Download as pdf or txt
You might also like
- Atlas of Oculoplastic and Orbital SurgeryDocument336 pagesAtlas of Oculoplastic and Orbital Surgerymelati100% (3)
- Traumatic Brain InjuryDocument23 pagesTraumatic Brain InjuryRisal WintokoNo ratings yet
- Infant Breastfeeding Assessment Tool (IBFAT)Document1 pageInfant Breastfeeding Assessment Tool (IBFAT)Sena Kawawura100% (1)
- Salbutamol Drug SummDocument1 pageSalbutamol Drug SummWarren100% (2)
- Hasper 2012Document4 pagesHasper 2012marcelo.lacknerNo ratings yet
- Neu 2013 3197Document8 pagesNeu 2013 3197Sri MarniantiNo ratings yet
- 2022 - Temperature Management in The ICUDocument10 pages2022 - Temperature Management in The ICUQui Nguyen MinhNo ratings yet
- Hyerion Trial en Arresto Cardiaco HipotermiaDocument11 pagesHyerion Trial en Arresto Cardiaco HipotermiagomsuiNo ratings yet
- Philips InnerCool Product BrochureDocument8 pagesPhilips InnerCool Product BrochurephilipsinnercoolNo ratings yet
- 2022 - 04-IVTM - Introduction - SMART Medical - RomaniaDocument27 pages2022 - 04-IVTM - Introduction - SMART Medical - RomaniaMaryNo ratings yet
- Surface Cooling MendeleyDocument19 pagesSurface Cooling MendeleyYudi BorneoNo ratings yet
- Hyperthermia in The Forty Eight Hours After.6Document7 pagesHyperthermia in The Forty Eight Hours After.6hadeel fahimNo ratings yet
- Motta 2004Document4 pagesMotta 2004muntasir antuNo ratings yet
- Post-Arrest Therapeutic Hypothermia in Pediatric Patients With Congenital Heart Disease - 2018Document19 pagesPost-Arrest Therapeutic Hypothermia in Pediatric Patients With Congenital Heart Disease - 2018Chang TruNo ratings yet
- Bradley 2018 Oi 180199Document11 pagesBradley 2018 Oi 180199Steven BrownNo ratings yet
- Post Cardiac Arrest Therapeutic Hypothermia in Adult Patients, State of Art and Practical ConsiderationsDocument11 pagesPost Cardiac Arrest Therapeutic Hypothermia in Adult Patients, State of Art and Practical Considerationsserena7205No ratings yet
- Brain Injury Resuscitation 2009Document8 pagesBrain Injury Resuscitation 2009Dandy Azmi AzwirNo ratings yet
- Intermittent Hemodialysis For Managing Metabolic Acidosis During Resuscitation of Septic Shock: A Descriptive StudyDocument5 pagesIntermittent Hemodialysis For Managing Metabolic Acidosis During Resuscitation of Septic Shock: A Descriptive Studyilham masdarNo ratings yet
- Crane Otomi ADocument11 pagesCrane Otomi ATemoc TemocNo ratings yet
- Nejmoa 2100591Document12 pagesNejmoa 2100591FELIPE OTALVARO ALVAREZNo ratings yet
- ECZ TTM TrainingDocument31 pagesECZ TTM Trainingeczhr.eczuricNo ratings yet
- Fever Management in Acute Brain Injury: ReviewDocument8 pagesFever Management in Acute Brain Injury: ReviewYuyuNo ratings yet
- Incidence of Postoperative Shivering Decreased With The Use of Acetaminophen: A Propensity Score Matching AnalysisDocument7 pagesIncidence of Postoperative Shivering Decreased With The Use of Acetaminophen: A Propensity Score Matching AnalysisnukeNo ratings yet
- ResuscitationDocument4 pagesResuscitationZara Yupita AzraNo ratings yet
- Icu Journal ClubDocument4 pagesIcu Journal Clubapi-610938913No ratings yet
- Comparison DN Vs Custodiol in ChildrenDocument12 pagesComparison DN Vs Custodiol in ChildrenAldo Miguel Flores GómezNo ratings yet
- Efficacy of Active Forced Air Warming During.92Document8 pagesEfficacy of Active Forced Air Warming During.92kepheroNo ratings yet
- Guidelines For The Management of Severe Traumatic Brain InjuryDocument50 pagesGuidelines For The Management of Severe Traumatic Brain InjurydenekeNo ratings yet
- Insight Into The Use of Tympanic Temperature During Target Temperature Management in Emergency and Critical Care: A Scoping ReviewDocument18 pagesInsight Into The Use of Tympanic Temperature During Target Temperature Management in Emergency and Critical Care: A Scoping Reviewmarcelo.lacknerNo ratings yet
