Download as pdf or txt
You might also like
- Expectant Mother'S and Baby Information Sheet: Given Name: Middle Name: Last NameDocument3 pagesExpectant Mother'S and Baby Information Sheet: Given Name: Middle Name: Last NameLeslie D. Aton87% (15)
- Practical Research 1: Quarter 3 - Module 2: Characteristics, Processes and Ethics of ResearchDocument32 pagesPractical Research 1: Quarter 3 - Module 2: Characteristics, Processes and Ethics of ResearchVINCENT BIALEN80% (30)
- Sleep Duration and The Academic Performance of 12th Grade Senior High School Students, Academic Year 2019 - 2020Document14 pagesSleep Duration and The Academic Performance of 12th Grade Senior High School Students, Academic Year 2019 - 2020Daniel Malhabour100% (5)
- Vaishak - AmulDocument22 pagesVaishak - AmulVaishak Nair75% (4)
- Arabic Grammar - Level 01 - English AnswersDocument47 pagesArabic Grammar - Level 01 - English AnswersJawedsIslamicLibrary100% (3)
- 10 Ways To Create Shareholder ValueDocument3 pages10 Ways To Create Shareholder ValuetahirNo ratings yet
- 4 Sleep Reis 2021Document8 pages4 Sleep Reis 2021Bruna Filliettaz RiosNo ratings yet
- Jurnal 8 CDocument5 pagesJurnal 8 CCintya RambuNo ratings yet
- CCH 12376Document15 pagesCCH 12376alifia shafa s psiNo ratings yet
- Sleep Quality Among Primary Care Attendees in Kaduna, Northern Nigeria A Case-Control Study-Nuhu Et Al IJPMDocument11 pagesSleep Quality Among Primary Care Attendees in Kaduna, Northern Nigeria A Case-Control Study-Nuhu Et Al IJPMAdeyemi OlusolaNo ratings yet
- Sleep Health: Pilot Study of A Sleep Health Promotion Program For College StudentsDocument8 pagesSleep Health: Pilot Study of A Sleep Health Promotion Program For College StudentsLushy Ayu DistaNo ratings yet
- Psychiatry Research: Lan Wang, Peng Qin, Yunshan Zhao, Shengyun Duan, Qing Zhang, Ying Liu, Yueling Hu, Juan SunDocument6 pagesPsychiatry Research: Lan Wang, Peng Qin, Yunshan Zhao, Shengyun Duan, Qing Zhang, Ying Liu, Yueling Hu, Juan SunBrayan CorreaNo ratings yet
- Sleep Predictors and Sleep Patterns - CarskadonDocument29 pagesSleep Predictors and Sleep Patterns - CarskadonScarlettBlondeNo ratings yet
- 3 PBDocument9 pages3 PBaddityarosyyi tama2 (Webinar data analisis)No ratings yet
- 2 - Quality of SleepDocument13 pages2 - Quality of SleepDr Mryhan AdelNo ratings yet
- 6.anitha. P Jayestri Kurushev A. Jalajarani A. Felicia ChitraDocument14 pages6.anitha. P Jayestri Kurushev A. Jalajarani A. Felicia ChitraRiya RishabNo ratings yet
- Child Sleep HabitsDocument9 pagesChild Sleep HabitsAravind Babu100% (1)
- Fpsyt 10 00284Document9 pagesFpsyt 10 00284Cella BamilexNo ratings yet
- FinalDocument8 pagesFinalthejas omkarNo ratings yet
- Suardiaz-Muro Et Al. - 2023 - Sleep Quality and Sleep Deprivation RelationshipDocument7 pagesSuardiaz-Muro Et Al. - 2023 - Sleep Quality and Sleep Deprivation RelationshipMARIBEL YAQUI YAURI MENDOZANo ratings yet
- Associations of Physical Activity, Screen Time With Depression, Anxiety and Sleep Quality Among Chinese College FreshmenDocument5 pagesAssociations of Physical Activity, Screen Time With Depression, Anxiety and Sleep Quality Among Chinese College FreshmenReynaldy Anggara SaputraNo ratings yet
- Chekwa ChekwaDocument7 pagesChekwa ChekwaRain Luis CagulaNo ratings yet
