Download as docx, pdf, or txt
You might also like
- SPREad PlateDocument7 pagesSPREad PlateJermeLou BaoNo ratings yet
- Management of Chronic Hepatitis B - An Overview of Practice Guidelines For Primary Care ProvidersDocument16 pagesManagement of Chronic Hepatitis B - An Overview of Practice Guidelines For Primary Care Providersdanny17phNo ratings yet
- Keeffe 2008Document27 pagesKeeffe 2008Maymay DamayNo ratings yet
- EASL HepBDocument42 pagesEASL HepBmutiara dewiNo ratings yet
- AASLD Guidelines For Treatment of Chronic Hepatitis BDocument23 pagesAASLD Guidelines For Treatment of Chronic Hepatitis BNuGroHooNo ratings yet
- Tratamiento de HVB y VihDocument4 pagesTratamiento de HVB y VihCarlos Elio Polo VargasNo ratings yet
- Keeffe 2006Document27 pagesKeeffe 2006Maymay DamayNo ratings yet
- Zoulim 2014Document18 pagesZoulim 2014Indah LestariNo ratings yet
- 04 02 12 - CHB in Pregnancy - The Female PatientDocument5 pages04 02 12 - CHB in Pregnancy - The Female PatientElli Dwi ErmawatiNo ratings yet
- Awareness On HepatitisDocument52 pagesAwareness On HepatitisMizanur RahmanNo ratings yet
- 2006HCV SingleDocument22 pages2006HCV Singleharishiyer1504No ratings yet
- WJG. Hepatitis BDocument18 pagesWJG. Hepatitis BMuhammad Nur Ardhi LahabuNo ratings yet
- Monitoring The Patient With HIV and Chronic Hepatitis B Virus InfectionDocument9 pagesMonitoring The Patient With HIV and Chronic Hepatitis B Virus Infectionmayteveronica1000No ratings yet
- Art HBV 1Document14 pagesArt HBV 1Daniel Manay GuadalupeNo ratings yet
- Sinn 2019Document13 pagesSinn 2019Shiza FathimakbNo ratings yet
- AASLDUpdate Treatment Genotype 1 HCV11113Document14 pagesAASLDUpdate Treatment Genotype 1 HCV11113Mew KanokwanNo ratings yet
- Number 1 MARCH 2006Document178 pagesNumber 1 MARCH 2006wawanpecelNo ratings yet
- British Hiv-Tb GuidelinesDocument34 pagesBritish Hiv-Tb GuidelinesPuspita SariNo ratings yet
- HCV Treatment RevolutionDocument3 pagesHCV Treatment RevolutionMai NabiehNo ratings yet
- AIDS TreatmentDocument85 pagesAIDS TreatmentZoranNo ratings yet
- Literature Review of HBVDocument6 pagesLiterature Review of HBVafmabbpoksbfdp100% (1)
- Literature Review of Hepatitis B Virus InfectionDocument4 pagesLiterature Review of Hepatitis B Virus Infectionbsdavcvkg100% (1)
- Aasld Practice Guidelines Chronic Hepatitis B: Update 2009Document36 pagesAasld Practice Guidelines Chronic Hepatitis B: Update 2009lirucrocodilulNo ratings yet
- UntitledDocument43 pagesUntitledJovania B.No ratings yet
- Hepatology - 2018 - Terrault - Update On Prevention Diagnosis and Treatment of Chronic Hepatitis B AASLD 2018 HepatitisDocument40 pagesHepatology - 2018 - Terrault - Update On Prevention Diagnosis and Treatment of Chronic Hepatitis B AASLD 2018 HepatitisratuNo ratings yet
- Canadian Thoracic Society Clinical Practice Guideline On Pharmacotherapy in Patients With COPD 2019 Update of EvidenceDocument24 pagesCanadian Thoracic Society Clinical Practice Guideline On Pharmacotherapy in Patients With COPD 2019 Update of EvidenceDavid Gonzalo Ramirez EstelaNo ratings yet
