
Clinico Morphological Evaluation of Melasma and Other Hyperpigmentary Disorders of Skin
Clinico Morphological Evaluation of Melasma and Other Hyperpigmentary Disorders of Skin
You might also like
- Lookingbill and Marksâ Principles of Dermatology (PDFDrive)Document320 pagesLookingbill and Marksâ Principles of Dermatology (PDFDrive)Alexander Hartono100% (5)
- Your Body Believes Every Word Y - Barbara Hoberman LevineDocument380 pagesYour Body Believes Every Word Y - Barbara Hoberman LevineRoryBradshawNo ratings yet
- SKIN TYPES Roberts2009Document5 pagesSKIN TYPES Roberts2009Brigitte Elisa Vivanco CcahuanaNo ratings yet
- Case 4 - Diana Cross - Sheet1Document1 pageCase 4 - Diana Cross - Sheet1muranNo ratings yet
- Micro Chapter 6 Ppt.11th EditionDocument66 pagesMicro Chapter 6 Ppt.11th EditionPVallNo ratings yet
- HPP BrochureDocument2 pagesHPP BrochureAlbert YoungNo ratings yet
- Melasma A Prospective Study of Clinico Etiological and Dermoscopic Pattern in MenDocument4 pagesMelasma A Prospective Study of Clinico Etiological and Dermoscopic Pattern in MenInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Thyroid Disorders in Patients With MelasmaDocument8 pagesThyroid Disorders in Patients With MelasmaIJAR JOURNALNo ratings yet
- Nauti Yal 2021Document29 pagesNauti Yal 2021Amanda LopesNo ratings yet
- Neagu 2021Document40 pagesNeagu 2021meenakshi.r.agrawalNo ratings yet
- Evaluation of Quality of Life in Female Patients With MelasmaDocument5 pagesEvaluation of Quality of Life in Female Patients With Melasmaضحى الغزيNo ratings yet
- Dissertation LeucodermaDocument90 pagesDissertation LeucodermaRashmi Mishra100% (1)
- Melasma UpdateDocument11 pagesMelasma Updateirwan jun100% (1)
- A Case Report of A Morphea in A 19 Years Old FemaleDocument2 pagesA Case Report of A Morphea in A 19 Years Old FemaleInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Association Between Melasma and Postin Ammatory Hyperpigmenta-Tion in Acne PatientsDocument4 pagesThe Association Between Melasma and Postin Ammatory Hyperpigmenta-Tion in Acne PatientsRicoNo ratings yet
- 2021 The Pathogenesis of Melasma and Implications For TreatmentDocument14 pages2021 The Pathogenesis of Melasma and Implications For Treatmentyezafig4001No ratings yet
- Papu Los Qu AmousDocument8 pagesPapu Los Qu AmousKata TölgyesiNo ratings yet
- Dermoscopic Features of Pigmentary Disorders in Indian Skin: A Prospective Observational StudyDocument10 pagesDermoscopic Features of Pigmentary Disorders in Indian Skin: A Prospective Observational StudyIJAR JOURNALNo ratings yet
- PRELIMS - Indd 17 1/18/2018 11:06:42 AMDocument7 pagesPRELIMS - Indd 17 1/18/2018 11:06:42 AMhoang ho LeNo ratings yet
- Natural Options For Management of MelasmaDocument17 pagesNatural Options For Management of Melasmapuji lestari100% (1)
- Tratment Melasma PDFDocument18 pagesTratment Melasma PDFGheavita Chandra DewiNo ratings yet
- Article WJPR 1469860909Document27 pagesArticle WJPR 1469860909loNo ratings yet
- brown2011Document4 pagesbrown2011z8hc2s6scpNo ratings yet
- MelasmaDocument6 pagesMelasmaMuhammad Irfan BalochNo ratings yet
- melasma abstract finalDocument15 pagesmelasma abstract finalshaikzaiba46No ratings yet
- New Oral and Topical Approaches For The Treatment of MelasmaDocument7 pagesNew Oral and Topical Approaches For The Treatment of MelasmaSong JieunNo ratings yet
- International Journal of Women's Dermatology: P.E. Grimes, MD, S. Ijaz, BA, MPH, R. Nashawati, BS, MSGM, D. KwakDocument7 pagesInternational Journal of Women's Dermatology: P.E. Grimes, MD, S. Ijaz, BA, MPH, R. Nashawati, BS, MSGM, D. KwakRiefka Ananda ZulfaNo ratings yet
- PCMR 12404Document14 pagesPCMR 12404Riefka Ananda ZulfaNo ratings yet
- Shankar2014 Evidence Based Treatment MelasmaDocument22 pagesShankar2014 Evidence Based Treatment MelasmaErnawati HidayatNo ratings yet
- Hyperpigmentation and Melasma: D Rigopoulos, MD, PHD, S Gregoriou, MD, & A Katsambas, MD, PHDDocument8 pagesHyperpigmentation and Melasma: D Rigopoulos, MD, PHD, S Gregoriou, MD, & A Katsambas, MD, PHDGÜLSÜM GÜNEŞNo ratings yet
- Guideline MelasmaDocument23 pagesGuideline MelasmaTHERESIANo ratings yet
