Download as doc, pdf, or txt
You might also like
- Cl-Molec Cap Assay Check ListDocument74 pagesCl-Molec Cap Assay Check ListAndreína Gabriela Sánchez González0% (1)
- 025 SOP Cobas E411 SOPDocument13 pages025 SOP Cobas E411 SOPrehab rabea100% (1)
- Urinalysis 2021Document17 pagesUrinalysis 2021Tanu BhatiaNo ratings yet
- Case Study Discussion Blok Urin 2014-2015docxDocument5 pagesCase Study Discussion Blok Urin 2014-2015docxEdita DevanaNo ratings yet
- (Clinical Cases Uncovered) - CARDIOLOGY - (2010) - Halaman-202-207Document6 pages(Clinical Cases Uncovered) - CARDIOLOGY - (2010) - Halaman-202-207zizaNo ratings yet
- DownloadsPro68-01 Manual Urin Micro SOPDocument19 pagesDownloadsPro68-01 Manual Urin Micro SOPInn MironNo ratings yet
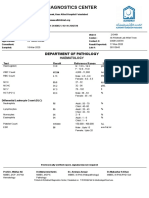
- Al-Khidmat Diagnostics Center: Department of PathologyDocument1 pageAl-Khidmat Diagnostics Center: Department of PathologyKiran HassanNo ratings yet
- 3.3.2 Anti HCV Testing (Rapid Method)Document4 pages3.3.2 Anti HCV Testing (Rapid Method)BALAJINo ratings yet
- Standard Operating Procedure (Haematology) : R. K. Life Services Private LimitedDocument61 pagesStandard Operating Procedure (Haematology) : R. K. Life Services Private LimitedAniruddha ChatterjeeNo ratings yet
- QC-7 Hematology Westgard Rules in Good Performance LaboratoryDocument38 pagesQC-7 Hematology Westgard Rules in Good Performance LaboratoryWita100% (1)
- KKHL c6 SP 03 Sop For Iqc and Eqa Final 1Document23 pagesKKHL c6 SP 03 Sop For Iqc and Eqa Final 1GABULA MIKENo ratings yet
- ISO 15189 - 2012 Technical RequirementsDocument104 pagesISO 15189 - 2012 Technical RequirementsAhmed AdemNo ratings yet
- Laboratory Testing Turn-Around Times PolicyDocument5 pagesLaboratory Testing Turn-Around Times PolicyGHL AdaroNo ratings yet
- Physical ExamDocument14 pagesPhysical ExamAl Ge IrNo ratings yet
- Job Description:: Phlebotomists DutiesDocument7 pagesJob Description:: Phlebotomists DutiesRajeev PareekNo ratings yet
- Quality Control in Blood BankDocument46 pagesQuality Control in Blood BankTanyaNo ratings yet
- Lab Policies Complete Blood Count of Whole Blood On The Sysmex KX 21N - RB Lab 1535Document20 pagesLab Policies Complete Blood Count of Whole Blood On The Sysmex KX 21N - RB Lab 1535tomNo ratings yet
- Laboratory Tests For EndocrinologyDocument6 pagesLaboratory Tests For EndocrinologyAnastasia100% (1)
- Hem Lab Manual DiffDocument9 pagesHem Lab Manual DiffFatima Mae LusanNo ratings yet
- Whole Blood Analysis (Full Blood Count-FBC) Using SYSMEX XE-2100 Haematology Automated AnalyserDocument16 pagesWhole Blood Analysis (Full Blood Count-FBC) Using SYSMEX XE-2100 Haematology Automated AnalyserFULGENCE RUHARARANo ratings yet
- Packed Cell Volume (PCV) TestDocument3 pagesPacked Cell Volume (PCV) TestchineduNo ratings yet
- I STATDocument24 pagesI STATPraveen RamasamyNo ratings yet
- Content: Standard Operating Procedure (SOP) Use and Maintenance of A CentrifugeDocument9 pagesContent: Standard Operating Procedure (SOP) Use and Maintenance of A CentrifugenazmiNo ratings yet
- Quality Control2Document32 pagesQuality Control2Mustafa KhandgawiNo ratings yet
- Unsuccessful VenipunctureDocument6 pagesUnsuccessful Venipuncturehatemfarouk50% (2)
- POCT and PT by Group6bsmt3bDocument15 pagesPOCT and PT by Group6bsmt3bRuzzelle Mae ParasNo ratings yet
- Lab Policies Urinalysis - Clinetek Status and Visual Lab 1583Document17 pagesLab Policies Urinalysis - Clinetek Status and Visual Lab 1583hunnylandNo ratings yet
- Client Feedback FormDocument4 pagesClient Feedback FormASHLEE DADOR FERRERNo ratings yet
