
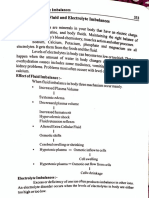
Electrolyte Imbalances
Electrolyte Imbalances
You might also like
- Predictions OnlyDocument89 pagesPredictions OnlyJan Crizza Dale R. Franco73% (11)
- Clinical Chemistry 2 LAB MT305 Rlh3: ElectrolytesDocument2 pagesClinical Chemistry 2 LAB MT305 Rlh3: ElectrolytesEmiaj Francinne Mendoza100% (2)
- ATI Fluids, AcidBase, DietsDocument9 pagesATI Fluids, AcidBase, DietsBernardo AntonioNo ratings yet
- Sodium Potassium Imbalances MedsurgDocument5 pagesSodium Potassium Imbalances Medsurgchi kNo ratings yet
- Medical Surgical Nursing Fluids Electrolytes Acid Base ImbalanceDocument11 pagesMedical Surgical Nursing Fluids Electrolytes Acid Base ImbalanceAlaa OmarNo ratings yet
- Med Surg Study GuideDocument24 pagesMed Surg Study Guidekylie100% (4)
- Fe Finals NotesDocument23 pagesFe Finals NoteshanhananicasNo ratings yet
- Electrolytes LecDocument4 pagesElectrolytes LecMichelle San Miguel FeguroNo ratings yet
- SAJAA (V27) p126-130 2691 FCA SupplementDocument5 pagesSAJAA (V27) p126-130 2691 FCA SupplementVivek PatangeNo ratings yet
- Fluids & Electrolytes: Nio Cruzada Noveno, RN, MAN, MSNDocument66 pagesFluids & Electrolytes: Nio Cruzada Noveno, RN, MAN, MSNapi-19824701No ratings yet
- HYPONATREMIADocument8 pagesHYPONATREMIAfilescrocsNo ratings yet
- Adrenal GlandDocument1 pageAdrenal GlandAfiera MurpiNo ratings yet
- Primary: Congenital Disease 2. Finnish Nephrotic Syndrome (Inherited) 3. Nephrotic Syndrome Minimal Change (The Most Common Type)Document6 pagesPrimary: Congenital Disease 2. Finnish Nephrotic Syndrome (Inherited) 3. Nephrotic Syndrome Minimal Change (The Most Common Type)Cici Novelia ManurungNo ratings yet
- Primary: Congenital Disease 2. Finnish Nephrotic Syndrome (Inherited) 3. Nephrotic Syndrome Minimal Change (The Most Common Type)Document6 pagesPrimary: Congenital Disease 2. Finnish Nephrotic Syndrome (Inherited) 3. Nephrotic Syndrome Minimal Change (The Most Common Type)Cici Novelia ManurungNo ratings yet
- Management of Electrolyte ImbalanceDocument77 pagesManagement of Electrolyte ImbalanceSatyajit SwainNo ratings yet
- Week 2 Electrolyte Imbalance Group Work INSTRUCTOR 1 PDFDocument8 pagesWeek 2 Electrolyte Imbalance Group Work INSTRUCTOR 1 PDFMaica LectanaNo ratings yet
- Felixcharlie Electrolyte Homeostasis Part 3Document3 pagesFelixcharlie Electrolyte Homeostasis Part 3Nur Fatima SanaaniNo ratings yet
- CDLec and FluidsEABB CompiledDocument12 pagesCDLec and FluidsEABB CompiledJuana ToriomNo ratings yet
- CC2 Midterm Electrocytes 111Document10 pagesCC2 Midterm Electrocytes 111jacquelinebiteranta13No ratings yet
- NCM112 LP1 Transes - RosalesDocument4 pagesNCM112 LP1 Transes - RosalesChristine CalleyNo ratings yet
- Fluid and Electrolyte ManagementDocument2 pagesFluid and Electrolyte ManagementАчпже ЧпжечуNo ratings yet
- ELECTROLYTES Clinica SignificanceDocument6 pagesELECTROLYTES Clinica SignificanceKim Mae ComendadorNo ratings yet
- Fluids and Electrolytes: PGI Pat JacintoDocument21 pagesFluids and Electrolytes: PGI Pat JacintoPat JacintoNo ratings yet
- Dietary Management - Renal DisordersDocument8 pagesDietary Management - Renal DisordersReanne Mae AbreraNo ratings yet
- Drug StudyDocument21 pagesDrug StudyRhuby Pascual AbenojaNo ratings yet
- Fluids and Electrolytes Part 1Document4 pagesFluids and Electrolytes Part 1baraderoayyah41No ratings yet