- A Comparative Study of Efficacy Between Modified Kligmans Formula and Dermaroller With Tranexamic Acid in Treatment of MelasmaDocument8 pagesA Comparative Study of Efficacy Between Modified Kligmans Formula and Dermaroller With Tranexamic Acid in Treatment of MelasmaIJAR JOURNALNo ratings yet
- Evaluation Ofefficacy of Cysteamine Cream in The Treatment of Epidermal Melasma - A Randomized Double Blind Placebo Controlled StudyDocument28 pagesEvaluation Ofefficacy of Cysteamine Cream in The Treatment of Epidermal Melasma - A Randomized Double Blind Placebo Controlled StudyFransiscus ClintonNo ratings yet
- Diseases of Skin With HP ManagementDocument130 pagesDiseases of Skin With HP ManagementMaheen HayatNo ratings yet
- Melasma Insights and PerspectivesDocument6 pagesMelasma Insights and PerspectivesTatianaNo ratings yet
- Topic Treatment Acne Scars1Document3 pagesTopic Treatment Acne Scars1Stanca NicolaeNo ratings yet
- DamevskamelasmasjdvDocument15 pagesDamevskamelasmasjdvlaithuyduong007No ratings yet
- Dic 2021 11 2Document14 pagesDic 2021 11 2Kopo Sentral MedikaNo ratings yet
- Sarkar, RashmiDocument10 pagesSarkar, RashmiXena Poetri Xaverya RenggaNo ratings yet
- A Novel at Home Procedure Providing Marked Improvements - 2014 - Journal of The PDFDocument1 pageA Novel at Home Procedure Providing Marked Improvements - 2014 - Journal of The PDFNachi MontianarrtNo ratings yet
- Melasma and HomoeopathyDocument14 pagesMelasma and HomoeopathyDr. Rajneesh Kumar Sharma MD HomNo ratings yet
- Laser Skin Treatment in Non-Caucasian PatientsReview ArticleDocument8 pagesLaser Skin Treatment in Non-Caucasian PatientsReview ArticledoctorbanNo ratings yet
- Ashy Dermatosis and Lichen PlanusDocument27 pagesAshy Dermatosis and Lichen PlanusAthenaeum Scientific PublishersNo ratings yet
- 63a739687e3dd0 44662008Document12 pages63a739687e3dd0 44662008Sravani PeddagangannagariNo ratings yet
- Glacial RXDocument15 pagesGlacial RXcarloshgmedeirosNo ratings yet
- Skin Manifestations of Hypothyroidism-A Clinical Study: S.Haritha, K. Kirthi SampathDocument3 pagesSkin Manifestations of Hypothyroidism-A Clinical Study: S.Haritha, K. Kirthi SampathGorakh Raj JoshiNo ratings yet
- Melasma: An Up-to-Date Comprehensive Review: Oluwatobi A. Ogbechie-Godec Nada ElbulukDocument14 pagesMelasma: An Up-to-Date Comprehensive Review: Oluwatobi A. Ogbechie-Godec Nada ElbulukDra Natalia Maria ZuluagaNo ratings yet
- Httpmediskin - Cnuploadfilesfile2013073120130731095126 3872 PDFDocument9 pagesHttpmediskin - Cnuploadfilesfile2013073120130731095126 3872 PDFRHBeautyCareTambolakaNo ratings yet
- 241932-Article Text-834071-2-10-20200806Document9 pages241932-Article Text-834071-2-10-20200806mushaddiqNo ratings yet
- A Comparative Study of Dermatoscopic Features of Acne-Related Postinfl Ammatory Hyperpigmentation in Facial and Nonfacial Areas in Asian PatientsDocument6 pagesA Comparative Study of Dermatoscopic Features of Acne-Related Postinfl Ammatory Hyperpigmentation in Facial and Nonfacial Areas in Asian Patientsdesi kumarayantiNo ratings yet
- Cosmetics 10 00025 v2 - RemovedDocument2 pagesCosmetics 10 00025 v2 - Removedmeisya 102018090No ratings yet
- 9930 PDFDocument9 pages9930 PDFAnonymous 2BC7omLaWCNo ratings yet
- Skin Disorders in Patients With Primary Psychiatric ConditionsDocument3 pagesSkin Disorders in Patients With Primary Psychiatric ConditionsWahyuniNo ratings yet
- Recent Advancements in Skin Cancer Treatment: A Critical ReviewDocument31 pagesRecent Advancements in Skin Cancer Treatment: A Critical ReviewRajat GoyalNo ratings yet
- Assessment of Laser Effects On Skin RejuvenationDocument8 pagesAssessment of Laser Effects On Skin RejuvenationOrel LachianiNo ratings yet
- Top Six Health Issue in SingaporeDocument22 pagesTop Six Health Issue in SingaporeMatthewRumondorNo ratings yet
- Overview of Ultrasound Imaging Applications in DermatologyDocument9 pagesOverview of Ultrasound Imaging Applications in DermatologyLeonardo PiberNo ratings yet
- Dermatologica Sinica: Ai-Young LeeDocument7 pagesDermatologica Sinica: Ai-Young LeeNatta ApucaranaNo ratings yet
- Thesis PsoriasisDocument4 pagesThesis PsoriasisDereck Downing100% (2)