- Sleep Quality and The Factors Affecting The Fatigue Severity and Academic Performance of Students at AJA University of Medical SciencesDocument7 pagesSleep Quality and The Factors Affecting The Fatigue Severity and Academic Performance of Students at AJA University of Medical SciencesRima SitiNo ratings yet
- Sleep Disturbances Among Medical Students: A Global PerspectiveDocument6 pagesSleep Disturbances Among Medical Students: A Global PerspectiveShinichi Conan HaibaraNo ratings yet
- About SleepDocument71 pagesAbout SleepAnnisa Kurnia HastutiNo ratings yet
- CC 12736Document8 pagesCC 12736Neneng HumairohNo ratings yet
- JCSM 14 11 1849Document9 pagesJCSM 14 11 1849Angel NikiyuluwNo ratings yet
- Influence of Sleep in Academic Performance - An Integrated Review of LiteratureDocument4 pagesInfluence of Sleep in Academic Performance - An Integrated Review of LiteratureIOSRjournalNo ratings yet
- Ajol File Journals - 414 - Articles - 227458 - Submission - Proof - 227458 4933 553839 1 10 20220630Document5 pagesAjol File Journals - 414 - Articles - 227458 - Submission - Proof - 227458 4933 553839 1 10 20220630daaktarsaabNo ratings yet
- Sleep Quality Among University Students Associations Between Demographic Factors and Physical ActiDocument9 pagesSleep Quality Among University Students Associations Between Demographic Factors and Physical ActiBrent KinawutNo ratings yet
- Research ReferenceDocument20 pagesResearch Referencelexschub12No ratings yet
- Do Medical Students in Hong Kong Have Enough Sleep?: Comments and OpinionsDocument5 pagesDo Medical Students in Hong Kong Have Enough Sleep?: Comments and OpinionsTony AndersonNo ratings yet
- 10.1016 J.jadohealth.2009.06.016Document9 pages10.1016 J.jadohealth.2009.06.016WahyuNo ratings yet
- Jurnal Pendukung - Investigation The Relation Between Sleep and Quality of Life For College Student in TaiwanDocument11 pagesJurnal Pendukung - Investigation The Relation Between Sleep and Quality of Life For College Student in TaiwanKHEZIA ANGGELANo ratings yet
- Diccionario Laplanche PontalisDocument1 pageDiccionario Laplanche PontalisPedro Carlos MartinezNo ratings yet
- Sleep Disturbances Among MedstudDocument12 pagesSleep Disturbances Among MedstudPutri NareswariNo ratings yet
- Evaluation of Sleep Quality in Medical Students During The Covid-19 PandemicDocument4 pagesEvaluation of Sleep Quality in Medical Students During The Covid-19 PandemicIJAR JOURNALNo ratings yet
- Prevalence of Insomnia JACH 29042010 FinalizedDocument16 pagesPrevalence of Insomnia JACH 29042010 FinalizedAmii BușecanNo ratings yet
- Socio-Demographic Issues and Health-Related Quality of Life Among Inmates of A Correctional Center in Southwest NigeriaDocument5 pagesSocio-Demographic Issues and Health-Related Quality of Life Among Inmates of A Correctional Center in Southwest NigeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Questionnaire-Derived Sleep Habits and Academic Achievement in First Year University StudentsDocument7 pagesQuestionnaire-Derived Sleep Habits and Academic Achievement in First Year University Studentsrocelle marbellaNo ratings yet
- Prevalence and Correlates of Poor Sleep Quality Among Medical Students at A Nigerian UniversityDocument7 pagesPrevalence and Correlates of Poor Sleep Quality Among Medical Students at A Nigerian UniversityCandra FaridNo ratings yet
- J Am Board Fam MedDocument15 pagesJ Am Board Fam MedLucía VallzNo ratings yet
