Download as pdf or txt
You might also like
- Neurocognitive Impairment Addressing Couple and Family ChallengesDocument20 pagesNeurocognitive Impairment Addressing Couple and Family ChallengesFrancisca Cid BelmarNo ratings yet
- Neurology Multiple Choice Questions With Explanations: Volume IFrom EverandNeurology Multiple Choice Questions With Explanations: Volume IRating: 4 out of 5 stars4/5 (7)
- 3rdQ Health DLLDocument4 pages3rdQ Health DLLMichelle Handumon Alviar85% (13)
- STG and Nemlt 2021Document618 pagesSTG and Nemlt 2021Emmanuel Ngimba100% (2)
- Major Neurological Syndromes PDFDocument260 pagesMajor Neurological Syndromes PDFVirlan Vasile Catalin100% (1)
- Atrial FibrillationDocument24 pagesAtrial FibrillationFani Butt50% (2)
- Paraplegia Types Causes and DiagnosisDocument15 pagesParaplegia Types Causes and Diagnosismudzung100% (1)
- Lumbar Spinal StenosisDocument4 pagesLumbar Spinal StenosiswangNo ratings yet
- 19 Spinal CordDocument8 pages19 Spinal Cordkarar AhmedNo ratings yet
- 7 - Spinal-InjuriesDocument40 pages7 - Spinal-Injuriesraed faisalNo ratings yet
- Publication CESDocument6 pagesPublication CESmedeorhoNo ratings yet
- Cauda Equina Syndrome: Innovait October 2011Document6 pagesCauda Equina Syndrome: Innovait October 2011shrt gtNo ratings yet
- Cervical RadiculopathyDocument40 pagesCervical RadiculopathyarunupadhayaNo ratings yet
- Cauda Equina Syndrome: Innovait October 2011Document6 pagesCauda Equina Syndrome: Innovait October 2011Ikhsan FebriansyahNo ratings yet
- RADIOLOGI - NEURORADIOLOGI 2 - Dr. Farah - Kelas ADocument106 pagesRADIOLOGI - NEURORADIOLOGI 2 - Dr. Farah - Kelas ASeno TanubrataNo ratings yet
- Low Back Pain: Dr. Suherman, SP.SDocument27 pagesLow Back Pain: Dr. Suherman, SP.SArmiya MiaowNo ratings yet
- Spinal Cord Disease by GadisaDocument128 pagesSpinal Cord Disease by GadisaGadisa DejeneNo ratings yet
- Spinal Cord InjuriesDocument35 pagesSpinal Cord InjuriesTitanium TssNo ratings yet
- Pott DiseaseDocument36 pagesPott DiseaseGiovanna Algu100% (1)
- BMS2-K7 Spinal Cord DiseaseDocument28 pagesBMS2-K7 Spinal Cord DiseaseFred RickNo ratings yet
- Seizure Disorder, Spinal Injury Neural TumorDocument52 pagesSeizure Disorder, Spinal Injury Neural TumornipoNo ratings yet
- ATROFIA MUSCULAR ESPINAL Lancet 2008Document14 pagesATROFIA MUSCULAR ESPINAL Lancet 2008Sebastián Silva SotoNo ratings yet
- ParaplegiaDocument7 pagesParaplegiaRigaga GopiNo ratings yet
- Lesion Del Tracto Cortico - Espinal InglesDocument14 pagesLesion Del Tracto Cortico - Espinal InglesCarolina Andrea Daza CharrisNo ratings yet
- Pott's DiseaseDocument19 pagesPott's DiseaseShashi KantNo ratings yet
- 10 1016@j Amjmed 2018 03 009Document17 pages10 1016@j Amjmed 2018 03 009pedoNo ratings yet
- Leg Weakness in A 66-Year-Old Woman: A Common Presentation of An Uncommon DiseaseDocument10 pagesLeg Weakness in A 66-Year-Old Woman: A Common Presentation of An Uncommon DiseaseCarlos De Santiago CastilloNo ratings yet
- CNS PBL 2Document6 pagesCNS PBL 2Hugh JacobsNo ratings yet
- Disc Herniation - PhysiopediaDocument1 pageDisc Herniation - Physiopedia6gydhn8ydhNo ratings yet
- Staphyllococcus Aureus and Escherichia Coli (Chronic Osteomyelitis)Document4 pagesStaphyllococcus Aureus and Escherichia Coli (Chronic Osteomyelitis)wasak123No ratings yet
- TB Spine OrthopedicsDocument34 pagesTB Spine OrthopedicsHafizah HoshniNo ratings yet