- Efektivitas Dan Keamanan Kojic DipalmitatDocument6 pagesEfektivitas Dan Keamanan Kojic DipalmitatmurjonocrbNo ratings yet
- Iranian Journal of Basic Medical SciencesDocument10 pagesIranian Journal of Basic Medical SciencesDeaz Fazzaura PutriNo ratings yet
- Evaluation of Culture Media For The Rapid Isolation of DermatophytesDocument4 pagesEvaluation of Culture Media For The Rapid Isolation of DermatophytesIOSRjournalNo ratings yet
- Melanoma Classification A Comprehensive Survey (3 240314 220858Document67 pagesMelanoma Classification A Comprehensive Survey (3 240314 220858Kovid AggarwalNo ratings yet
- Patch Testing and Prick Testing: A Practical Guide Official Publication of the ICDRGFrom EverandPatch Testing and Prick Testing: A Practical Guide Official Publication of the ICDRGNo ratings yet
- Development and Validation of Stability Indicating Assay Method For Estimation of Teriflunomide in Tablet Dosage FormDocument11 pagesDevelopment and Validation of Stability Indicating Assay Method For Estimation of Teriflunomide in Tablet Dosage FormBaru Chandrasekhar RaoNo ratings yet
- Analytical Method Development and Validation of Stability Indicating RP-HPLC Method For Estimation of Lercanidipine Hydrochloride and Enalapril Maleate in CombinationDocument8 pagesAnalytical Method Development and Validation of Stability Indicating RP-HPLC Method For Estimation of Lercanidipine Hydrochloride and Enalapril Maleate in CombinationBaru Chandrasekhar RaoNo ratings yet
- Relationship of Testosterone With Body Mass Index in Infertile Males in Local CommunityDocument4 pagesRelationship of Testosterone With Body Mass Index in Infertile Males in Local CommunityBaru Chandrasekhar RaoNo ratings yet
- Gastroprotective Activity of Methanolic Extract of Phyllanthus Acidus Fruit Against Indomethacin-Induced Gastric Ulcers in RatsDocument7 pagesGastroprotective Activity of Methanolic Extract of Phyllanthus Acidus Fruit Against Indomethacin-Induced Gastric Ulcers in RatsBaru Chandrasekhar RaoNo ratings yet
- Knowledge On Antibiotics Use and Its Storage Among Saudi Arabia Residents: A Cross Sectional StudyDocument8 pagesKnowledge On Antibiotics Use and Its Storage Among Saudi Arabia Residents: A Cross Sectional StudyBaru Chandrasekhar RaoNo ratings yet
- A Brief Review On YawsDocument7 pagesA Brief Review On YawsBaru Chandrasekhar RaoNo ratings yet
- Review On: Inventory ManagementDocument8 pagesReview On: Inventory ManagementBaru Chandrasekhar RaoNo ratings yet
- Pharmaceutical Sciences: IAJPS 2018, 05 (04), 3075-3081 Aneeqa Ali RaoDocument7 pagesPharmaceutical Sciences: IAJPS 2018, 05 (04), 3075-3081 Aneeqa Ali RaoBaru Chandrasekhar RaoNo ratings yet
- Assessment of Correlation Between Physical Activity and Academic Performance Among The Students of Gujranwala Medical College, GujranwalaDocument7 pagesAssessment of Correlation Between Physical Activity and Academic Performance Among The Students of Gujranwala Medical College, GujranwalaBaru Chandrasekhar RaoNo ratings yet
- Descriptive Study Knowing The Patients Load in The Neonatal Icu at The Tertiary Care Hospital LahoreDocument4 pagesDescriptive Study Knowing The Patients Load in The Neonatal Icu at The Tertiary Care Hospital LahoreBaru Chandrasekhar RaoNo ratings yet
- The Role of Clinical Pharmacist in Pharmacovigilance and Drug Safety in Teritiary Care Teaching HospitalDocument11 pagesThe Role of Clinical Pharmacist in Pharmacovigilance and Drug Safety in Teritiary Care Teaching HospitalBaru Chandrasekhar RaoNo ratings yet
- Pharmacological and Phytochemical Evidence of Scutia Genus Plants - A ReviewDocument7 pagesPharmacological and Phytochemical Evidence of Scutia Genus Plants - A ReviewBaru Chandrasekhar RaoNo ratings yet
- DISTINCTIVE PHARMACOLOGICAL ACTIVITIES OF Eclipta Alba AND IT'S COUMESTAN WEDELOLACTONEDocument7 pagesDISTINCTIVE PHARMACOLOGICAL ACTIVITIES OF Eclipta Alba AND IT'S COUMESTAN WEDELOLACTONEBaru Chandrasekhar RaoNo ratings yet
- DETERMINATION OF BIOACTIVE COMPOUNDS FROM Piper Nigrum. L BY USING HPLC ANALYSISDocument3 pagesDETERMINATION OF BIOACTIVE COMPOUNDS FROM Piper Nigrum. L BY USING HPLC ANALYSISBaru Chandrasekhar RaoNo ratings yet