- Translate Yasleep HygieneDocument8 pagesTranslate Yasleep HygieneFitria Indah LestariNo ratings yet
- Sleep Disorder 2Document5 pagesSleep Disorder 2Dani ursNo ratings yet
- Changes in Sleep Habits of Medical Students According To Class Starting Time: A Longitudinal StudyDocument2 pagesChanges in Sleep Habits of Medical Students According To Class Starting Time: A Longitudinal StudyCarrie Anne GarciaNo ratings yet
- 35-Article Text-123-1-10-20210127Document9 pages35-Article Text-123-1-10-20210127Hariharan HemarajanNo ratings yet
- 1024-Article Text-2121-1-10-20230207Document7 pages1024-Article Text-2121-1-10-20230207Charity TololiuNo ratings yet
- Assessing Sleep Qualityof SHSStudentsDocument10 pagesAssessing Sleep Qualityof SHSStudentskberrameNo ratings yet
- 1877 7544 2 PB PDFDocument4 pages1877 7544 2 PB PDFSabaNo ratings yet
- Impact of Poor Sleep Quality On The Academic Performance of Medical StudentsDocument6 pagesImpact of Poor Sleep Quality On The Academic Performance of Medical StudentsAngela Cuevas DimaanoNo ratings yet
- A Cross Sectional Survey On Sleep Quality, Mental Health, and Academic Performance Among Medical Student in Saudia ArabiaDocument5 pagesA Cross Sectional Survey On Sleep Quality, Mental Health, and Academic Performance Among Medical Student in Saudia ArabiaReynaldy Anggara SaputraNo ratings yet
- Association Between Subjective Sleep Quality, Hypertension, Depression and Body Mass Index in A Nigerian Family Practice SettingDocument7 pagesAssociation Between Subjective Sleep Quality, Hypertension, Depression and Body Mass Index in A Nigerian Family Practice SettingFerdy LainsamputtyNo ratings yet
- CSHQDocument11 pagesCSHQRiffq Rambu AnarkiNo ratings yet
- Prevalence of Sleep Quality Among Academic Staff of A Private University in MalaysiaDocument7 pagesPrevalence of Sleep Quality Among Academic Staff of A Private University in MalaysiaSitNo ratings yet
- Assessment of Sleep Quality and Related Factors in Stroke PatientsDocument8 pagesAssessment of Sleep Quality and Related Factors in Stroke PatientsajmrdNo ratings yet
- PsqiDocument7 pagesPsqiIntanwatiNo ratings yet
- Factors Associated With Sleep Quality Among Undergraduate Students at A Malaysian Public UniversityDocument19 pagesFactors Associated With Sleep Quality Among Undergraduate Students at A Malaysian Public UniversityHayati RaisNo ratings yet
- The Correlation Between Sleep Quality and Levels of Stress Among Students in Universitas IndonesiaDocument5 pagesThe Correlation Between Sleep Quality and Levels of Stress Among Students in Universitas IndonesiaKripa SriramNo ratings yet
- The Relationship Between Sleep Habits and Academic Performance in Dental Students in CroatiaDocument8 pagesThe Relationship Between Sleep Habits and Academic Performance in Dental Students in CroatiaBeatrizCamposNo ratings yet
- Sleepiness, Sleep Deprivation, Quality of Life, Mental Symptoms and Perception of Academic Environment in Medical StudentsDocument14 pagesSleepiness, Sleep Deprivation, Quality of Life, Mental Symptoms and Perception of Academic Environment in Medical StudentsAljho AljhoNo ratings yet
- Assessing Sleep Quality of Shs StudentsDocument10 pagesAssessing Sleep Quality of Shs StudentsDian HernandezNo ratings yet
- Association of Physical Activity, SedentaryDocument10 pagesAssociation of Physical Activity, SedentaryIsabella Camacho BarragánNo ratings yet
