Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5825)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Woodenclock Gears-Pl PDFDocument8 pagesWoodenclock Gears-Pl PDFstaticfactory928178% (9)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Oxford Handbooks Download LinkDocument5 pagesOxford Handbooks Download LinkAdithya Vishwanath43% (7)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Miessler-Fischer-Tarr5e SM CH 07 CM FinalDocument10 pagesMiessler-Fischer-Tarr5e SM CH 07 CM FinalgrignardreagnetsNo ratings yet
- Acquired C1 Inhibitor Deficiencymanagement and PrognosisDocument14 pagesAcquired C1 Inhibitor Deficiencymanagement and PrognosisjalalfaizNo ratings yet
- ACE Inhibitor-Induced AngioedemaDocument14 pagesACE Inhibitor-Induced AngioedemajalalfaizNo ratings yet
- Lichen Planus and Its Management An Update and Observation Ijced 18 001Document5 pagesLichen Planus and Its Management An Update and Observation Ijced 18 001jalalfaizNo ratings yet
- Cutaneous TuberculosisDocument10 pagesCutaneous TuberculosisjalalfaizNo ratings yet
- Pityriasis RoseaDocument2 pagesPityriasis RoseajalalfaizNo ratings yet
- Lichen Planus: Santa Clara Medical Center, Department of Dermatology #472Document2 pagesLichen Planus: Santa Clara Medical Center, Department of Dermatology #472jalalfaizNo ratings yet
- Acne Keloidalis NuchaeDocument16 pagesAcne Keloidalis NuchaejalalfaizNo ratings yet
- Levamisole in L.PDocument5 pagesLevamisole in L.PjalalfaizNo ratings yet
- Pemphigus: Clinical FeaturesDocument7 pagesPemphigus: Clinical FeaturesjalalfaizNo ratings yet
- WartsDocument5 pagesWartsjalalfaizNo ratings yet
- PemphigoidDocument4 pagesPemphigoidjalalfaizNo ratings yet
- Candidiasis: Clinical FeaturesDocument4 pagesCandidiasis: Clinical FeaturesjalalfaizNo ratings yet
- UrticariaDocument5 pagesUrticariajalalfaizNo ratings yet
- Molluscum ContagiosumDocument2 pagesMolluscum ContagiosumjalalfaizNo ratings yet
- Herpes SimplexDocument5 pagesHerpes SimplexjalalfaizNo ratings yet
- 21 Molluscum Contagiosum PDFDocument2 pages21 Molluscum Contagiosum PDFjalalfaizNo ratings yet
- Tinea (Dermatomycosis)Document9 pagesTinea (Dermatomycosis)jalalfaizNo ratings yet
- Tinea VersicolorDocument2 pagesTinea VersicolorjalalfaizNo ratings yet
- Deep Mycotic InfectionDocument5 pagesDeep Mycotic InfectionjalalfaizNo ratings yet
- Lichen Simplex ChronicusDocument3 pagesLichen Simplex ChronicusjalalfaizNo ratings yet
- Lupus Vulgaris of External NoseDocument3 pagesLupus Vulgaris of External NosejalalfaizNo ratings yet
- PyodermasDocument5 pagesPyodermasjalalfaizNo ratings yet
- Drug ReactionsDocument11 pagesDrug ReactionsjalalfaizNo ratings yet
- Acne and Acneiform DermatosesDocument5 pagesAcne and Acneiform DermatosesjalalfaizNo ratings yet
- Meralgia Paresthetica: Case PresentationDocument2 pagesMeralgia Paresthetica: Case PresentationjalalfaizNo ratings yet
- I S D, TC, I S: Mechanisms of DiseaseDocument12 pagesI S D, TC, I S: Mechanisms of DiseasejalalfaizNo ratings yet
- Top 30 Skin DiseasesDocument32 pagesTop 30 Skin DiseasesjalalfaizNo ratings yet