- Determination of Bioactive Compounds From Piper Nigrum L by Using Ft-Ir Spectroscopic AnalysisDocument3 pagesDetermination of Bioactive Compounds From Piper Nigrum L by Using Ft-Ir Spectroscopic AnalysisBaru Chandrasekhar RaoNo ratings yet
- RP-HPLC Method Development and Validation of Alogliptin Bulk and Tablet Dosage FormDocument8 pagesRP-HPLC Method Development and Validation of Alogliptin Bulk and Tablet Dosage FormBaru Chandrasekhar RaoNo ratings yet
- STUDIES ON QUALITATIVE PHYTOCHEMICAL ANALYSIS AND ANTIBACTERIAL ACTIVITY OF Piper NigrumDocument7 pagesSTUDIES ON QUALITATIVE PHYTOCHEMICAL ANALYSIS AND ANTIBACTERIAL ACTIVITY OF Piper NigrumBaru Chandrasekhar RaoNo ratings yet
- Determination of Bioactive Compounds From Piper Longum L. by Using HP-LC AnalysisDocument4 pagesDetermination of Bioactive Compounds From Piper Longum L. by Using HP-LC AnalysisBaru Chandrasekhar RaoNo ratings yet
- Blood Products and Their UsesDocument28 pagesBlood Products and Their UsesJeevitha Vanitha100% (1)
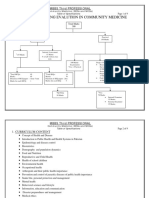
- Flow Chart Showng Evalution in Community Medicine: Mbbs Third ProfessionalDocument9 pagesFlow Chart Showng Evalution in Community Medicine: Mbbs Third ProfessionalusamaNo ratings yet
- Admission Notice For General PublicDocument6 pagesAdmission Notice For General Publicmoney moneyNo ratings yet
- Respiratory System: Copd (Bronchitis & Emphysema)Document7 pagesRespiratory System: Copd (Bronchitis & Emphysema)Rhea Lyn LamosteNo ratings yet
- Immature GranulocytesDocument10 pagesImmature Granulocytespieterinpretoria391No ratings yet
- Screenshot 2023-12-11 at 3.53.36 PMDocument62 pagesScreenshot 2023-12-11 at 3.53.36 PMahmedmansi055No ratings yet
- Golden Hour of Neonatal Life - Need of The HourDocument21 pagesGolden Hour of Neonatal Life - Need of The HourEdwin AlvarezNo ratings yet
- CSR Activities of LUPIN LTDDocument12 pagesCSR Activities of LUPIN LTDVishal SinghNo ratings yet
- Comparison of Modified Borg Scale and Visual Analog Scale Dyspnea Scores in Predicting Re-Intervention After Drainage of Malignant Pleural EffusionDocument8 pagesComparison of Modified Borg Scale and Visual Analog Scale Dyspnea Scores in Predicting Re-Intervention After Drainage of Malignant Pleural EffusionMukhlis HasNo ratings yet
- PsychosisDocument11 pagesPsychosisChan's RoomNo ratings yet
- Augmentin DuoDocument2 pagesAugmentin Duojunaid hashmiNo ratings yet
- 26 ProtozoaDocument74 pages26 ProtozoaCalvin BlueNo ratings yet
- Air Pollution in QuitoDocument14 pagesAir Pollution in Quitoapi-385158934No ratings yet
- Chinese Exclusion Act 1f4nr0kDocument17 pagesChinese Exclusion Act 1f4nr0kbald bullNo ratings yet
- Complete Catalog Row0704Document175 pagesComplete Catalog Row0704Krish GulabaniNo ratings yet
- Slide Master Apm CPR N AedDocument46 pagesSlide Master Apm CPR N AedDivyaaNo ratings yet
- Puerperal SepsisDocument30 pagesPuerperal Sepsisjonaa2564No ratings yet
- Psychoanalysis of Gifted Minds PSYDocument12 pagesPsychoanalysis of Gifted Minds PSYVirat SinghNo ratings yet
- Field Visit Report To Vrindavan Botanical Garden and Lumle Regional Agricultural Research StationDocument43 pagesField Visit Report To Vrindavan Botanical Garden and Lumle Regional Agricultural Research StationAmresh kumar Shah100% (1)
- Cefepime Vs Zosyn For Empiric Sepsis CoverageDocument2 pagesCefepime Vs Zosyn For Empiric Sepsis Coveragetl drNo ratings yet
- Amyotrophic Lateral SclerosisDocument23 pagesAmyotrophic Lateral SclerosisAfshan Pt T100% (1)
- Malunggay Leaf Extracts As An AlternativDocument57 pagesMalunggay Leaf Extracts As An AlternativGrilhamon ShenNo ratings yet
- 1 s2.0 S0740002020301337 MainDocument9 pages1 s2.0 S0740002020301337 MainIggjchthfx JcytxutxutxtjNo ratings yet
- Rudiyanto, Liver FibrosisDocument41 pagesRudiyanto, Liver Fibrosisbudi darmantaNo ratings yet
- Three-Part EssayDocument1 pageThree-Part EssayLovely CastroNo ratings yet
- Annals of General Psychiatry: Hospital Anxiety and Depression Scale (HADS) : Validation in A Greek General Hospital SampleDocument5 pagesAnnals of General Psychiatry: Hospital Anxiety and Depression Scale (HADS) : Validation in A Greek General Hospital SampleGeraldo Antonio GranzottoNo ratings yet











































































