- Pretreatment Evaluation of Chronic Hepatitis B Virus Infection in The Patient With HIVDocument8 pagesPretreatment Evaluation of Chronic Hepatitis B Virus Infection in The Patient With HIVmayteveronica1000No ratings yet
- HepC Treatment 2015Document38 pagesHepC Treatment 2015Claudia IrinaNo ratings yet
- HIV Resistance AssaysDocument9 pagesHIV Resistance AssayssonykoNo ratings yet
- Treatment Algorithm For Managing Chronic Hepatitis B VirusDocument10 pagesTreatment Algorithm For Managing Chronic Hepatitis B VirusRadhaRajasekaranNo ratings yet
- Chronic Hepatitis B - New Goals, New Treatment: Ching-Lung Lai, M.D., and Man-Fung Yuen, M.DDocument4 pagesChronic Hepatitis B - New Goals, New Treatment: Ching-Lung Lai, M.D., and Man-Fung Yuen, M.DSofara RezantiNo ratings yet
- Guidelines On Hepatitis B and C Testing: November 2016Document16 pagesGuidelines On Hepatitis B and C Testing: November 2016Hichem MansouriNo ratings yet
- KEDOKTERANDocument19 pagesKEDOKTERANAndi RahmaNo ratings yet
- Idsa Tratamiento TBC EspañolDocument8 pagesIdsa Tratamiento TBC EspañolJosé D. Lira BouttóNo ratings yet
- Chronic Hepatitis B Infection in ChildrenDocument4 pagesChronic Hepatitis B Infection in ChildrenSara KhanNo ratings yet
- Literature Review of Hepatitis B VirusDocument4 pagesLiterature Review of Hepatitis B Virusbaduidcnd100% (1)
- Template Letter For Insurance Mandating 8 Weeks Vs 12 Weeks of HarvoniDocument1 pageTemplate Letter For Insurance Mandating 8 Weeks Vs 12 Weeks of HarvoniRobert G. Gish, MDNo ratings yet
- Tugas KMB 3 Mayanih 08200100112Document14 pagesTugas KMB 3 Mayanih 08200100112indri pijuNo ratings yet
- Management of Chronic Hepatitis C Virus Infection - Initial Antiviral Therapy in Adults - UpToDateDocument22 pagesManagement of Chronic Hepatitis C Virus Infection - Initial Antiviral Therapy in Adults - UpToDateGabrielle AndersonNo ratings yet
- Tacke2016 - Treatment For Hepatitis B in Patients With Drug ResistanceDocument7 pagesTacke2016 - Treatment For Hepatitis B in Patients With Drug ResistanceClarisa AnindyaNo ratings yet
- HCV 1Document2 pagesHCV 1Mostafa ElashryNo ratings yet
- Simple, Effective, But Out of Reach? Public Health Implications of HCV DrugsDocument3 pagesSimple, Effective, But Out of Reach? Public Health Implications of HCV DrugsDirga Rasyidin LNo ratings yet
- Tb-Hiv Card 2012Document2 pagesTb-Hiv Card 2012soulanalyticaNo ratings yet
- 1 s2.0 S0168827818319688 Main PDFDocument51 pages1 s2.0 S0168827818319688 Main PDFChadi MamloukNo ratings yet
- Antiviral Therapy For Chronic Hepatitis B in China: Xin Zheng Junzhong Wang Dongliang YangDocument6 pagesAntiviral Therapy For Chronic Hepatitis B in China: Xin Zheng Junzhong Wang Dongliang Yangapi-206282033No ratings yet
- Structure of The Guidelines Along The Continuum of Care: 1.1. Goals and ObjectivesDocument11 pagesStructure of The Guidelines Along The Continuum of Care: 1.1. Goals and ObjectivesSarahNo ratings yet
- MT 6322 - Mycology and Virology 2nd Shifting OLADocument9 pagesMT 6322 - Mycology and Virology 2nd Shifting OLAlily bluesNo ratings yet
- Hepatitis B Virus and Hepatitis C Virus Co-Infection With HIVDocument54 pagesHepatitis B Virus and Hepatitis C Virus Co-Infection With HIVShree Narayan YadavNo ratings yet