- Fluid and Electrolytes NCM 109Document3 pagesFluid and Electrolytes NCM 109syroise margauxNo ratings yet
- Micronutrients: Water & ElectrolytesDocument2 pagesMicronutrients: Water & ElectrolytesRANDY ERNEST GESTOSANINo ratings yet
- Fluid & Electrolyte, Acid-Base Imbalance (MS REPORT)Document41 pagesFluid & Electrolyte, Acid-Base Imbalance (MS REPORT)Jane BelvisNo ratings yet
- AG BP Exam1Document21 pagesAG BP Exam1katelynricki14No ratings yet
- Chloride ImbalancesDocument2 pagesChloride ImbalancesBruce EstilloteNo ratings yet
- Study Guide 9 Fluids Electrolytes Acid Base Balance For StudentsDocument10 pagesStudy Guide 9 Fluids Electrolytes Acid Base Balance For StudentsliahekuriNo ratings yet
- Fluids and ElectrolylesDocument12 pagesFluids and ElectrolylesTine GuibaoNo ratings yet
- FE Imbalance HandoutsDocument2 pagesFE Imbalance HandoutsPrasanth Kurien Mathew100% (2)
- NCM 112 Fluid and ElectrolytesDocument2 pagesNCM 112 Fluid and ElectrolytesAngeline NavarroNo ratings yet
- Fluids and Electrolytes NotesDocument17 pagesFluids and Electrolytes NotesFaye G.No ratings yet
- Fluid and ElectrolyteDocument4 pagesFluid and Electrolytevaibhav nigamNo ratings yet
- Electrolyte DisordersDocument29 pagesElectrolyte Disorderssanketh bhat.sNo ratings yet
- M1 - F&eDocument2 pagesM1 - F&ejuiceNo ratings yet
- Midterms - Electrolyte Renal DisordersDocument40 pagesMidterms - Electrolyte Renal DisordersRachelle DelantarNo ratings yet
- PEDIA REPORT - Fluids and ElectrolytesDocument47 pagesPEDIA REPORT - Fluids and ElectrolytesFaydhal SalikNo ratings yet
- Hyponatremia in Children (PICU COURSE)Document83 pagesHyponatremia in Children (PICU COURSE)surasuarezlopezNo ratings yet
- DR Saroj PandaDocument45 pagesDR Saroj PandaPranshu Prajyot 67No ratings yet
- English of NursingDocument1 pageEnglish of NursingyustiNo ratings yet
- Quiz 1Document3 pagesQuiz 1Wiljohn de la CruzNo ratings yet
- Fluid and Electrolyte in InfantDocument44 pagesFluid and Electrolyte in InfantVibin K vNo ratings yet
- ELECTROLYTES EditedDocument6 pagesELECTROLYTES EditedKrystel Bea DinqueNo ratings yet
- Chapter 5-Inorganic ChemDocument5 pagesChapter 5-Inorganic ChemMark Harold GonzalesNo ratings yet
- Anaphy Lec IDocument3 pagesAnaphy Lec IKrishna LibrodoNo ratings yet
- Fluidandelectrolyte TodayDocument76 pagesFluidandelectrolyte TodayPrithvi MagarNo ratings yet
- Chapter 34 - PolyuriaDocument6 pagesChapter 34 - Polyuriajonalyn.mejellanoNo ratings yet
- The Most Commonly Ordered (Chemistry) Laboratory InvestigationsDocument94 pagesThe Most Commonly Ordered (Chemistry) Laboratory InvestigationsZEESHAN YOUSUFNo ratings yet
- MidtermsDocument40 pagesMidtermsSteph CaronanNo ratings yet
- Fluids PDFDocument26 pagesFluids PDFLeogalvez BedanoNo ratings yet
- Drug StudyDocument7 pagesDrug StudyBella Cy LopezNo ratings yet
- Prof. Sandra M. Covarrubias - September 24, 2021: 5.2fluid & Electrolytes ImbalancesDocument5 pagesProf. Sandra M. Covarrubias - September 24, 2021: 5.2fluid & Electrolytes ImbalancesIvy VillalobosNo ratings yet
- Electrolyte Imbalances ReviewerDocument14 pagesElectrolyte Imbalances ReviewerhoneyNo ratings yet
- Fluids & Elec. 3Document87 pagesFluids & Elec. 3Krystal AliñabonNo ratings yet
- Disorders-Of-Sodium-Balance - CAMBRIDGEDocument10 pagesDisorders-Of-Sodium-Balance - CAMBRIDGEDenisa Carmen ColiofNo ratings yet
