Download as pdf or txt
You might also like
- Operating Instructions: V2500-A1/A5 SERIES Commercial Turbofan Engines On The Airbus A319/A320/A321 Ceo AIRPLANESDocument79 pagesOperating Instructions: V2500-A1/A5 SERIES Commercial Turbofan Engines On The Airbus A319/A320/A321 Ceo AIRPLANESBilal Abbasi100% (2)
- 1magnetic Forces On Wires: Equipment IncludedDocument12 pages1magnetic Forces On Wires: Equipment IncludedDewi Cahya FitriNo ratings yet
- Chemistry Investigatory Project On Bio-Diesel Made by Kamal/KishanDocument15 pagesChemistry Investigatory Project On Bio-Diesel Made by Kamal/KishanKishan Saluja76% (84)
- Use of Artificial Neural Network in Diagnostic PatDocument4 pagesUse of Artificial Neural Network in Diagnostic Patsellappan marappanNo ratings yet
- ScienceDocument1 pageScienceFionaNo ratings yet
- Artificial Neural Networks Based Heart Disease Predictive ApproachDocument4 pagesArtificial Neural Networks Based Heart Disease Predictive ApproachInternational Journal of Application or Innovation in Engineering & ManagementNo ratings yet
- Bmjopen 2018 022810Document15 pagesBmjopen 2018 022810syukronchalimNo ratings yet
- 2019 DsadaşsklDocument8 pages2019 DsadaşsklAhmet KaragozNo ratings yet
- Prediction of Heart Disease Using Neural Network With Back PropagationDocument4 pagesPrediction of Heart Disease Using Neural Network With Back PropagationIntegrated Intelligent ResearchNo ratings yet
- Automatic Seizure Detection Using Three-Dimensional CNN Based On Multi-Channel EEGDocument10 pagesAutomatic Seizure Detection Using Three-Dimensional CNN Based On Multi-Channel EEGDhanalekshmi YedurkarNo ratings yet
- Brain Tumor Classification Using Deep Learning AlgorithmsDocument12 pagesBrain Tumor Classification Using Deep Learning AlgorithmsIJRASETPublicationsNo ratings yet
- Stroke Prediction System Using ANN (Artificial Neural Network)Document3 pagesStroke Prediction System Using ANN (Artificial Neural Network)International Journal of Innovative Science and Research TechnologyNo ratings yet
- ABSTRACT TechnicalDocument2 pagesABSTRACT TechnicalSahil TiwariNo ratings yet
- BP 2Document6 pagesBP 2kandeharikabaiNo ratings yet
- Diagnosis of Pneumonia From Chest X-Ray Images Using Deep LearningDocument5 pagesDiagnosis of Pneumonia From Chest X-Ray Images Using Deep LearningShoumik MuhtasimNo ratings yet
- Transfer LearningDocument7 pagesTransfer LearningAdah EneNo ratings yet
- 2004-Neural Network Classification of Ped - Post FossaDocument10 pages2004-Neural Network Classification of Ped - Post FossaAhmet KaragozNo ratings yet
- Breast Cancer Diagnosis Using Artificial Intelligence Neural NetworksDocument13 pagesBreast Cancer Diagnosis Using Artificial Intelligence Neural NetworksAndy PutraNo ratings yet
- Document3 TexDocument4 pagesDocument3 TexNavin M ANo ratings yet
- Pneumonia Detection Using VGG19 (Group No. 10)Document20 pagesPneumonia Detection Using VGG19 (Group No. 10)Amrit Kumar100% (1)
- Rana 2018Document6 pagesRana 2018smritii bansalNo ratings yet
- Chronic Kidney Disease Prediciton Using Neural NetworksDocument5 pagesChronic Kidney Disease Prediciton Using Neural NetworksNirmal KumarNo ratings yet
- Urinary System Diseases Diagnosis Using Artificial Neural NetworksDocument5 pagesUrinary System Diseases Diagnosis Using Artificial Neural NetworksEsemuze LuckyNo ratings yet
- 2022-CMIG-End-systole and End-Diastole Detection in Short Axis Cine MRI Using A Fully CNN With Dilated ConvolutionsDocument8 pages2022-CMIG-End-systole and End-Diastole Detection in Short Axis Cine MRI Using A Fully CNN With Dilated ConvolutionsZhenyu BuNo ratings yet