- Acute Spinal Cord Injuries - PDFDocument9 pagesAcute Spinal Cord Injuries - PDFEmanuel31No ratings yet
- Diseases of The Spinal Cord: Dr. Khairul P Surbakti, SpsDocument35 pagesDiseases of The Spinal Cord: Dr. Khairul P Surbakti, SpsAnnisa SasaNo ratings yet
- Pott Disease 122329asdas2121651385 8Document54 pagesPott Disease 122329asdas2121651385 8Dexter Flores100% (1)
- Low Back Pain: Dr. Andi Dhedie P. Sam, M.Kes, SP - OTDocument41 pagesLow Back Pain: Dr. Andi Dhedie P. Sam, M.Kes, SP - OTNia Anggreni100% (1)
- Spinal Cord Injury and CompressionDocument10 pagesSpinal Cord Injury and CompressionAdeputhNo ratings yet
- Cervical Spondylosis Treatment OptionsDocument110 pagesCervical Spondylosis Treatment OptionsA.R.AthreyaNo ratings yet
- Neuromuscular Handout 2006Document12 pagesNeuromuscular Handout 2006Windy MentariiNo ratings yet
- Spinal CordDocument15 pagesSpinal Cordsimi y100% (1)
- Low Back Pain Low Back Pain: Aldsr B Aldy S. RambeDocument40 pagesLow Back Pain Low Back Pain: Aldsr B Aldy S. RambeSantri Sasmita DewiNo ratings yet
- Seminar: Mitchell R Lunn, Ching H WangDocument14 pagesSeminar: Mitchell R Lunn, Ching H WangCatalina AlzogarayNo ratings yet
- JurnalDocument5 pagesJurnalQorin Diin ArifniNo ratings yet
- Compilation Spinal SsmsDocument35 pagesCompilation Spinal SsmsPiaRomildaTagaoCayetano100% (1)
- Neurologic Emergencies 2 MergedDocument71 pagesNeurologic Emergencies 2 MergedDanica FrancoNo ratings yet
- Low Back Pain: Aldy S. RambeDocument40 pagesLow Back Pain: Aldy S. RambeHatta Diana TariganNo ratings yet
- Emg Notes: Sunday, April 22, 2007Document11 pagesEmg Notes: Sunday, April 22, 2007Shauki AliNo ratings yet
- Clinical Approach andDocument21 pagesClinical Approach andtavooppNo ratings yet
- Neck PainDocument39 pagesNeck Paink.adeputriNo ratings yet
- Birth Injury: Prof. DR - Abbas Alrabaty College of Medicine /HMU Pediatric DepartmentDocument31 pagesBirth Injury: Prof. DR - Abbas Alrabaty College of Medicine /HMU Pediatric DepartmentChro MANo ratings yet
- Javt 14 I 2 P 86Document5 pagesJavt 14 I 2 P 86Bhayu RizallinoorNo ratings yet
- Tuberculosis of The Spine Is One of The Oldest Demonstrated Diseases of HumankindDocument32 pagesTuberculosis of The Spine Is One of The Oldest Demonstrated Diseases of HumankindtechcaresystemNo ratings yet
- Hernia de DiscoDocument7 pagesHernia de DiscoEmanoel PachecoNo ratings yet
- Cervical Spine TraumaDocument63 pagesCervical Spine TraumaDr-Gehad Samy HalwagyNo ratings yet
- Radiography of The SpineDocument4 pagesRadiography of The SpineJorge VergaraNo ratings yet
- Spinal Cord InjuryDocument24 pagesSpinal Cord InjuryGayzel Dela CruzNo ratings yet
- Esguince CervicalDocument8 pagesEsguince CervicalpaolalizethsanchezmezaNo ratings yet
- Cervical Myelopathy - ERHDocument42 pagesCervical Myelopathy - ERHAries RHNo ratings yet
- Lecture 6 Lower Limb and Foot AffectionsDocument22 pagesLecture 6 Lower Limb and Foot AffectionsDeep PatelNo ratings yet
- Spinal Cord InjuryDocument37 pagesSpinal Cord Injurylim sjNo ratings yet
- SpondylolisthesisDocument31 pagesSpondylolisthesisMD ABDUR RAHANNo ratings yet
- Radicular SyndromeDocument40 pagesRadicular Syndromeainulhawa89No ratings yet