- Group 4 Final Paper Bacterial OrganismDocument55 pagesGroup 4 Final Paper Bacterial OrganismRodriguez, Jhe-ann M.No ratings yet
- Doon Institute of Medical Science2 (Exam Paper)Document3 pagesDoon Institute of Medical Science2 (Exam Paper)Shaila PanchalNo ratings yet
- Escherichia Coli 1. Definition of Escherichia ColiDocument6 pagesEscherichia Coli 1. Definition of Escherichia Coliwiwi oktafianiNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Siva ShanmugamNo ratings yet
- Stress and Periodontal Disease PDFDocument7 pagesStress and Periodontal Disease PDFDaniela RusnacNo ratings yet
- 4 - Rohini Nakshatra Padas in Ravana SamhitaDocument15 pages4 - Rohini Nakshatra Padas in Ravana SamhitaMarilou1963No ratings yet
- Parainfluenza Viruses in Adults - UpToDateDocument25 pagesParainfluenza Viruses in Adults - UpToDateMisael TaverasNo ratings yet
- Balance de LiquidosDocument8 pagesBalance de LiquidosAhira Susana Mendoza de RiveraNo ratings yet
- Eating Fruits - The Correct WayDocument5 pagesEating Fruits - The Correct WayNimesh Shah100% (2)
- Genetic Disorders AVN 24 12 2020Document17 pagesGenetic Disorders AVN 24 12 2020MuskanNo ratings yet
- G6PD Deficiency Group 6Document36 pagesG6PD Deficiency Group 6Christian Darwin Llanes100% (2)
- Intra Uterine Growth RetardationDocument46 pagesIntra Uterine Growth RetardationIba Ghannam100% (1)
- Acute Gastroenteritis: Brigitte Ulrike D. Tabaranza M.DDocument65 pagesAcute Gastroenteritis: Brigitte Ulrike D. Tabaranza M.DChandice CuaNo ratings yet
- Pathophysiology Cholelithiasis 2Document2 pagesPathophysiology Cholelithiasis 2Jamie HaravataNo ratings yet
- Paper IX MCQ Set ADocument3 pagesPaper IX MCQ Set AHimanshu KarmacharyaNo ratings yet
- Willemsen 2012Document13 pagesWillemsen 2012EstebanGiraNo ratings yet
- Ismail's Undergraduate ThesisDocument82 pagesIsmail's Undergraduate ThesisAbiola IbrahimNo ratings yet
- Health and Safety Protocols: Dr. Michael Bautista Dr. Ethyl Salvador-CayetanoDocument35 pagesHealth and Safety Protocols: Dr. Michael Bautista Dr. Ethyl Salvador-CayetanoJordz PlaciNo ratings yet
- (2020) Glycyrrhiza Glabra (Licorice)Document10 pages(2020) Glycyrrhiza Glabra (Licorice)icaNo ratings yet
- Health Psychology Canadian 4th Edition Taylor Test BankDocument13 pagesHealth Psychology Canadian 4th Edition Taylor Test BankJosephWilliamsinaom100% (12)
- 100014Z09JM2016 Mathew PDFDocument7 pages100014Z09JM2016 Mathew PDFRameshKrishnanNo ratings yet
- Mnemonics Definitions PDFDocument6 pagesMnemonics Definitions PDFsaquib eqbalNo ratings yet
- Ir Choice Board 1Document1 pageIr Choice Board 1api-621945476No ratings yet
- Microbiology First Exam - Past Year QDocument7 pagesMicrobiology First Exam - Past Year QNabilah Mohd YaakobNo ratings yet
- Physical EducationDocument3 pagesPhysical EducationusunomNo ratings yet
- Medical Ethics 2023 FINALDocument56 pagesMedical Ethics 2023 FINALBelinda ELISHANo ratings yet
- COVID 19 - Clinical Picture in The Elderly Population: A Qualitative Systematic ReviewDocument21 pagesCOVID 19 - Clinical Picture in The Elderly Population: A Qualitative Systematic ReviewRila RivandaNo ratings yet
- 203 Health DefinitionDocument20 pages203 Health DefinitionJodi BrutonNo ratings yet
- Psychoactive Drugs and Transactional Analysis PDFDocument7 pagesPsychoactive Drugs and Transactional Analysis PDFAlex LenkemzNo ratings yet






















































