- Whoqol BrefDocument7 pagesWhoqol BrefreetikaNo ratings yet
- Final (Local)Document3 pagesFinal (Local)dl masanquexNo ratings yet
- Neurological Assessment in the First Two Years of LifeFrom EverandNeurological Assessment in the First Two Years of LifeGiovanni CioniNo ratings yet
- Steimour Rate of Sedimentation Suspensions of Uniform-Size Angular Particles PDFDocument8 pagesSteimour Rate of Sedimentation Suspensions of Uniform-Size Angular Particles PDFpixulinoNo ratings yet
- Review: Steps Big Book: Step 4Document28 pagesReview: Steps Big Book: Step 4Jaime LaroseNo ratings yet
- GREY BOOK August 2017 66thDocument146 pagesGREY BOOK August 2017 66thxedoyis969No ratings yet
- Fashion Retail Merchandising Retail Visit ReportDocument6 pagesFashion Retail Merchandising Retail Visit Reportchins1289No ratings yet
- Cwts - Module - 1st Semester A.Y 2022-2023Document71 pagesCwts - Module - 1st Semester A.Y 2022-2023Jae Ashlie BernabeNo ratings yet
- Compliance Factors Associated With Contact Lens-Related Dry EyeDocument6 pagesCompliance Factors Associated With Contact Lens-Related Dry EyeAlda Gitu RahmaNo ratings yet
- Response Sheet For SCQDocument7 pagesResponse Sheet For SCQChandresh Gambhir100% (1)
- 1E Star Trek Customizable Card Game - 4 Introductory Two-Player Rule BookDocument9 pages1E Star Trek Customizable Card Game - 4 Introductory Two-Player Rule Bookmrtibbles100% (1)
- NITIE PGDEx VLFM Brochure 2021 22Document36 pagesNITIE PGDEx VLFM Brochure 2021 22PiyushNo ratings yet
- La Credibilidad de Las Noticias en InternetDocument19 pagesLa Credibilidad de Las Noticias en InternetDavid Ricardo García CantorNo ratings yet
- How To Use Friends As A Reference (Plus How To Ask Them)Document6 pagesHow To Use Friends As A Reference (Plus How To Ask Them)josieliraychanNo ratings yet
- Feedback Mechanism InstrumentDocument2 pagesFeedback Mechanism InstrumentKing RickNo ratings yet
- The DasharupakasDocument8 pagesThe DasharupakasvedasriradhaNo ratings yet
- Common Abbreviations Abbreviation Meaning: 4.24.18.CAS - AGDocument2 pagesCommon Abbreviations Abbreviation Meaning: 4.24.18.CAS - AGLu GonzoNo ratings yet
- Revision of An Upper Lip Scar Following - 2022 - Advances in Oral and MaxillofacDocument2 pagesRevision of An Upper Lip Scar Following - 2022 - Advances in Oral and MaxillofacГне ДзжNo ratings yet
- Report MAN AS EMBODIED SUBJECTIVITYDocument7 pagesReport MAN AS EMBODIED SUBJECTIVITYCute TzyNo ratings yet
- Maoism in Bangla PDFDocument15 pagesMaoism in Bangla PDFAyub Khan JrNo ratings yet
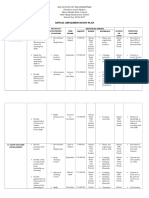
- Annual Implementation PlanDocument4 pagesAnnual Implementation PlanNeil Atanacio50% (2)
- What Is MentoringDocument5 pagesWhat Is MentoringDeepak Kumar SinghNo ratings yet
- AIIMS PG Solved Paper 1999Document3 pagesAIIMS PG Solved Paper 1999Beta ReaderNo ratings yet
- Ecology of PA ReportDocument19 pagesEcology of PA ReportJulius Lacaba AstudilloNo ratings yet
- Mahasneh 2010 Emotiveness in Darwish PDFDocument140 pagesMahasneh 2010 Emotiveness in Darwish PDFAlaa SabbahNo ratings yet
- Sentence TransformationDocument31 pagesSentence Transformationsdbw5rgxfgNo ratings yet
- Connectors RephrasingDocument2 pagesConnectors RephrasingsoniaNo ratings yet
- Solomon Concert ReviewDocument4 pagesSolomon Concert ReviewBrianWeathersNo ratings yet