- Carpal Tunnel Syndrome, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandCarpal Tunnel Syndrome, A Simple Guide To The Condition, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Transverse Myelitis, A Simple Guide To The Condition, Treatment And Related DiseasesFrom EverandTransverse Myelitis, A Simple Guide To The Condition, Treatment And Related DiseasesRating: 5 out of 5 stars5/5 (1)
- Drug Study CardinalDocument21 pagesDrug Study CardinalDrei LanuzoNo ratings yet
- Mitral Valve ProlapseDocument6 pagesMitral Valve ProlapseMary Joy FrancoNo ratings yet
- Ren 13Document1 pageRen 13ray72roNo ratings yet
- RR8 - Van Richten's Guide To The Created PDFDocument98 pagesRR8 - Van Richten's Guide To The Created PDFYukikoSchyzo100% (7)
- Feeding Tube Insertion (Gastrostomy)Document5 pagesFeeding Tube Insertion (Gastrostomy)maredithsaludarNo ratings yet
- PSPv2022 12 02Document37 pagesPSPv2022 12 02ynid wageNo ratings yet
- The Health Consequences of Consuming Cow's MilkDocument124 pagesThe Health Consequences of Consuming Cow's MilkVegan Future86% (7)
- English PDFDocument186 pagesEnglish PDFTusharNo ratings yet
- Efficacy of Cognitive Behaviour Therapy in ManagementDocument5 pagesEfficacy of Cognitive Behaviour Therapy in ManagementIrfan FauziNo ratings yet
- Simple Past and Present PerfectDocument10 pagesSimple Past and Present PerfectNur RudiyantoNo ratings yet
- 7 Health Benefits of A Cold Shower - The Art of ManlinessDocument16 pages7 Health Benefits of A Cold Shower - The Art of ManlinessNick KirkNo ratings yet
- Mike Reinold Shoulder Clinical Exam ChecklistDocument20 pagesMike Reinold Shoulder Clinical Exam ChecklistAdmir100% (1)
- Bissonette, Andrew H. - Chanmugam, Arjun S. - Desai, Sanjay v. - Putman, Shannon B - Infectious Diseases Emergencies (2017, Oxford University Press)Document441 pagesBissonette, Andrew H. - Chanmugam, Arjun S. - Desai, Sanjay v. - Putman, Shannon B - Infectious Diseases Emergencies (2017, Oxford University Press)Bagus Wahyu M.100% (1)
- Review: Lenat Joffe, Elena J LadasDocument11 pagesReview: Lenat Joffe, Elena J LadasGUSTAVO BELLONo ratings yet
- Glenmark - Respicare: TEST PAPER - Microbiology, Disease, Organisms & AntibioticsDocument6 pagesGlenmark - Respicare: TEST PAPER - Microbiology, Disease, Organisms & AntibioticskurutalaNo ratings yet
- Acute Chronic Renal FailureDocument43 pagesAcute Chronic Renal FailureHigh Education100% (1)
- Dust Suppression in Coal Ash Applications: Aaron ValencicDocument6 pagesDust Suppression in Coal Ash Applications: Aaron ValencicSreenubabu KandruNo ratings yet
- Andreasen 1979 - TLCDocument7 pagesAndreasen 1979 - TLCSivaprakash Balasundaram100% (1)
- ZumbaDocument13 pagesZumbaamitsingh_singh041No ratings yet
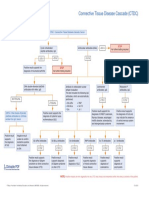
- Connective Tissue Disease CascadeDocument1 pageConnective Tissue Disease CascadeYustina BubnovaNo ratings yet
- Seventy-Fifth World Health Assembly: WHA75/2022/REC/1Document297 pagesSeventy-Fifth World Health Assembly: WHA75/2022/REC/1Paola CronopioNo ratings yet
- 1 PB PDFDocument11 pages1 PB PDFmuhammadkamaraNo ratings yet
- Covid 19Document9 pagesCovid 19abuumaiyoNo ratings yet
- The Short-Form Leeds Dyspepsia Questionnaire Validation StudyDocument10 pagesThe Short-Form Leeds Dyspepsia Questionnaire Validation Studynermal93No ratings yet
- Endocrine Disorders 1234399857677955 1Document130 pagesEndocrine Disorders 1234399857677955 1api-19824701No ratings yet
- Long Runs and Long RidesDocument5 pagesLong Runs and Long RidesGary MollerNo ratings yet