Download as docx, pdf, or txt
You might also like
- Predictions OnlyDocument89 pagesPredictions OnlyJan Crizza Dale R. Franco73% (11)
- Clinical Chemistry 2 LAB MT305 Rlh3: ElectrolytesDocument2 pagesClinical Chemistry 2 LAB MT305 Rlh3: ElectrolytesEmiaj Francinne Mendoza100% (2)
- ATI Fluids, AcidBase, DietsDocument9 pagesATI Fluids, AcidBase, DietsBernardo AntonioNo ratings yet
- Sodium Potassium Imbalances MedsurgDocument5 pagesSodium Potassium Imbalances Medsurgchi kNo ratings yet
- Medical Surgical Nursing Fluids Electrolytes Acid Base ImbalanceDocument11 pagesMedical Surgical Nursing Fluids Electrolytes Acid Base ImbalanceAlaa OmarNo ratings yet
- Med Surg Study GuideDocument24 pagesMed Surg Study Guidekylie100% (4)
- Fe Finals NotesDocument23 pagesFe Finals NoteshanhananicasNo ratings yet
- Electrolytes LecDocument4 pagesElectrolytes LecMichelle San Miguel FeguroNo ratings yet
- SAJAA (V27) p126-130 2691 FCA SupplementDocument5 pagesSAJAA (V27) p126-130 2691 FCA SupplementVivek PatangeNo ratings yet
- Fluids & Electrolytes: Nio Cruzada Noveno, RN, MAN, MSNDocument66 pagesFluids & Electrolytes: Nio Cruzada Noveno, RN, MAN, MSNapi-19824701No ratings yet
- HYPONATREMIADocument8 pagesHYPONATREMIAfilescrocsNo ratings yet
- Adrenal GlandDocument1 pageAdrenal GlandAfiera MurpiNo ratings yet
- Primary: Congenital Disease 2. Finnish Nephrotic Syndrome (Inherited) 3. Nephrotic Syndrome Minimal Change (The Most Common Type)Document6 pagesPrimary: Congenital Disease 2. Finnish Nephrotic Syndrome (Inherited) 3. Nephrotic Syndrome Minimal Change (The Most Common Type)Cici Novelia ManurungNo ratings yet
- Primary: Congenital Disease 2. Finnish Nephrotic Syndrome (Inherited) 3. Nephrotic Syndrome Minimal Change (The Most Common Type)Document6 pagesPrimary: Congenital Disease 2. Finnish Nephrotic Syndrome (Inherited) 3. Nephrotic Syndrome Minimal Change (The Most Common Type)Cici Novelia ManurungNo ratings yet
- Management of Electrolyte ImbalanceDocument77 pagesManagement of Electrolyte ImbalanceSatyajit SwainNo ratings yet
- Week 2 Electrolyte Imbalance Group Work INSTRUCTOR 1 PDFDocument8 pagesWeek 2 Electrolyte Imbalance Group Work INSTRUCTOR 1 PDFMaica LectanaNo ratings yet
- Felixcharlie Electrolyte Homeostasis Part 3Document3 pagesFelixcharlie Electrolyte Homeostasis Part 3Nur Fatima SanaaniNo ratings yet
- CDLec and FluidsEABB CompiledDocument12 pagesCDLec and FluidsEABB CompiledJuana ToriomNo ratings yet
- CC2 Midterm Electrocytes 111Document10 pagesCC2 Midterm Electrocytes 111jacquelinebiteranta13No ratings yet
- NCM112 LP1 Transes - RosalesDocument4 pagesNCM112 LP1 Transes - RosalesChristine CalleyNo ratings yet
- Fluid and Electrolyte ManagementDocument2 pagesFluid and Electrolyte ManagementАчпже ЧпжечуNo ratings yet
- ELECTROLYTES Clinica SignificanceDocument6 pagesELECTROLYTES Clinica SignificanceKim Mae ComendadorNo ratings yet
- Fluids and Electrolytes: PGI Pat JacintoDocument21 pagesFluids and Electrolytes: PGI Pat JacintoPat JacintoNo ratings yet
- Dietary Management - Renal DisordersDocument8 pagesDietary Management - Renal DisordersReanne Mae AbreraNo ratings yet
- Drug StudyDocument21 pagesDrug StudyRhuby Pascual AbenojaNo ratings yet
- Fluids and Electrolytes Part 1Document4 pagesFluids and Electrolytes Part 1baraderoayyah41No ratings yet