- Sample: Interference Testing in Clinical Chemistry Approved Guideline-Second EditionDocument12 pagesSample: Interference Testing in Clinical Chemistry Approved Guideline-Second EditionSvetlana MorozovaNo ratings yet
- CSF and Synovial FluidDocument12 pagesCSF and Synovial Fluidquerokeropi100% (1)
- Sop HemaDocument10 pagesSop HemaRochell OcampoNo ratings yet
- Usman FRCPath An Overview of Examination Requirments 1Document56 pagesUsman FRCPath An Overview of Examination Requirments 1Asma Umair100% (1)
- Chapter 14 - Routine and Point of Care Testing in HematologyDocument10 pagesChapter 14 - Routine and Point of Care Testing in HematologyNathaniel Sim100% (1)
- 301 Examination of Peripheral SmearDocument13 pages301 Examination of Peripheral SmearSilpa ThotaNo ratings yet
- Point of Care TestingDocument40 pagesPoint of Care TestingPrincewill Seiyefa100% (1)
- Quality Control in A Clinical LaboratoryDocument9 pagesQuality Control in A Clinical LaboratoryHenry OseiNo ratings yet
- Policy Critical ResultDocument6 pagesPolicy Critical ResultSafiqulatif AbdillahNo ratings yet
- Clinical Chemistry - SamplesDocument105 pagesClinical Chemistry - SamplesSamar SharafNo ratings yet
- Introduction of Clinical BiochemistryDocument32 pagesIntroduction of Clinical BiochemistryKaren LowNo ratings yet
- Rapid Plasma Reagin (RPR)Document7 pagesRapid Plasma Reagin (RPR)Gakwaya Jules CesarNo ratings yet
- Laboratory SOPsDocument286 pagesLaboratory SOPsMohamed Annavi100% (1)
- Blood Bank ManualDocument29 pagesBlood Bank ManualMarice Ferrufino SchmidtNo ratings yet
- 03 - SOP Clinical PathologyDocument88 pages03 - SOP Clinical PathologyKailash PrajapatNo ratings yet
- Piccolo Xpress Chemistry Analyser SOPDocument16 pagesPiccolo Xpress Chemistry Analyser SOPBahamas Wellness Diagnostic ServicesNo ratings yet
- Quality Assurance in Hematology Group 11Document51 pagesQuality Assurance in Hematology Group 11Mandy A. DelfinNo ratings yet
- Primary Sample Collection Manual GD-QSPMDocument51 pagesPrimary Sample Collection Manual GD-QSPMLalit Surykant Chavan100% (1)
- Centrifuge Maintenance SopDocument6 pagesCentrifuge Maintenance Sopkavaim001No ratings yet
- Lab - Report - BHAVISHKA JIDocument4 pagesLab - Report - BHAVISHKA JIYogeshKumarLoharNo ratings yet
- Critical Result ReportingDocument9 pagesCritical Result ReportingSafiqulatif AbdillahNo ratings yet
- Quality Assurance in Hemat LabsDocument38 pagesQuality Assurance in Hemat LabsSmriti Dwivedi SharmaNo ratings yet
- IQCPDocument1 pageIQCPPrabhu Selvaraj100% (1)
- Fuji Dri-Chem Slide: Tcho-PiiiDocument1 pageFuji Dri-Chem Slide: Tcho-Piiisusey tepaNo ratings yet
- Basics of Laboratory Internal Quality Control, Ola ElgaddarDocument27 pagesBasics of Laboratory Internal Quality Control, Ola ElgaddarOla ElgaddarNo ratings yet
- Laboratory ScopesDocument67 pagesLaboratory ScopesNash Si100% (1)
- Quality Management Training For Blood Transfusion Services: EHT/05.03 A RestrictedDocument86 pagesQuality Management Training For Blood Transfusion Services: EHT/05.03 A RestrictedindrajeetNo ratings yet
- Evaluation Reporting of ResultsDocument16 pagesEvaluation Reporting of ResultspurnachandrashekarNo ratings yet
- BLOOD TYPING and RH TYPING TUBE METHOD PROCEDURESDocument1 pageBLOOD TYPING and RH TYPING TUBE METHOD PROCEDURESmichael mannNo ratings yet
- Sop For Abo GroupingDocument10 pagesSop For Abo GroupingMohd Fekharudin Mahmud75% (4)
- Laboratory Quality Control A Complete Guide - 2020 EditionFrom EverandLaboratory Quality Control A Complete Guide - 2020 EditionNo ratings yet
