
Ibyt 13 I 4 P 659
Ibyt 13 I 4 P 659
You might also like
- Common JCI CBAHI Survey QuestionsDocument371 pagesCommon JCI CBAHI Survey Questionsshadi alshadafan100% (4)
- Executive Order - Municipal Rdana Team (Reorganization)Document2 pagesExecutive Order - Municipal Rdana Team (Reorganization)June E. Jaramillo100% (8)
- Spears Opposition Jan 14Document36 pagesSpears Opposition Jan 14THROnline100% (1)
- Company Profile PT KEIDocument6 pagesCompany Profile PT KEIMochammad IrchamNo ratings yet
- MCQs Developmental PsychologyDocument28 pagesMCQs Developmental PsychologyUrooj Jamil Ahmad50% (4)
- Iop HT 7Document9 pagesIop HT 7Peer TutorNo ratings yet
- What Is NTGDocument4 pagesWhat Is NTGSonia RogersNo ratings yet
- Normal Tension Glaucoma: A Different Disease?: Kuldev SinghDocument3 pagesNormal Tension Glaucoma: A Different Disease?: Kuldev SinghRasha Mounir Abdel-Kader El-TanamlyNo ratings yet
- Normal Tension GlaucomaDocument7 pagesNormal Tension GlaucomaSonia RogersNo ratings yet
- Palmberg 2004Document14 pagesPalmberg 2004nishtha singhNo ratings yet
- Normal-Tension (Low-Tension) GlaucomaDocument13 pagesNormal-Tension (Low-Tension) GlaucomaFidela OliviaNo ratings yet
- NTG Practical ApproachDocument6 pagesNTG Practical ApproachRasha Mounir Abdel-Kader El-TanamlyNo ratings yet
- 2018 Heart Rate Variability - The Comparison Between High Tension and Normal Tension GlaucomaDocument11 pages2018 Heart Rate Variability - The Comparison Between High Tension and Normal Tension GlaucomaAlex KwanNo ratings yet
- The Need To Maintain IOP Over 24hrs ... Article From Journal of Current Glaucoma Practice Sep-Dec2012Document4 pagesThe Need To Maintain IOP Over 24hrs ... Article From Journal of Current Glaucoma Practice Sep-Dec2012Tanmoy SinghaNo ratings yet
- J Curr Glauc 2015Document6 pagesJ Curr Glauc 2015Widya azharNo ratings yet
- Fnmol 07 00038Document15 pagesFnmol 07 00038Ratih Kusuma DewiNo ratings yet
- The Glymphatic System and New Etiopathogenic Hypotheses Concerning Glaucoma Based On Pilot Study On Glaucoma Patients Who Underwent Osteopathic Manipulative Treatment (OMT)Document7 pagesThe Glymphatic System and New Etiopathogenic Hypotheses Concerning Glaucoma Based On Pilot Study On Glaucoma Patients Who Underwent Osteopathic Manipulative Treatment (OMT)BOHR International Journal of Current Research in Optometry and Ophthalmology (BIJCROO)No ratings yet
- Perfusionpressure GLAUCOMA IOPDocument1 pagePerfusionpressure GLAUCOMA IOPJuan Andrés Castaño CisfNo ratings yet
- DM Dan GlaukomaDocument5 pagesDM Dan GlaukomaYandhie RahmanNo ratings yet
- Ceo 12718Document2 pagesCeo 12718fdfvzcr6qdNo ratings yet
- Lutfi-Full Paper-Pit 2024Document6 pagesLutfi-Full Paper-Pit 2024Lutfi MaulanaNo ratings yet
- Gfad 118Document10 pagesGfad 118pepegiovannyNo ratings yet
- ACNRJA10 Review ArticleDocument3 pagesACNRJA10 Review ArticleNouchan NoupNo ratings yet
- Lens-Based Glaucoma Surgery: Using Cataract Surgery To Reduce Intraocular PressureDocument8 pagesLens-Based Glaucoma Surgery: Using Cataract Surgery To Reduce Intraocular PressureSehat JanuarNo ratings yet
- Target IopDocument18 pagesTarget IopdrheriNo ratings yet
- Normal-Tension Glaucoma and Obstructive Sleep Apnea SyndromeDocument6 pagesNormal-Tension Glaucoma and Obstructive Sleep Apnea SyndromeyuliNo ratings yet
- Glaucoma ArticleDocument5 pagesGlaucoma ArticleNikhil PaulNo ratings yet