- Icec 2020Document5 pagesIcec 2020Nur SakinahNo ratings yet
- Comparison of Different Types of Artificial Neural Networks For Diagnosing Thyroid DiseaseDocument11 pagesComparison of Different Types of Artificial Neural Networks For Diagnosing Thyroid DiseaseSabrina JonesNo ratings yet
- Implementation of An Incremental Deep Learning Model For Survival Prediction of Cardiovascular PatientsDocument9 pagesImplementation of An Incremental Deep Learning Model For Survival Prediction of Cardiovascular PatientsIAES IJAINo ratings yet
- Febrianto 2020 IOP Conf. Ser. Mater. Sci. Eng. 771 012031Document7 pagesFebrianto 2020 IOP Conf. Ser. Mater. Sci. Eng. 771 012031Asma ChikhaouiNo ratings yet
- Pediatric Seizure Forecasting Using Nonlinear Features and Gaussian Mixture Hidden Markov Models On Scalp EEG SignalsDocument6 pagesPediatric Seizure Forecasting Using Nonlinear Features and Gaussian Mixture Hidden Markov Models On Scalp EEG SignalsTanvin AyatNo ratings yet
- 1 s2.0 S2666522022000065 MainDocument13 pages1 s2.0 S2666522022000065 Mainamrusankar4No ratings yet
- Fisrt ReviewDocument62 pagesFisrt ReviewramhudiyaNo ratings yet
- Transfer Learning For Ultrasound ImagesDocument10 pagesTransfer Learning For Ultrasound ImagesKoundinya DesirajuNo ratings yet
- Predicting Outcome For Hospitalized Cardiac Patients Using A Combined Neural Network and Rough Set ApproachDocument4 pagesPredicting Outcome For Hospitalized Cardiac Patients Using A Combined Neural Network and Rough Set ApproachBryancito Chumbes LizarragaNo ratings yet
- Ann Clin Transl Neurol - 2017 - Stinear - PREP2 A Biomarker Based Algorithm For Predicting Upper Limb Function AfterDocument10 pagesAnn Clin Transl Neurol - 2017 - Stinear - PREP2 A Biomarker Based Algorithm For Predicting Upper Limb Function Afterginelly quinteroNo ratings yet
- Abe 2022 Oi 220481 1654263485.26457Document11 pagesAbe 2022 Oi 220481 1654263485.26457b4b758h7jhNo ratings yet
- Nuclear PP Diagnosis FaultDocument9 pagesNuclear PP Diagnosis FaultsuderNo ratings yet
- 19999-Article Text (Manuscript) in DOC or DOCX Format-84173-3!10!20230630Document15 pages19999-Article Text (Manuscript) in DOC or DOCX Format-84173-3!10!20230630Khusnun FirdhaNo ratings yet
- Segmentation of Vestibular Schwannoma From MRI, An Open Annotated Dataset and Baseline AlgorithmDocument6 pagesSegmentation of Vestibular Schwannoma From MRI, An Open Annotated Dataset and Baseline AlgorithmIndra PrimaNo ratings yet
- Analysis of Head CT Scans Flagged by Deep Learning Software For Acute Intracranial HemorrhageDocument6 pagesAnalysis of Head CT Scans Flagged by Deep Learning Software For Acute Intracranial HemorrhageAshish MehtaNo ratings yet
- Campen EllaDocument21 pagesCampen EllaWhy BotherNo ratings yet
- Sompawong 2019Document5 pagesSompawong 2019Mahmudur Rahman27No ratings yet
- Expert Systems With Applications: Xiaolong Zhai, Zhanhong Zhou, Chung TinDocument10 pagesExpert Systems With Applications: Xiaolong Zhai, Zhanhong Zhou, Chung Tinpuneet5246No ratings yet
- A Machine Learning System For Automated Whole-Brain Seizure DetectionDocument20 pagesA Machine Learning System For Automated Whole-Brain Seizure DetectionNEHA BHATINo ratings yet
- 10 1016@j Compbiomed 2019 04 017Document11 pages10 1016@j Compbiomed 2019 04 017tomniucNo ratings yet
- Application of Multi Layer Artificial Neural Network in The Diagnosis System: A Systematic ReviewDocument5 pagesApplication of Multi Layer Artificial Neural Network in The Diagnosis System: A Systematic ReviewIAES IJAINo ratings yet
- 1-S2.0-Neural Network Lisboa2002Document29 pages1-S2.0-Neural Network Lisboa2002Vildson BorbaNo ratings yet