Download as pdf or txt
You might also like
- Lookingbill and Marksâ Principles of Dermatology (PDFDrive)Document320 pagesLookingbill and Marksâ Principles of Dermatology (PDFDrive)Alexander Hartono100% (5)
- Your Body Believes Every Word Y - Barbara Hoberman LevineDocument380 pagesYour Body Believes Every Word Y - Barbara Hoberman LevineRoryBradshawNo ratings yet
- SKIN TYPES Roberts2009Document5 pagesSKIN TYPES Roberts2009Brigitte Elisa Vivanco CcahuanaNo ratings yet
- Case 4 - Diana Cross - Sheet1Document1 pageCase 4 - Diana Cross - Sheet1muranNo ratings yet
- Micro Chapter 6 Ppt.11th EditionDocument66 pagesMicro Chapter 6 Ppt.11th EditionPVallNo ratings yet
- HPP BrochureDocument2 pagesHPP BrochureAlbert YoungNo ratings yet
- Melasma A Prospective Study of Clinico Etiological and Dermoscopic Pattern in MenDocument4 pagesMelasma A Prospective Study of Clinico Etiological and Dermoscopic Pattern in MenInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Thyroid Disorders in Patients With MelasmaDocument8 pagesThyroid Disorders in Patients With MelasmaIJAR JOURNALNo ratings yet
- Nauti Yal 2021Document29 pagesNauti Yal 2021Amanda LopesNo ratings yet
- Neagu 2021Document40 pagesNeagu 2021meenakshi.r.agrawalNo ratings yet
- Evaluation of Quality of Life in Female Patients With MelasmaDocument5 pagesEvaluation of Quality of Life in Female Patients With Melasmaضحى الغزيNo ratings yet
- Dissertation LeucodermaDocument90 pagesDissertation LeucodermaRashmi Mishra100% (1)
- Melasma UpdateDocument11 pagesMelasma Updateirwan jun100% (1)
- A Case Report of A Morphea in A 19 Years Old FemaleDocument2 pagesA Case Report of A Morphea in A 19 Years Old FemaleInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Association Between Melasma and Postin Ammatory Hyperpigmenta-Tion in Acne PatientsDocument4 pagesThe Association Between Melasma and Postin Ammatory Hyperpigmenta-Tion in Acne PatientsRicoNo ratings yet
- 2021 The Pathogenesis of Melasma and Implications For TreatmentDocument14 pages2021 The Pathogenesis of Melasma and Implications For Treatmentyezafig4001No ratings yet
- Papu Los Qu AmousDocument8 pagesPapu Los Qu AmousKata TölgyesiNo ratings yet
- Dermoscopic Features of Pigmentary Disorders in Indian Skin: A Prospective Observational StudyDocument10 pagesDermoscopic Features of Pigmentary Disorders in Indian Skin: A Prospective Observational StudyIJAR JOURNALNo ratings yet
- PRELIMS - Indd 17 1/18/2018 11:06:42 AMDocument7 pagesPRELIMS - Indd 17 1/18/2018 11:06:42 AMhoang ho LeNo ratings yet
- Natural Options For Management of MelasmaDocument17 pagesNatural Options For Management of Melasmapuji lestari100% (1)
- Tratment Melasma PDFDocument18 pagesTratment Melasma PDFGheavita Chandra DewiNo ratings yet
- Article WJPR 1469860909Document27 pagesArticle WJPR 1469860909loNo ratings yet
- brown2011Document4 pagesbrown2011z8hc2s6scpNo ratings yet
- MelasmaDocument6 pagesMelasmaMuhammad Irfan BalochNo ratings yet
- melasma abstract finalDocument15 pagesmelasma abstract finalshaikzaiba46No ratings yet
- New Oral and Topical Approaches For The Treatment of MelasmaDocument7 pagesNew Oral and Topical Approaches For The Treatment of MelasmaSong JieunNo ratings yet
- International Journal of Women's Dermatology: P.E. Grimes, MD, S. Ijaz, BA, MPH, R. Nashawati, BS, MSGM, D. KwakDocument7 pagesInternational Journal of Women's Dermatology: P.E. Grimes, MD, S. Ijaz, BA, MPH, R. Nashawati, BS, MSGM, D. KwakRiefka Ananda ZulfaNo ratings yet
- PCMR 12404Document14 pagesPCMR 12404Riefka Ananda ZulfaNo ratings yet
- Shankar2014 Evidence Based Treatment MelasmaDocument22 pagesShankar2014 Evidence Based Treatment MelasmaErnawati HidayatNo ratings yet
- Hyperpigmentation and Melasma: D Rigopoulos, MD, PHD, S Gregoriou, MD, & A Katsambas, MD, PHDDocument8 pagesHyperpigmentation and Melasma: D Rigopoulos, MD, PHD, S Gregoriou, MD, & A Katsambas, MD, PHDGÜLSÜM GÜNEŞNo ratings yet
- Guideline MelasmaDocument23 pagesGuideline MelasmaTHERESIANo ratings yet