- Temperature Management For Comatose Adult Survivors of Cardiac Arrest A Science Advisory From The American Heart AssociationDocument7 pagesTemperature Management For Comatose Adult Survivors of Cardiac Arrest A Science Advisory From The American Heart AssociationfbonillaNo ratings yet
- Temperature Control After Adult Cardiac Arrest AnDocument9 pagesTemperature Control After Adult Cardiac Arrest Anaida154No ratings yet
- Bertsch 2010Document14 pagesBertsch 2010Daniel ChaNo ratings yet
- Is There Still A Role For Hypothermia in Neurocritical Care?Document7 pagesIs There Still A Role For Hypothermia in Neurocritical Care?Oswaldo García-ParraNo ratings yet
- JURNAL READING - Asam TranexamatDocument45 pagesJURNAL READING - Asam TranexamatNurul fajriyatiNo ratings yet
- Just The Facts: Massive Hemorrhage Protocol: Clinical ScenarioDocument3 pagesJust The Facts: Massive Hemorrhage Protocol: Clinical ScenarioIsraelNo ratings yet
- The Setscore To Predict Tracheostomy Need in Cerebrovascular Neurocritical Care PatientsDocument11 pagesThe Setscore To Predict Tracheostomy Need in Cerebrovascular Neurocritical Care PatientsLuis HernándezNo ratings yet
- 2019 Guidelines Update Infographic PALS FINAL EN PDFDocument1 page2019 Guidelines Update Infographic PALS FINAL EN PDFVinay Kumar NandimallaNo ratings yet
- Deccompresive Brain InjuryDocument4 pagesDeccompresive Brain InjuryDharmendra WidetyaNo ratings yet
- Walter Reed MCHypothermiaprotocolrevised 21 SeptDocument8 pagesWalter Reed MCHypothermiaprotocolrevised 21 SeptBEST OF PAKISTANNo ratings yet
- Manuseio Da Hipotermia No Tactical Combat Casualty CareDocument26 pagesManuseio Da Hipotermia No Tactical Combat Casualty CareVitorNo ratings yet
- ICU Trial SummariesDocument31 pagesICU Trial SummariesSimon WongNo ratings yet
- Aha 24 HorasDocument17 pagesAha 24 HorasRichard SossaNo ratings yet
- FUGANTI, CCT Efeitos Do PreaquecimentoDocument10 pagesFUGANTI, CCT Efeitos Do PreaquecimentoIngrid AraújoNo ratings yet
- 4 Preliminary Guideline - and Pathophysiology - Base Protocols For Neurological CareDocument9 pages4 Preliminary Guideline - and Pathophysiology - Base Protocols For Neurological CareehuaniNo ratings yet
- Part 15 PDFDocument7 pagesPart 15 PDFKarolina PolskaNo ratings yet
- Intracranial Pressure Management in Patients With Traumatic Brain Injury: An UpdateDocument5 pagesIntracranial Pressure Management in Patients With Traumatic Brain Injury: An UpdatedimasNo ratings yet
- Artigo 2 PubmedDocument10 pagesArtigo 2 PubmedThiago GonçalvesNo ratings yet
- Raval 2008 J Clin Monit ComputDocument7 pagesRaval 2008 J Clin Monit ComputCamilaNo ratings yet
- Early Intravenous Thrombolysis For Acute Ischemic Stroke in A Community-Based ApproachDocument7 pagesEarly Intravenous Thrombolysis For Acute Ischemic Stroke in A Community-Based ApproachBeny RiliantoNo ratings yet
- Abstract TTMDocument16 pagesAbstract TTMssasongkoNo ratings yet
- Blood Pressure Management in Intracerebral Haemorrhage When, HowDocument9 pagesBlood Pressure Management in Intracerebral Haemorrhage When, HowpepeNo ratings yet
- Columbia Anti Shivering ProtocolDocument6 pagesColumbia Anti Shivering ProtocolPisica ZmeuNo ratings yet
- Strokeaha 119 027356Document4 pagesStrokeaha 119 027356Orlin ZlatarskiNo ratings yet
- Management of Acute Moderate and Severe Traumatic Brain InjuryDocument34 pagesManagement of Acute Moderate and Severe Traumatic Brain InjuryAndra MariaNo ratings yet
- 01 STR 0000137607 61697 77Document6 pages01 STR 0000137607 61697 77Jasna BuhariNo ratings yet
- Massive Hemorrhage ProtocolDocument19 pagesMassive Hemorrhage ProtocolYeseniaNo ratings yet
- JurnalDocument7 pagesJurnalbrygitaymNo ratings yet