- Transfer Learning For ECG ClassificationDocument12 pagesTransfer Learning For ECG ClassificationAbduljabbar Salem Ba-MahelNo ratings yet
- A Pneumonia Detection Method Based On ImprovedDocument6 pagesA Pneumonia Detection Method Based On ImprovedAmílcar CáceresNo ratings yet
- Risk Management of Investment Projects Based On Artificial Neural NetworkDocument13 pagesRisk Management of Investment Projects Based On Artificial Neural NetworkAakash DebnathNo ratings yet
- Wu 2017Document4 pagesWu 2017Vikas KumarNo ratings yet
- CNN-Based Image Analysis For Malaria Diagnosis: Abstract - Malaria Is A Major Global Health Threat. TheDocument4 pagesCNN-Based Image Analysis For Malaria Diagnosis: Abstract - Malaria Is A Major Global Health Threat. TheMiftahul RakaNo ratings yet
- Deep Learning For Automatically Visual Evoked Potential Classification During Surgical Decompression of Sellar Region TumorDocument7 pagesDeep Learning For Automatically Visual Evoked Potential Classification During Surgical Decompression of Sellar Region TumoradityaNo ratings yet
- Article 1Document4 pagesArticle 1Tashu SardaNo ratings yet
- BackprpDocument6 pagesBackprpAnay ChowdharyNo ratings yet
- Chest X-Ray Analysis Using Deep Learning AlgorithmDocument7 pagesChest X-Ray Analysis Using Deep Learning AlgorithmIJRASETPublicationsNo ratings yet
- Application of Neural Networks in Medical Image Processing: Zhenghao Shi, and Lifeng HeDocument4 pagesApplication of Neural Networks in Medical Image Processing: Zhenghao Shi, and Lifeng HeDanielle PerryNo ratings yet
- Automatic Prediction of Diabetic Retinopathy and Glaucoma Through Retinal Image Analysis and Data Mining Techniques PDFDocument4 pagesAutomatic Prediction of Diabetic Retinopathy and Glaucoma Through Retinal Image Analysis and Data Mining Techniques PDFMohammad RofiiNo ratings yet
- AB Report Group 2Document14 pagesAB Report Group 2Abyan HarahapNo ratings yet
- Project PresentationDocument3 pagesProject PresentationGourab PalNo ratings yet
- Artificial Intelligence 1Document8 pagesArtificial Intelligence 1Andy BaiNo ratings yet
- Teja - Technical Seminar PresentationDocument28 pagesTeja - Technical Seminar PresentationArjun P LinekajeNo ratings yet
- Predicting Heart Disease Using Neural NetworksDocument7 pagesPredicting Heart Disease Using Neural NetworksNitya BoyinaNo ratings yet
- Interfacing Bioelectronics and Biomedical SensingFrom EverandInterfacing Bioelectronics and Biomedical SensingHung CaoNo ratings yet
- Myocardial InfarctionDocument6 pagesMyocardial InfarctionDewi Cahya FitriNo ratings yet
- Detection of Myocardial Infarction in 12 Lead ECG Using Support Vector Machine PDFDocument10 pagesDetection of Myocardial Infarction in 12 Lead ECG Using Support Vector Machine PDFDewi Cahya FitriNo ratings yet
- Comparison Between Type-2 and Type-1 Myocardial Infarction: Clinical Features, Treatment Strategies and OutcomesDocument8 pagesComparison Between Type-2 and Type-1 Myocardial Infarction: Clinical Features, Treatment Strategies and OutcomesDewi Cahya FitriNo ratings yet
- BME 301: Biomedical Sensors: Lecture Note 3: Bioelectric Potentials and Biopotential ElectrodesDocument67 pagesBME 301: Biomedical Sensors: Lecture Note 3: Bioelectric Potentials and Biopotential ElectrodesDewi Cahya FitriNo ratings yet
- 3 6Document3 pages3 6Dewi Cahya FitriNo ratings yet
- Discovery Learning Dilaksanakan Dengan Langkah-Langkah: (A)Document6 pagesDiscovery Learning Dilaksanakan Dengan Langkah-Langkah: (A)Dewi Cahya FitriNo ratings yet