- Pro68-01 Manual Urin Micro SOPDocument20 pagesPro68-01 Manual Urin Micro SOPesraa asemNo ratings yet
- Routine UrinalysisDocument2 pagesRoutine UrinalysisSkylar MendesNo ratings yet
- Exercise Adherence Rating ScaleDocument6 pagesExercise Adherence Rating ScalemadhumidhaNo ratings yet
- Process Flow For Issuance of Medical Clearance For PCG Applicants (2021)Document4 pagesProcess Flow For Issuance of Medical Clearance For PCG Applicants (2021)Aljen Rey BuenafeNo ratings yet
- Detection of Typhoid CarriersDocument6 pagesDetection of Typhoid CarriersClarestaNo ratings yet
- PMLS2 - Week 3Document1 pagePMLS2 - Week 3MA. ANDREA NICOLE DURANNo ratings yet
- Practical Research 2 Q2Module 2Document5 pagesPractical Research 2 Q2Module 2Florene Bhon GumapacNo ratings yet
- Part I TB Data Project RedoDocument2 pagesPart I TB Data Project Redoapi-583813179No ratings yet
- Guideline On General Principles of Process ValidationDocument23 pagesGuideline On General Principles of Process ValidationI-Sun Deep Mohan TeaNo ratings yet
- MDCG 2022-6Document17 pagesMDCG 2022-6md edaNo ratings yet
- Mythic 60Document2 pagesMythic 60yogesh kumarNo ratings yet
- Utility Hazard AssessmentDocument2 pagesUtility Hazard AssessmentsafwanNo ratings yet
- Radiologic Technologists and X-Ray Technologists 12-2021Document24 pagesRadiologic Technologists and X-Ray Technologists 12-2021PRC Baguio100% (1)
- Work Permit SystemDocument50 pagesWork Permit SystemBin khammash and sons Co.No ratings yet
- C54ADocument64 pagesC54Arehaaam.abdullahNo ratings yet
- Nursing Process: Mrs. Sumaira Noreen Senior Nursing InstructorDocument40 pagesNursing Process: Mrs. Sumaira Noreen Senior Nursing InstructorSumaira NoreenNo ratings yet
- CAPTODAY - Urinalysis TrendsDocument6 pagesCAPTODAY - Urinalysis Trendsalexandre larmagnacNo ratings yet
- Name of Patient: Age: Sex: Ward/room: Diagnosis: Proposed Operation: Anesthesia: Anesthesiologist: SurgeonDocument2 pagesName of Patient: Age: Sex: Ward/room: Diagnosis: Proposed Operation: Anesthesia: Anesthesiologist: SurgeonJan Federick Bantay100% (3)
- AUOBF Manual Activity 3Document6 pagesAUOBF Manual Activity 3Francis ValdezNo ratings yet
- RM Practice Questions Inferential Statistics MainlyDocument24 pagesRM Practice Questions Inferential Statistics MainlyGhalia DoshanNo ratings yet
- ISO 15189 DraftDocument76 pagesISO 15189 DraftAM100% (1)
- 2 (B) Food SafetyDocument4 pages2 (B) Food SafetyDanial IqhwanNo ratings yet
- Onsite APE 2022 GuidelinesDocument6 pagesOnsite APE 2022 GuidelinesAXIS CORPORATIONNo ratings yet
- Activity 1 Serial Dilution NEWDocument7 pagesActivity 1 Serial Dilution NEWJoshua Richard Jr Tubiano PayopaninNo ratings yet
- Worksheet - RLE 1 Significance of Laboratory ResultsDocument9 pagesWorksheet - RLE 1 Significance of Laboratory Results1H - Althea VestilNo ratings yet
- EoI For Franchisee & Business Associates For NEDocument7 pagesEoI For Franchisee & Business Associates For NESarath MenonNo ratings yet
- Piedmont Authorization Form FIT TestDocument1 pagePiedmont Authorization Form FIT Testodurden02No ratings yet
- Scaffolding: External Referral Draft 19 December 2012Document38 pagesScaffolding: External Referral Draft 19 December 2012Azad pravesh khanNo ratings yet
- Name - 8-Part Eye Exam ChecklistDocument2 pagesName - 8-Part Eye Exam Checklistrubie ann tillor100% (1)
- Urinalysis Procedure N21 Desiata, LyrizzaDocument3 pagesUrinalysis Procedure N21 Desiata, LyrizzaLYRIZZA LEA BHEA DESIATANo ratings yet
- Assessment of The Ear and Hearing AcuityDocument3 pagesAssessment of The Ear and Hearing AcuityJay Debby RuizoNo ratings yet