- Adult and Adolescent GLDocument240 pagesAdult and Adolescent GLFadilLoveMamaNo ratings yet
- Cmmi2021 2135924Document7 pagesCmmi2021 2135924ken3365448No ratings yet
- Mediterranean Journal of Hematology and Infectious DiseasesDocument7 pagesMediterranean Journal of Hematology and Infectious Diseasesbryan ruditaNo ratings yet
- C. 48-Year-Old Man Who Has Sex With Men: AlasanDocument12 pagesC. 48-Year-Old Man Who Has Sex With Men: AlasanAjeng WidyastutiNo ratings yet
- Chronic Hepatitis B 1Document1 pageChronic Hepatitis B 1Drsajith Sebastian JosephNo ratings yet
- Lesson 9 Article 2Document11 pagesLesson 9 Article 2JafinNo ratings yet
- Hepb y RTX PDFDocument3 pagesHepb y RTX PDFYeli VeMeNo ratings yet
- Table 44-8 Nursing Assessment: Hepatitis Subjective Data Important Health InformationDocument7 pagesTable 44-8 Nursing Assessment: Hepatitis Subjective Data Important Health InformationAnggela kian puspaNo ratings yet
- AGA Clinical Practice Update On Management of Inflammatory Bowel Disease in Elderly Patients Expert ReviewDocument22 pagesAGA Clinical Practice Update On Management of Inflammatory Bowel Disease in Elderly Patients Expert Reviewinfinity TangNo ratings yet
- Treatment of Pulmonary and Extra-Pulmonary Tuberculosis in AdultsDocument65 pagesTreatment of Pulmonary and Extra-Pulmonary Tuberculosis in AdultsLloyd Daniel BarrantesNo ratings yet
- User's Guide to Natural Therapies for Cancer Prevention and ControlFrom EverandUser's Guide to Natural Therapies for Cancer Prevention and ControlRating: 5 out of 5 stars5/5 (1)
- Targeted Therapy in Translational Cancer ResearchFrom EverandTargeted Therapy in Translational Cancer ResearchApostolia-Maria TsimberidouNo ratings yet
- Optimizing Advanced Therapies in Ulcerative Colitis: Is Your Practice Up to Date? A Focus on Clinical Evidence and Guideline RecommendationsFrom EverandOptimizing Advanced Therapies in Ulcerative Colitis: Is Your Practice Up to Date? A Focus on Clinical Evidence and Guideline RecommendationsNo ratings yet
- Types of CatheterDocument1 pageTypes of CatheterShine KhayNo ratings yet
- ILEOSTOMYDocument11 pagesILEOSTOMYShine Khay100% (1)
- Abdominal UltrasoundDocument11 pagesAbdominal UltrasoundShine Khay100% (2)
- Cardio Skills LabDocument4 pagesCardio Skills LabShine KhayNo ratings yet
- Shingles PosterDocument1 pageShingles Posterapi-266804300100% (1)
- Activity Sheet Aseptic Technique Plate StreakingDocument2 pagesActivity Sheet Aseptic Technique Plate StreakingWAL- Michael Andrei AngeloNo ratings yet
- D.S.S Aiims Prepration Test Series DR - SANJAY 7014964651Document7 pagesD.S.S Aiims Prepration Test Series DR - SANJAY 7014964651Dr-Sanjay SinghaniaNo ratings yet
- Immunization AssignmentDocument4 pagesImmunization Assignmentgadoura95No ratings yet
- 2 5348228160427133754Document18 pages2 5348228160427133754Muhammad HasanNo ratings yet
- CIC Study Plan and Workbook 2018 (DOH-Orange)Document52 pagesCIC Study Plan and Workbook 2018 (DOH-Orange)Shameen KhanNo ratings yet