- Lecture 14 - Housing For All Mission (PMAY) & Technology Sub-MissionDocument15 pagesLecture 14 - Housing For All Mission (PMAY) & Technology Sub-MissionRadhika KhandelwalNo ratings yet
- C++ Exercises IIDocument4 pagesC++ Exercises IIZaid Al-Ali50% (2)
- Food Composition TableDocument3 pagesFood Composition Tablehafeesadetunji01No ratings yet
- A Comparative Study On Selected Fitness Components of 13-19 Years Female Basketball and Volleyball PlayersDocument11 pagesA Comparative Study On Selected Fitness Components of 13-19 Years Female Basketball and Volleyball PlayersAnonymous CwJeBCAXpNo ratings yet
- Process Oriented Measurements and Improvements - An Analysis of The OFCE-process at Tetra Pak BU DBFDocument5 pagesProcess Oriented Measurements and Improvements - An Analysis of The OFCE-process at Tetra Pak BU DBFĐạt Nguyễn ThànhNo ratings yet
- LLaVA MEDDocument17 pagesLLaVA MED권오민 / 학생 / 전기·정보공학부No ratings yet
- Full Download Retailing Management Levy 9th Edition Solutions Manual PDF Full ChapterDocument36 pagesFull Download Retailing Management Levy 9th Edition Solutions Manual PDF Full Chapterbeastlyfulberj6gkg100% (20)
- System Manuals: EBTS and Integrated Site ControllerDocument3 pagesSystem Manuals: EBTS and Integrated Site ControllerIsac LimaNo ratings yet
- Alywn Cosgrove Real World Fat Loss PDFDocument75 pagesAlywn Cosgrove Real World Fat Loss PDFJM Gym Manticao100% (1)
- Deliverable 5 - Trend Analysis & PresentationDocument6 pagesDeliverable 5 - Trend Analysis & PresentationRamizNo ratings yet
- Show All Work For Credit. Leave All Answers As Simplified FractionsDocument10 pagesShow All Work For Credit. Leave All Answers As Simplified FractionsAliRazaNo ratings yet
- Proposal Nanotechnology in GeotechnicsDocument4 pagesProposal Nanotechnology in GeotechnicsMOHAMED DiriyeNo ratings yet
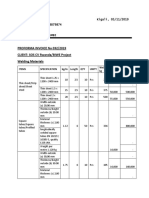
- KBN Proforma BIWE Welding and Plumbing Materials.Document23 pagesKBN Proforma BIWE Welding and Plumbing Materials.Gilbert KamanziNo ratings yet
- Second Year Mba Syllabus (Only Electives) Third Semester Functional Area: MarketingDocument21 pagesSecond Year Mba Syllabus (Only Electives) Third Semester Functional Area: MarketingSatya ReddyNo ratings yet
- World Islamic Banking Competitiveness Report 2013 - 2014Document84 pagesWorld Islamic Banking Competitiveness Report 2013 - 2014Lena HafizNo ratings yet
- 3D PythagorasDocument4 pages3D Pythagorasraghed alkelaniNo ratings yet
- Location Decisions: Revision AnswersDocument4 pagesLocation Decisions: Revision AnswersZakir HalilovNo ratings yet
- DLL MAPEH7 - 3rd QuarterDocument69 pagesDLL MAPEH7 - 3rd QuarterArah May RobosaNo ratings yet
- Lesson1: Cell, The Basic Unit of LifeDocument4 pagesLesson1: Cell, The Basic Unit of Lifedream kingNo ratings yet
- 07-09-14 EditionDocument28 pages07-09-14 EditionSan Mateo Daily JournalNo ratings yet
- Dumps: Pdfdumps Can Solve All Your It Exam Problems and Broaden Your KnowledgeDocument10 pagesDumps: Pdfdumps Can Solve All Your It Exam Problems and Broaden Your KnowledgeyeddekfiihNo ratings yet
- Astm A307Document6 pagesAstm A307thakrarhits100% (3)
- Trust Bank Account InstructionsDocument5 pagesTrust Bank Account InstructionsGregNo ratings yet
- Tekla StructuresDocument2 pagesTekla StructurescallofdutyondutyNo ratings yet
- CSMI v. TrinityDocument22 pagesCSMI v. TrinityCTV OttawaNo ratings yet
- Adv. Simi Pillay-Van Graan CVDocument14 pagesAdv. Simi Pillay-Van Graan CVDana JonesNo ratings yet
- OCH NH CH CH NH CH CH CH Si OCH OCHDocument2 pagesOCH NH CH CH NH CH CH CH Si OCH OCHPermesh GoelNo ratings yet
- Trading PlanDocument12 pagesTrading Planpeterhash5No ratings yet