- A Comparative Study of Efficacy Between Modified Kligmans Formula and Dermaroller With Tranexamic Acid in Treatment of MelasmaDocument8 pagesA Comparative Study of Efficacy Between Modified Kligmans Formula and Dermaroller With Tranexamic Acid in Treatment of MelasmaIJAR JOURNALNo ratings yet
- Evaluation Ofefficacy of Cysteamine Cream in The Treatment of Epidermal Melasma - A Randomized Double Blind Placebo Controlled StudyDocument28 pagesEvaluation Ofefficacy of Cysteamine Cream in The Treatment of Epidermal Melasma - A Randomized Double Blind Placebo Controlled StudyFransiscus ClintonNo ratings yet
- Diseases of Skin With HP ManagementDocument130 pagesDiseases of Skin With HP ManagementMaheen HayatNo ratings yet
- Melasma Insights and PerspectivesDocument6 pagesMelasma Insights and PerspectivesTatianaNo ratings yet
- Topic Treatment Acne Scars1Document3 pagesTopic Treatment Acne Scars1Stanca NicolaeNo ratings yet
- DamevskamelasmasjdvDocument15 pagesDamevskamelasmasjdvlaithuyduong007No ratings yet
- Dic 2021 11 2Document14 pagesDic 2021 11 2Kopo Sentral MedikaNo ratings yet
- Sarkar, RashmiDocument10 pagesSarkar, RashmiXena Poetri Xaverya RenggaNo ratings yet
- A Novel at Home Procedure Providing Marked Improvements - 2014 - Journal of The PDFDocument1 pageA Novel at Home Procedure Providing Marked Improvements - 2014 - Journal of The PDFNachi MontianarrtNo ratings yet
- Melasma and HomoeopathyDocument14 pagesMelasma and HomoeopathyDr. Rajneesh Kumar Sharma MD HomNo ratings yet
- Laser Skin Treatment in Non-Caucasian PatientsReview ArticleDocument8 pagesLaser Skin Treatment in Non-Caucasian PatientsReview ArticledoctorbanNo ratings yet
- Ashy Dermatosis and Lichen PlanusDocument27 pagesAshy Dermatosis and Lichen PlanusAthenaeum Scientific PublishersNo ratings yet
- 63a739687e3dd0 44662008Document12 pages63a739687e3dd0 44662008Sravani PeddagangannagariNo ratings yet
- Glacial RXDocument15 pagesGlacial RXcarloshgmedeirosNo ratings yet
- Skin Manifestations of Hypothyroidism-A Clinical Study: S.Haritha, K. Kirthi SampathDocument3 pagesSkin Manifestations of Hypothyroidism-A Clinical Study: S.Haritha, K. Kirthi SampathGorakh Raj JoshiNo ratings yet
- Melasma: An Up-to-Date Comprehensive Review: Oluwatobi A. Ogbechie-Godec Nada ElbulukDocument14 pagesMelasma: An Up-to-Date Comprehensive Review: Oluwatobi A. Ogbechie-Godec Nada ElbulukDra Natalia Maria ZuluagaNo ratings yet
- Httpmediskin - Cnuploadfilesfile2013073120130731095126 3872 PDFDocument9 pagesHttpmediskin - Cnuploadfilesfile2013073120130731095126 3872 PDFRHBeautyCareTambolakaNo ratings yet
- 241932-Article Text-834071-2-10-20200806Document9 pages241932-Article Text-834071-2-10-20200806mushaddiqNo ratings yet
- A Comparative Study of Dermatoscopic Features of Acne-Related Postinfl Ammatory Hyperpigmentation in Facial and Nonfacial Areas in Asian PatientsDocument6 pagesA Comparative Study of Dermatoscopic Features of Acne-Related Postinfl Ammatory Hyperpigmentation in Facial and Nonfacial Areas in Asian Patientsdesi kumarayantiNo ratings yet
- Cosmetics 10 00025 v2 - RemovedDocument2 pagesCosmetics 10 00025 v2 - Removedmeisya 102018090No ratings yet
- 9930 PDFDocument9 pages9930 PDFAnonymous 2BC7omLaWCNo ratings yet
- Skin Disorders in Patients With Primary Psychiatric ConditionsDocument3 pagesSkin Disorders in Patients With Primary Psychiatric ConditionsWahyuniNo ratings yet
- Recent Advancements in Skin Cancer Treatment: A Critical ReviewDocument31 pagesRecent Advancements in Skin Cancer Treatment: A Critical ReviewRajat GoyalNo ratings yet
- Assessment of Laser Effects On Skin RejuvenationDocument8 pagesAssessment of Laser Effects On Skin RejuvenationOrel LachianiNo ratings yet
- Top Six Health Issue in SingaporeDocument22 pagesTop Six Health Issue in SingaporeMatthewRumondorNo ratings yet
- Overview of Ultrasound Imaging Applications in DermatologyDocument9 pagesOverview of Ultrasound Imaging Applications in DermatologyLeonardo PiberNo ratings yet
- Dermatologica Sinica: Ai-Young LeeDocument7 pagesDermatologica Sinica: Ai-Young LeeNatta ApucaranaNo ratings yet
- Thesis PsoriasisDocument4 pagesThesis PsoriasisDereck Downing100% (2)