- AnnCardAnaesth9144-7552051 020552Document5 pagesAnnCardAnaesth9144-7552051 020552Imanuel Far-FarNo ratings yet
- Risck Factor For Prostoperative Hypothermia in TheDocument9 pagesRisck Factor For Prostoperative Hypothermia in TheRaul SousaNo ratings yet
- Takutsubo SyndromeDocument17 pagesTakutsubo Syndromerizqina ajraNo ratings yet
- Bab Iii Pembahasan: 3.1. Profil Penelitian 3.1.1. Judul PenelitianDocument4 pagesBab Iii Pembahasan: 3.1. Profil Penelitian 3.1.1. Judul PenelitianMuhammad Mariadi FirdausNo ratings yet
- DCV PDFDocument25 pagesDCV PDFLeyDi CamposanoNo ratings yet
- Concept Map PedsDocument7 pagesConcept Map Pedsapi-545001894No ratings yet
- Combine Class Chronic Inflammation & Wound Healing (Power Point)Document35 pagesCombine Class Chronic Inflammation & Wound Healing (Power Point)Suleiman KikulweNo ratings yet
- Microbiological Quality of Bottled Drinking W A T E R in The Uae and The Effect of Storage at Different TemperaturesDocument5 pagesMicrobiological Quality of Bottled Drinking W A T E R in The Uae and The Effect of Storage at Different TemperaturesUSMANNo ratings yet
- Fallot TetralogyDocument20 pagesFallot Tetralogykgt88No ratings yet
- MEN1 PPDocument15 pagesMEN1 PPAaron D. PhoenixNo ratings yet
- Acupuncture Brochure 002Document2 pagesAcupuncture Brochure 002Stanley NguiNo ratings yet
- Skala Klepto PDFDocument2 pagesSkala Klepto PDFdefani ismiriamNo ratings yet
- Duke University Department of Medicine Annual Report 2013Document21 pagesDuke University Department of Medicine Annual Report 2013Duke Department of MedicineNo ratings yet
- Who Pen 2020Document85 pagesWho Pen 2020Faye PalmaresNo ratings yet
- FIIIIIINAAAAALLLLLLDocument132 pagesFIIIIIINAAAAALLLLLLJohn Remy HerbitoNo ratings yet
- Pylori) Is Most Common Bacterial Cause of Gastritis.: IndigestionDocument6 pagesPylori) Is Most Common Bacterial Cause of Gastritis.: IndigestionLANGWAEMILLNo ratings yet
- Seminar IDAI Protein Intake To Support Immune System Children With Allergy Disease PDFDocument39 pagesSeminar IDAI Protein Intake To Support Immune System Children With Allergy Disease PDFMohammad Jofa Rachman PNo ratings yet
- Heart AnatomyDocument11 pagesHeart AnatomyJohn FisherNo ratings yet
- Cuidado PacientDocument92 pagesCuidado PacientdanielaNo ratings yet
- The Commonwealth of Massachusetts: One Ashburton Place, Room 1819 Boston, Massachusetts 02108Document53 pagesThe Commonwealth of Massachusetts: One Ashburton Place, Room 1819 Boston, Massachusetts 02108WBURNo ratings yet
- FR Muller-HMC-PGSynopsis (2007-08)Document30 pagesFR Muller-HMC-PGSynopsis (2007-08)mapati66No ratings yet
- Principles of Drug Therapy For The Elderly PatientDocument16 pagesPrinciples of Drug Therapy For The Elderly PatientGalih Maygananda Putra100% (1)
- Knockout Paralysis FlyerDocument1 pageKnockout Paralysis FlyerJessika KattahNo ratings yet
- Product BookletDocument46 pagesProduct BookletNARESH JANDIALNo ratings yet
- Hospital ProgrammingDocument24 pagesHospital ProgrammingJolina InverseNo ratings yet
- LP 4-ImmunoprophylaxisDocument15 pagesLP 4-ImmunoprophylaxismlinaballerinaNo ratings yet
- Ilovepdf MergedDocument125 pagesIlovepdf MergedinnyNo ratings yet
- Week 3 - MenstruationDocument10 pagesWeek 3 - MenstruationTEDDY BEAR PRODUCTIONNo ratings yet
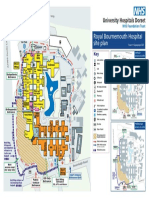
- Royal Bournemouth Hospital Site Plan: A338 Wessex Wa yDocument1 pageRoyal Bournemouth Hospital Site Plan: A338 Wessex Wa ydolar buhaNo ratings yet
- Vaginal Examination Wit RationaleDocument1 pageVaginal Examination Wit RationaleAna Maria Teresa H RollanNo ratings yet
- Why Should A Hospital Have CSSDDocument12 pagesWhy Should A Hospital Have CSSDANOOPVA100% (1)
- SafeguardDocument2 pagesSafeguardApril Joy EbinNo ratings yet