- Fluid and Electrolytes NCM 109Document3 pagesFluid and Electrolytes NCM 109syroise margauxNo ratings yet
- Micronutrients: Water & ElectrolytesDocument2 pagesMicronutrients: Water & ElectrolytesRANDY ERNEST GESTOSANINo ratings yet
- Fluid & Electrolyte, Acid-Base Imbalance (MS REPORT)Document41 pagesFluid & Electrolyte, Acid-Base Imbalance (MS REPORT)Jane BelvisNo ratings yet
- AG BP Exam1Document21 pagesAG BP Exam1katelynricki14No ratings yet
- Chloride ImbalancesDocument2 pagesChloride ImbalancesBruce EstilloteNo ratings yet
- Study Guide 9 Fluids Electrolytes Acid Base Balance For StudentsDocument10 pagesStudy Guide 9 Fluids Electrolytes Acid Base Balance For StudentsliahekuriNo ratings yet
- Fluids and ElectrolylesDocument12 pagesFluids and ElectrolylesTine GuibaoNo ratings yet
- FE Imbalance HandoutsDocument2 pagesFE Imbalance HandoutsPrasanth Kurien Mathew100% (2)
- NCM 112 Fluid and ElectrolytesDocument2 pagesNCM 112 Fluid and ElectrolytesAngeline NavarroNo ratings yet
- Fluids and Electrolytes NotesDocument17 pagesFluids and Electrolytes NotesFaye G.No ratings yet
- Fluid and ElectrolyteDocument4 pagesFluid and Electrolytevaibhav nigamNo ratings yet
- Electrolyte DisordersDocument29 pagesElectrolyte Disorderssanketh bhat.sNo ratings yet
- M1 - F&eDocument2 pagesM1 - F&ejuiceNo ratings yet
- Midterms - Electrolyte Renal DisordersDocument40 pagesMidterms - Electrolyte Renal DisordersRachelle DelantarNo ratings yet
- PEDIA REPORT - Fluids and ElectrolytesDocument47 pagesPEDIA REPORT - Fluids and ElectrolytesFaydhal SalikNo ratings yet
- Hyponatremia in Children (PICU COURSE)Document83 pagesHyponatremia in Children (PICU COURSE)surasuarezlopezNo ratings yet
- DR Saroj PandaDocument45 pagesDR Saroj PandaPranshu Prajyot 67No ratings yet
- English of NursingDocument1 pageEnglish of NursingyustiNo ratings yet
- Quiz 1Document3 pagesQuiz 1Wiljohn de la CruzNo ratings yet
- Fluid and Electrolyte in InfantDocument44 pagesFluid and Electrolyte in InfantVibin K vNo ratings yet
- ELECTROLYTES EditedDocument6 pagesELECTROLYTES EditedKrystel Bea DinqueNo ratings yet
- Chapter 5-Inorganic ChemDocument5 pagesChapter 5-Inorganic ChemMark Harold GonzalesNo ratings yet
- Anaphy Lec IDocument3 pagesAnaphy Lec IKrishna LibrodoNo ratings yet
- Fluidandelectrolyte TodayDocument76 pagesFluidandelectrolyte TodayPrithvi MagarNo ratings yet
- Chapter 34 - PolyuriaDocument6 pagesChapter 34 - Polyuriajonalyn.mejellanoNo ratings yet
- The Most Commonly Ordered (Chemistry) Laboratory InvestigationsDocument94 pagesThe Most Commonly Ordered (Chemistry) Laboratory InvestigationsZEESHAN YOUSUFNo ratings yet
- MidtermsDocument40 pagesMidtermsSteph CaronanNo ratings yet
- Fluids PDFDocument26 pagesFluids PDFLeogalvez BedanoNo ratings yet
- Drug StudyDocument7 pagesDrug StudyBella Cy LopezNo ratings yet
- Prof. Sandra M. Covarrubias - September 24, 2021: 5.2fluid & Electrolytes ImbalancesDocument5 pagesProf. Sandra M. Covarrubias - September 24, 2021: 5.2fluid & Electrolytes ImbalancesIvy VillalobosNo ratings yet
- Electrolyte Imbalances ReviewerDocument14 pagesElectrolyte Imbalances ReviewerhoneyNo ratings yet
- Fluids & Elec. 3Document87 pagesFluids & Elec. 3Krystal AliñabonNo ratings yet
- Disorders-Of-Sodium-Balance - CAMBRIDGEDocument10 pagesDisorders-Of-Sodium-Balance - CAMBRIDGEDenisa Carmen ColiofNo ratings yet