- Molecular Diagnostics: Report Status - Final Test Name Result Biological Ref. Interval UnitDocument3 pagesMolecular Diagnostics: Report Status - Final Test Name Result Biological Ref. Interval UnitRumble RiderNo ratings yet
- Control of Hospital Acquired Infection PDFDocument36 pagesControl of Hospital Acquired Infection PDFPrakashNo ratings yet
- Outbreak Investigation Case Scenarios-PHASE III-SDL, 15-17.05.2023-1Document13 pagesOutbreak Investigation Case Scenarios-PHASE III-SDL, 15-17.05.2023-1srinidhi premkumarNo ratings yet
- Arief EffendiDocument43 pagesArief EffendiHarsya KhairudinNo ratings yet
- Coronavirus Covid 19 Presentation Free Template by Slidecore 87pusdDocument24 pagesCoronavirus Covid 19 Presentation Free Template by Slidecore 87pusdHASSANNo ratings yet
- Shigella - Режим Совместимости - ВосстановленDocument25 pagesShigella - Режим Совместимости - Восстановленabbassi mohammedNo ratings yet
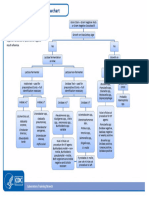
- Aerobic Gram Negative Rods FlowchartDocument1 pageAerobic Gram Negative Rods FlowchartKeithNo ratings yet
- Assessment of Bacterial Contamination in Cellular PhonesDocument8 pagesAssessment of Bacterial Contamination in Cellular PhonesMedrechEditorialNo ratings yet
- Safety Aspects of Probiotic ProductsDocument4 pagesSafety Aspects of Probiotic ProductsSrinivas PingaliNo ratings yet
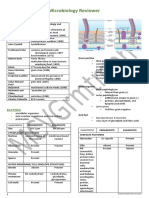
- Microbiology Reviewer: HistoryDocument29 pagesMicrobiology Reviewer: HistoryJOHN ROCKFORD LAZARONo ratings yet
- Parasitology ReviewerDocument15 pagesParasitology ReviewerMariel Angelie TuringanNo ratings yet
- IN893000 v6.0 Clearview PBP2a SA Culture Colony ProducDocument101 pagesIN893000 v6.0 Clearview PBP2a SA Culture Colony ProducRazaz AdilNo ratings yet
- Identification of Enterococcus Faecium and Enterococcus Faecalid As Vanc TypeDocument11 pagesIdentification of Enterococcus Faecium and Enterococcus Faecalid As Vanc TypeoinkNo ratings yet
- Life Cycle of The Malaria ParasiteDocument4 pagesLife Cycle of The Malaria ParasiteDyah Ayu KusumawarddhaniNo ratings yet
- REOVIRUSESDocument28 pagesREOVIRUSESFrancis MakanyaNo ratings yet
- Usp 2022 Microbiological Procedures For Absence of SpecifiedDocument7 pagesUsp 2022 Microbiological Procedures For Absence of SpecifiedChetalee NaikNo ratings yet
- Immunization and Population - Fertility Statistics - III-II Practical ScheduleDocument1 pageImmunization and Population - Fertility Statistics - III-II Practical ScheduleBlanket PotatoNo ratings yet
- Botany B.SCDocument2 pagesBotany B.SCAkash Deep PandeyNo ratings yet
- Veterinary MicrobiologyDocument206 pagesVeterinary MicrobiologyHomosapienNo ratings yet
- Differential StainingDocument8 pagesDifferential Stainingabdullah albayatiNo ratings yet
- Chemo ProphylaxisDocument13 pagesChemo ProphylaxisSaket DaokarNo ratings yet
- Novilyn C. Pataray BSN - Ii Pharyngitis: St. Paul College of Ilocos SurDocument1 pageNovilyn C. Pataray BSN - Ii Pharyngitis: St. Paul College of Ilocos SurCharina AubreyNo ratings yet
- M5 Lesson 2 Check-In Activity On BacilliDocument1 pageM5 Lesson 2 Check-In Activity On BacilliANGELO LOUISE CATALIGNo ratings yet