- 86 Normal Low Tension Glaucoma PDFDocument4 pages86 Normal Low Tension Glaucoma PDFSherZalattha KuchikiElfNo ratings yet
- Erc e HtaDocument10 pagesErc e HtamiguelalmenarezNo ratings yet
- Pressure Fluctuations in GlaucomaDocument6 pagesPressure Fluctuations in GlaucomaTushar BatraNo ratings yet
- Am J Ophthalmol 2004 - p401Document6 pagesAm J Ophthalmol 2004 - p401Abrilia OctafijayantiNo ratings yet
- Tugas Akademik 13-Journal Reading 4-Glaukoma-Galuh Yulieta - 240215 - 072026Document8 pagesTugas Akademik 13-Journal Reading 4-Glaukoma-Galuh Yulieta - 240215 - 072026Arina SetyaningrumNo ratings yet
- Glaucoma and Diabetes - Is There An Association? Jain Shashi, Lakhtakia Sujata, Tirkey Eva Rani, Jain Sheel ChandraDocument5 pagesGlaucoma and Diabetes - Is There An Association? Jain Shashi, Lakhtakia Sujata, Tirkey Eva Rani, Jain Sheel ChandranjmdrNo ratings yet
- GlaucomaDocument11 pagesGlaucomaerkalemNo ratings yet
- Pubmed 3Document11 pagesPubmed 3Adam PrabataNo ratings yet
- Imp Landmark Glauc StudiesDocument100 pagesImp Landmark Glauc StudiesASHOK KUMAR SINGHNo ratings yet
- Biomedicines 11 03146Document10 pagesBiomedicines 11 03146Andrés HpNo ratings yet
- Statin and GalucomaDocument6 pagesStatin and Galucomawimakrifah istiqomahNo ratings yet
- 2017 Article 1861Document12 pages2017 Article 1861nanaNo ratings yet
- Cataract Surgery and Intraocular Pressure in Glaucoma: ReviewDocument8 pagesCataract Surgery and Intraocular Pressure in Glaucoma: ReviewJackNo ratings yet
- I1552 5783 60 14 4548 PDFDocument8 pagesI1552 5783 60 14 4548 PDFNetflix DheaNo ratings yet
- Lesiones Del SPAIN. Rev Esp Cardiol 2018Document3 pagesLesiones Del SPAIN. Rev Esp Cardiol 2018Ernesto J. Rocha ReyesNo ratings yet
- Intraocular Pressure in An American Community: The Deover Dom Eye StudyDocument5 pagesIntraocular Pressure in An American Community: The Deover Dom Eye StudyAngkat Prasetya Abdi NegaraNo ratings yet
- ETM 2021-03-Association of Obstructive Sleep Apnea-Hypopnea Syndrome With Glaucomatous Optic Neuropathy and Ocular Blood FlowDocument7 pagesETM 2021-03-Association of Obstructive Sleep Apnea-Hypopnea Syndrome With Glaucomatous Optic Neuropathy and Ocular Blood FlowMarcos FerrazNo ratings yet
- CRST1111 Cs Mini ZabriskieDocument2 pagesCRST1111 Cs Mini ZabriskieTyasBanggaPribadieNo ratings yet
- Link Between Neurodegeneration and Trabecular Meshwork Injury in Glaucomatous PatientsDocument7 pagesLink Between Neurodegeneration and Trabecular Meshwork Injury in Glaucomatous Patientsfaruq azmiNo ratings yet
- Simplifying Target Intraocular Pressure For.4Document11 pagesSimplifying Target Intraocular Pressure For.4syntacs skNo ratings yet
- Jovr 17 27Document6 pagesJovr 17 27fdfvzcr6qdNo ratings yet
- Glaucoma Suspect: Diagnosis and Management: Risk FactorsDocument5 pagesGlaucoma Suspect: Diagnosis and Management: Risk FactorsKrisno ParammanganNo ratings yet
- PIIS0002939422003774Document10 pagesPIIS0002939422003774Anca Florina GaceaNo ratings yet
- Nutritional Supplementation in The Treatment of Glaucoma - A Systematic Review 2018 PDFDocument64 pagesNutritional Supplementation in The Treatment of Glaucoma - A Systematic Review 2018 PDFjvprasad100% (1)
- The Effect of Prostaglandin Analogues On Central Corneal Thickness in Patients With GlaucomaDocument4 pagesThe Effect of Prostaglandin Analogues On Central Corneal Thickness in Patients With GlaucomarandyhermawanNo ratings yet