- Efektivitas Dan Keamanan Kojic DipalmitatDocument6 pagesEfektivitas Dan Keamanan Kojic DipalmitatmurjonocrbNo ratings yet
- Iranian Journal of Basic Medical SciencesDocument10 pagesIranian Journal of Basic Medical SciencesDeaz Fazzaura PutriNo ratings yet
- Evaluation of Culture Media For The Rapid Isolation of DermatophytesDocument4 pagesEvaluation of Culture Media For The Rapid Isolation of DermatophytesIOSRjournalNo ratings yet
- Melanoma Classification A Comprehensive Survey (3 240314 220858Document67 pagesMelanoma Classification A Comprehensive Survey (3 240314 220858Kovid AggarwalNo ratings yet
- Patch Testing and Prick Testing: A Practical Guide Official Publication of the ICDRGFrom EverandPatch Testing and Prick Testing: A Practical Guide Official Publication of the ICDRGNo ratings yet
- Development and Validation of Stability Indicating Assay Method For Estimation of Teriflunomide in Tablet Dosage FormDocument11 pagesDevelopment and Validation of Stability Indicating Assay Method For Estimation of Teriflunomide in Tablet Dosage FormBaru Chandrasekhar RaoNo ratings yet
- Analytical Method Development and Validation of Stability Indicating RP-HPLC Method For Estimation of Lercanidipine Hydrochloride and Enalapril Maleate in CombinationDocument8 pagesAnalytical Method Development and Validation of Stability Indicating RP-HPLC Method For Estimation of Lercanidipine Hydrochloride and Enalapril Maleate in CombinationBaru Chandrasekhar RaoNo ratings yet
- Relationship of Testosterone With Body Mass Index in Infertile Males in Local CommunityDocument4 pagesRelationship of Testosterone With Body Mass Index in Infertile Males in Local CommunityBaru Chandrasekhar RaoNo ratings yet
- Gastroprotective Activity of Methanolic Extract of Phyllanthus Acidus Fruit Against Indomethacin-Induced Gastric Ulcers in RatsDocument7 pagesGastroprotective Activity of Methanolic Extract of Phyllanthus Acidus Fruit Against Indomethacin-Induced Gastric Ulcers in RatsBaru Chandrasekhar RaoNo ratings yet
- Knowledge On Antibiotics Use and Its Storage Among Saudi Arabia Residents: A Cross Sectional StudyDocument8 pagesKnowledge On Antibiotics Use and Its Storage Among Saudi Arabia Residents: A Cross Sectional StudyBaru Chandrasekhar RaoNo ratings yet
- A Brief Review On YawsDocument7 pagesA Brief Review On YawsBaru Chandrasekhar RaoNo ratings yet
- Review On: Inventory ManagementDocument8 pagesReview On: Inventory ManagementBaru Chandrasekhar RaoNo ratings yet
- Pharmaceutical Sciences: IAJPS 2018, 05 (04), 3075-3081 Aneeqa Ali RaoDocument7 pagesPharmaceutical Sciences: IAJPS 2018, 05 (04), 3075-3081 Aneeqa Ali RaoBaru Chandrasekhar RaoNo ratings yet
- Assessment of Correlation Between Physical Activity and Academic Performance Among The Students of Gujranwala Medical College, GujranwalaDocument7 pagesAssessment of Correlation Between Physical Activity and Academic Performance Among The Students of Gujranwala Medical College, GujranwalaBaru Chandrasekhar RaoNo ratings yet
- Descriptive Study Knowing The Patients Load in The Neonatal Icu at The Tertiary Care Hospital LahoreDocument4 pagesDescriptive Study Knowing The Patients Load in The Neonatal Icu at The Tertiary Care Hospital LahoreBaru Chandrasekhar RaoNo ratings yet
- The Role of Clinical Pharmacist in Pharmacovigilance and Drug Safety in Teritiary Care Teaching HospitalDocument11 pagesThe Role of Clinical Pharmacist in Pharmacovigilance and Drug Safety in Teritiary Care Teaching HospitalBaru Chandrasekhar RaoNo ratings yet
- Pharmacological and Phytochemical Evidence of Scutia Genus Plants - A ReviewDocument7 pagesPharmacological and Phytochemical Evidence of Scutia Genus Plants - A ReviewBaru Chandrasekhar RaoNo ratings yet
- DISTINCTIVE PHARMACOLOGICAL ACTIVITIES OF Eclipta Alba AND IT'S COUMESTAN WEDELOLACTONEDocument7 pagesDISTINCTIVE PHARMACOLOGICAL ACTIVITIES OF Eclipta Alba AND IT'S COUMESTAN WEDELOLACTONEBaru Chandrasekhar RaoNo ratings yet
- DETERMINATION OF BIOACTIVE COMPOUNDS FROM Piper Nigrum. L BY USING HPLC ANALYSISDocument3 pagesDETERMINATION OF BIOACTIVE COMPOUNDS FROM Piper Nigrum. L BY USING HPLC ANALYSISBaru Chandrasekhar RaoNo ratings yet
