PressureDocument6 pagesPhysiology Practical Measurement of Blood PressureAli MohamedNo ratings yet
- Upper Extremities Ortho SG3Document119 pagesUpper Extremities Ortho SG3Nuhu Bankwhot100% (1)
- Cardiac CycleDocument38 pagesCardiac CycleKok HoongNo ratings yet
- Anatomy & Function of Conducting SystemDocument22 pagesAnatomy & Function of Conducting SystemhalayehiahNo ratings yet
- RRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRDocument2 pagesRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRSaginesh MkNo ratings yet
- Notes 231213 134139-1Document14 pagesNotes 231213 134139-1idlydumpfvckNo ratings yet
- Final DraftDocument5 pagesFinal Draftapi-451064930No ratings yet
- Mix Design C 35A - 50%Document1 pageMix Design C 35A - 50%cecbNo ratings yet
- 1the Bean Bar 1-8Document62 pages1the Bean Bar 1-8Rey Mart PerezNo ratings yet
- FYP-I Report-Hybrid Electric VehicleDocument35 pagesFYP-I Report-Hybrid Electric VehicleM UsamaNo ratings yet
- PED 5 Heat ExchangersDocument74 pagesPED 5 Heat ExchangersDiogo EstevesNo ratings yet
- Why Integration Is The Key To Asia's Economic Progress? Explain Your AnswerDocument2 pagesWhy Integration Is The Key To Asia's Economic Progress? Explain Your AnswerQueeny JavierNo ratings yet
- Diseases of Lungs BLACKWOODDocument360 pagesDiseases of Lungs BLACKWOODG AnshuNo ratings yet
- Business Ethics ANSWERSDocument3 pagesBusiness Ethics ANSWERSMỹ HàNo ratings yet
- ELEMAN HSEMS - Safety Management System PDFDocument64 pagesELEMAN HSEMS - Safety Management System PDFZafar SiddiquiNo ratings yet
- Graduate Programs and CoursesDocument75 pagesGraduate Programs and CoursesDarwin Aldas BasquialNo ratings yet
- Farmakologi Dan Toksikologi 2022Document25 pagesFarmakologi Dan Toksikologi 2022Ghost TsushimaNo ratings yet
- 16HP Operators ManualDocument40 pages16HP Operators ManualPaul ArguinNo ratings yet
- Test Bank For Williams Basic Nutrition and Diet Therapy 14th Edition Staci NixDocument24 pagesTest Bank For Williams Basic Nutrition and Diet Therapy 14th Edition Staci Nixdavidjonescrjeagtnwp100% (38)
- Operator's Manual: Hydril K20-5000 Pulsation Dampener IAW PED 97/23/ECDocument16 pagesOperator's Manual: Hydril K20-5000 Pulsation Dampener IAW PED 97/23/ECAli Ali67% (3)
- MSSL Annual Report 19 20Document427 pagesMSSL Annual Report 19 20gayatri suryakanthanNo ratings yet
- Orif ReportDocument5 pagesOrif ReportduypalaNo ratings yet
- Yasnac J300 Connecting Manual (Type B)Document186 pagesYasnac J300 Connecting Manual (Type B)sunhuynh100% (1)
- Boundary Line: Plan of Gpuff Temporary JettyDocument1 pageBoundary Line: Plan of Gpuff Temporary Jettyshafiq_05No ratings yet
- 2021, Schuhmacher - Big Techs and Startups in Pharmaceutical R&D - A 2020 Perspective On Artificial IntelligenceDocument6 pages2021, Schuhmacher - Big Techs and Startups in Pharmaceutical R&D - A 2020 Perspective On Artificial Intelligencejeffrey EellisNo ratings yet
- d000523 Doseuse RemplisseuseDocument2 pagesd000523 Doseuse RemplisseuseEnzo QuatremareNo ratings yet
- Repair Processes of Experimental Root Fractures in Rat Molars Examined by Histopathological Techniques and 3D Micro-CT ImagingDocument8 pagesRepair Processes of Experimental Root Fractures in Rat Molars Examined by Histopathological Techniques and 3D Micro-CT ImagingAhmad Ulil AlbabNo ratings yet
- Crab Lab ReportDocument2 pagesCrab Lab Reportapi-397859183No ratings yet
- Writing Task 2Document50 pagesWriting Task 2Khanh Chi Pham100% (1)
- R410A Aqua Tempo Super Series Air Cooled Scroll Chiller Technical ManualDocument172 pagesR410A Aqua Tempo Super Series Air Cooled Scroll Chiller Technical ManualJuan Imas Del PuertoNo ratings yet
- Lab Manual Separation Tech Jan 2021Document43 pagesLab Manual Separation Tech Jan 2021Abdul QayyumNo ratings yet
- Minimum Wages CAE EssayDocument1 pageMinimum Wages CAE EssayAmalia SereaNo ratings yet
- English SentencesDocument27 pagesEnglish Sentencesvarkriszti100% (2)
- IFAS System Troubleshooting Guide DraftDocument18 pagesIFAS System Troubleshooting Guide Draftsoumya pattanaikNo ratings yet
- KatalogDocument3 pagesKatalogJosua Sahat Parulian SinagaNo ratings yet