- 2016 Glencolmcille Show Entry BookletDocument24 pages2016 Glencolmcille Show Entry BookletGlencolmcille ShowNo ratings yet
- Session 14 Anxiety - Related DisordersDocument1 pageSession 14 Anxiety - Related DisordersMichelle Dona MirallesNo ratings yet
- Covid 19 Per Diem Offer Letter TemplateDocument7 pagesCovid 19 Per Diem Offer Letter TemplateAtchim NaiduNo ratings yet
- Vegetable Biryani Recipe by Sarita Bhandarkar - Ifood Sanjeev KapoorDocument3 pagesVegetable Biryani Recipe by Sarita Bhandarkar - Ifood Sanjeev KapoorNimmi NimsNo ratings yet
- Eng Turbomixer Brochure 2022Document28 pagesEng Turbomixer Brochure 2022BENHAIBA WAFAENo ratings yet
- MT36, MT41 Parts BookDocument669 pagesMT36, MT41 Parts Booksergio mata100% (2)
- Modicon TM3 - TM3DI16Document8 pagesModicon TM3 - TM3DI16Abdan SyakuraNo ratings yet
- Software Requirements Specification: Version 1.0 ApprovedDocument8 pagesSoftware Requirements Specification: Version 1.0 Approvedkirtika patelNo ratings yet
- PhilHealth CF4Document2 pagesPhilHealth CF4B MNo ratings yet
- Exercise ReadingDocument3 pagesExercise ReadingMuhammadMa'rufYusnainNo ratings yet
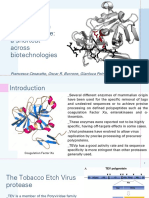
- Tobacco Etch Virus Protease: A Shortcut Across BiotechnologiesDocument16 pagesTobacco Etch Virus Protease: A Shortcut Across BiotechnologiesNhật ThiệnNo ratings yet
- UntitledDocument873 pagesUntitledjoker hotNo ratings yet
- RTN 320 V100 Quick Installation Guide 02Document37 pagesRTN 320 V100 Quick Installation Guide 02Juan Pablo CharrisNo ratings yet
- KNH 413 Case Study 4Document12 pagesKNH 413 Case Study 4api-272540385100% (1)
- 046: Unsafe Acts vs. Unsafe Conditions: Background Discussion Leader Duties For This SessionDocument2 pages046: Unsafe Acts vs. Unsafe Conditions: Background Discussion Leader Duties For This SessionVarahi VigneshNo ratings yet
- PPE PosterDocument1 pagePPE PosterJalak PatelNo ratings yet
- Sugafax BulletinDocument4 pagesSugafax BulletinmndmattNo ratings yet
- Levels of OrganizationDocument19 pagesLevels of OrganizationJoie MonrealNo ratings yet
- Harmony XB4 - XB4BD53Document5 pagesHarmony XB4 - XB4BD53vNo ratings yet
- Exploring The Mysteries of The Deep SeaDocument2 pagesExploring The Mysteries of The Deep SeaJajon JaesNo ratings yet
- Clniical ReasoningDocument30 pagesClniical Reasoningnunu ahmedNo ratings yet
- PHIL286 Handout 8Document3 pagesPHIL286 Handout 8Mochammad AndreNo ratings yet
- 10P 2L8M D5 V3 Product SpecificationsDocument6 pages10P 2L8M D5 V3 Product SpecificationsAnkur PrasadNo ratings yet
- Johnson OE (2012) - Therapeutic Exercises in The Management of Non-Specific Low Back PainDocument23 pagesJohnson OE (2012) - Therapeutic Exercises in The Management of Non-Specific Low Back PainApollwn100% (1)
- Awwa C 200 Specifications: " Steel Water Pipe - 6 Diameter and More "Document1 pageAwwa C 200 Specifications: " Steel Water Pipe - 6 Diameter and More "joseNo ratings yet
- Activity Guides 3 - 9°Document3 pagesActivity Guides 3 - 9°Dayanna Sofia Jossa OchoaNo ratings yet
- NC State PDFDocument27 pagesNC State PDFquantum16No ratings yet
- BookDocument424 pagesBookFolinNo ratings yet