- Determination of Bioactive Compounds From Piper Nigrum L by Using Ft-Ir Spectroscopic AnalysisDocument3 pagesDetermination of Bioactive Compounds From Piper Nigrum L by Using Ft-Ir Spectroscopic AnalysisBaru Chandrasekhar RaoNo ratings yet
- RP-HPLC Method Development and Validation of Alogliptin Bulk and Tablet Dosage FormDocument8 pagesRP-HPLC Method Development and Validation of Alogliptin Bulk and Tablet Dosage FormBaru Chandrasekhar RaoNo ratings yet
- STUDIES ON QUALITATIVE PHYTOCHEMICAL ANALYSIS AND ANTIBACTERIAL ACTIVITY OF Piper NigrumDocument7 pagesSTUDIES ON QUALITATIVE PHYTOCHEMICAL ANALYSIS AND ANTIBACTERIAL ACTIVITY OF Piper NigrumBaru Chandrasekhar RaoNo ratings yet
- Determination of Bioactive Compounds From Piper Longum L. by Using HP-LC AnalysisDocument4 pagesDetermination of Bioactive Compounds From Piper Longum L. by Using HP-LC AnalysisBaru Chandrasekhar RaoNo ratings yet
- Blood Products and Their UsesDocument28 pagesBlood Products and Their UsesJeevitha Vanitha100% (1)
- Flow Chart Showng Evalution in Community Medicine: Mbbs Third ProfessionalDocument9 pagesFlow Chart Showng Evalution in Community Medicine: Mbbs Third ProfessionalusamaNo ratings yet
- Admission Notice For General PublicDocument6 pagesAdmission Notice For General Publicmoney moneyNo ratings yet
- Respiratory System: Copd (Bronchitis & Emphysema)Document7 pagesRespiratory System: Copd (Bronchitis & Emphysema)Rhea Lyn LamosteNo ratings yet
- Immature GranulocytesDocument10 pagesImmature Granulocytespieterinpretoria391No ratings yet
- Screenshot 2023-12-11 at 3.53.36 PMDocument62 pagesScreenshot 2023-12-11 at 3.53.36 PMahmedmansi055No ratings yet
- Golden Hour of Neonatal Life - Need of The HourDocument21 pagesGolden Hour of Neonatal Life - Need of The HourEdwin AlvarezNo ratings yet
- CSR Activities of LUPIN LTDDocument12 pagesCSR Activities of LUPIN LTDVishal SinghNo ratings yet
- Comparison of Modified Borg Scale and Visual Analog Scale Dyspnea Scores in Predicting Re-Intervention After Drainage of Malignant Pleural EffusionDocument8 pagesComparison of Modified Borg Scale and Visual Analog Scale Dyspnea Scores in Predicting Re-Intervention After Drainage of Malignant Pleural EffusionMukhlis HasNo ratings yet
- PsychosisDocument11 pagesPsychosisChan's RoomNo ratings yet
- Augmentin DuoDocument2 pagesAugmentin Duojunaid hashmiNo ratings yet
- 26 ProtozoaDocument74 pages26 ProtozoaCalvin BlueNo ratings yet
- Air Pollution in QuitoDocument14 pagesAir Pollution in Quitoapi-385158934No ratings yet
- Chinese Exclusion Act 1f4nr0kDocument17 pagesChinese Exclusion Act 1f4nr0kbald bullNo ratings yet
- Complete Catalog Row0704Document175 pagesComplete Catalog Row0704Krish GulabaniNo ratings yet
- Slide Master Apm CPR N AedDocument46 pagesSlide Master Apm CPR N AedDivyaaNo ratings yet
- Puerperal SepsisDocument30 pagesPuerperal Sepsisjonaa2564No ratings yet
- Psychoanalysis of Gifted Minds PSYDocument12 pagesPsychoanalysis of Gifted Minds PSYVirat SinghNo ratings yet
- Field Visit Report To Vrindavan Botanical Garden and Lumle Regional Agricultural Research StationDocument43 pagesField Visit Report To Vrindavan Botanical Garden and Lumle Regional Agricultural Research StationAmresh kumar Shah100% (1)
- Cefepime Vs Zosyn For Empiric Sepsis CoverageDocument2 pagesCefepime Vs Zosyn For Empiric Sepsis Coveragetl drNo ratings yet
- Amyotrophic Lateral SclerosisDocument23 pagesAmyotrophic Lateral SclerosisAfshan Pt T100% (1)
- Malunggay Leaf Extracts As An AlternativDocument57 pagesMalunggay Leaf Extracts As An AlternativGrilhamon ShenNo ratings yet
- 1 s2.0 S0740002020301337 MainDocument9 pages1 s2.0 S0740002020301337 MainIggjchthfx JcytxutxutxtjNo ratings yet
- Rudiyanto, Liver FibrosisDocument41 pagesRudiyanto, Liver Fibrosisbudi darmantaNo ratings yet
- Three-Part EssayDocument1 pageThree-Part EssayLovely CastroNo ratings yet
- Annals of General Psychiatry: Hospital Anxiety and Depression Scale (HADS) : Validation in A Greek General Hospital SampleDocument5 pagesAnnals of General Psychiatry: Hospital Anxiety and Depression Scale (HADS) : Validation in A Greek General Hospital SampleGeraldo Antonio GranzottoNo ratings yet