- Group 4 Final Paper Bacterial OrganismDocument55 pagesGroup 4 Final Paper Bacterial OrganismRodriguez, Jhe-ann M.No ratings yet
- Doon Institute of Medical Science2 (Exam Paper)Document3 pagesDoon Institute of Medical Science2 (Exam Paper)Shaila PanchalNo ratings yet
- Escherichia Coli 1. Definition of Escherichia ColiDocument6 pagesEscherichia Coli 1. Definition of Escherichia Coliwiwi oktafianiNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Siva ShanmugamNo ratings yet
- Stress and Periodontal Disease PDFDocument7 pagesStress and Periodontal Disease PDFDaniela RusnacNo ratings yet
- 4 - Rohini Nakshatra Padas in Ravana SamhitaDocument15 pages4 - Rohini Nakshatra Padas in Ravana SamhitaMarilou1963No ratings yet
- Parainfluenza Viruses in Adults - UpToDateDocument25 pagesParainfluenza Viruses in Adults - UpToDateMisael TaverasNo ratings yet
- Balance de LiquidosDocument8 pagesBalance de LiquidosAhira Susana Mendoza de RiveraNo ratings yet
- Eating Fruits - The Correct WayDocument5 pagesEating Fruits - The Correct WayNimesh Shah100% (2)
- Genetic Disorders AVN 24 12 2020Document17 pagesGenetic Disorders AVN 24 12 2020MuskanNo ratings yet
- G6PD Deficiency Group 6Document36 pagesG6PD Deficiency Group 6Christian Darwin Llanes100% (2)
- Intra Uterine Growth RetardationDocument46 pagesIntra Uterine Growth RetardationIba Ghannam100% (1)
- Acute Gastroenteritis: Brigitte Ulrike D. Tabaranza M.DDocument65 pagesAcute Gastroenteritis: Brigitte Ulrike D. Tabaranza M.DChandice CuaNo ratings yet
- Pathophysiology Cholelithiasis 2Document2 pagesPathophysiology Cholelithiasis 2Jamie HaravataNo ratings yet
- Paper IX MCQ Set ADocument3 pagesPaper IX MCQ Set AHimanshu KarmacharyaNo ratings yet
- Willemsen 2012Document13 pagesWillemsen 2012EstebanGiraNo ratings yet
- Ismail's Undergraduate ThesisDocument82 pagesIsmail's Undergraduate ThesisAbiola IbrahimNo ratings yet
- Health and Safety Protocols: Dr. Michael Bautista Dr. Ethyl Salvador-CayetanoDocument35 pagesHealth and Safety Protocols: Dr. Michael Bautista Dr. Ethyl Salvador-CayetanoJordz PlaciNo ratings yet
- (2020) Glycyrrhiza Glabra (Licorice)Document10 pages(2020) Glycyrrhiza Glabra (Licorice)icaNo ratings yet
- Health Psychology Canadian 4th Edition Taylor Test BankDocument13 pagesHealth Psychology Canadian 4th Edition Taylor Test BankJosephWilliamsinaom100% (12)
- 100014Z09JM2016 Mathew PDFDocument7 pages100014Z09JM2016 Mathew PDFRameshKrishnanNo ratings yet
- Mnemonics Definitions PDFDocument6 pagesMnemonics Definitions PDFsaquib eqbalNo ratings yet
- Ir Choice Board 1Document1 pageIr Choice Board 1api-621945476No ratings yet
- Microbiology First Exam - Past Year QDocument7 pagesMicrobiology First Exam - Past Year QNabilah Mohd YaakobNo ratings yet
- Physical EducationDocument3 pagesPhysical EducationusunomNo ratings yet
- Medical Ethics 2023 FINALDocument56 pagesMedical Ethics 2023 FINALBelinda ELISHANo ratings yet
- COVID 19 - Clinical Picture in The Elderly Population: A Qualitative Systematic ReviewDocument21 pagesCOVID 19 - Clinical Picture in The Elderly Population: A Qualitative Systematic ReviewRila RivandaNo ratings yet
- 203 Health DefinitionDocument20 pages203 Health DefinitionJodi BrutonNo ratings yet
- Psychoactive Drugs and Transactional Analysis PDFDocument7 pagesPsychoactive Drugs and Transactional Analysis PDFAlex LenkemzNo ratings yet