- Iop HT 8Document11 pagesIop HT 8Peer TutorNo ratings yet
- Jurnal GlaukomaDocument6 pagesJurnal GlaukomaIntan NarariaNo ratings yet
- Gfad118 231203 161822Document10 pagesGfad118 231203 161822eduardo veNo ratings yet
- Jurnal Mata 3Document4 pagesJurnal Mata 3Ami AntariksawatiNo ratings yet
- 196 FullDocument7 pages196 FullPeer TutorNo ratings yet
- More Cardiovascular Outcome Trials in DiabetesDocument1 pageMore Cardiovascular Outcome Trials in Diabetesianelli93No ratings yet
- Steriod Cataract PDFDocument4 pagesSteriod Cataract PDFLisa IskandarNo ratings yet
- Update On Normal Tension Glaucoma: Review ArticleDocument5 pagesUpdate On Normal Tension Glaucoma: Review ArticleNur Rakhma AkmaliaNo ratings yet
- PRIMARY OPEN ANGLE GLAUCOMA AND RELEVANT CLINICAL STUDIES NotesDocument16 pagesPRIMARY OPEN ANGLE GLAUCOMA AND RELEVANT CLINICAL STUDIES Notessarjak shahNo ratings yet
- gt0513 LandmarkDocument5 pagesgt0513 Landmarkjoe lopasoNo ratings yet
- Landmark Studies in GlaucomaDocument53 pagesLandmark Studies in GlaucomaDrEknathPawarNo ratings yet
- Jurnal Mata 2Document30 pagesJurnal Mata 2Reza AryantiNo ratings yet
- Biophysical Properties in Glaucoma: Diagnostic TechnologiesFrom EverandBiophysical Properties in Glaucoma: Diagnostic TechnologiesIngrida JanulevicieneNo ratings yet
- Imm Rota NewDocument1 pageImm Rota NewdrshariquennazirNo ratings yet
- National Security Threats in The PhilippinesDocument1 pageNational Security Threats in The PhilippinesJonahweine BarramedaNo ratings yet
- Water Safety Search and Rescue ManualDocument8 pagesWater Safety Search and Rescue ManualRico Astillero100% (1)
- Normal 5fc8e5cc9d923Document3 pagesNormal 5fc8e5cc9d923sidra darNo ratings yet
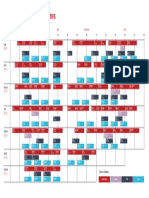
- Planning Cours Wellness Sport Club VIlleurbanneDocument1 pagePlanning Cours Wellness Sport Club VIlleurbanneAno NymeNo ratings yet
- NeurotransmittersDocument11 pagesNeurotransmittersapi-286518624100% (1)
- Dalair LimitedHealthSafetyManualDocument25 pagesDalair LimitedHealthSafetyManualRidarto LubisNo ratings yet
- EVIS-X1 E-Brochure EN 86578Document15 pagesEVIS-X1 E-Brochure EN 86578rq yNo ratings yet
- Sexual Orientation Scale 2020Document10 pagesSexual Orientation Scale 2020MaqboolNo ratings yet
- NTS Sample Past Papers Audit Department Analytical ReasoningDocument8 pagesNTS Sample Past Papers Audit Department Analytical ReasoningZia Ur RehmanNo ratings yet
- 10 1016@j JDSR 2020 08 003Document8 pages10 1016@j JDSR 2020 08 003maulana harahapNo ratings yet
- OrthoNeuro's Mark Gittins Is One of Three Orthopedic Surgeons Worldwide To Utilize New Handheld Robotics PlatformDocument3 pagesOrthoNeuro's Mark Gittins Is One of Three Orthopedic Surgeons Worldwide To Utilize New Handheld Robotics PlatformPR.comNo ratings yet
- Physical AssessmentDocument37 pagesPhysical AssessmentMaria ThereseNo ratings yet
- 2023 Grade 9 Lo Final ExaminationDocument9 pages2023 Grade 9 Lo Final Examinationmapulacatherine33No ratings yet
- Consent in Pediatric Urology First Edition Prasad Godbole Duncan PDFDocument284 pagesConsent in Pediatric Urology First Edition Prasad Godbole Duncan PDFMarcela Osorio DugandNo ratings yet
- Argumentative EssayDocument4 pagesArgumentative Essayapi-331227590No ratings yet
- Project On GothicDocument14 pagesProject On GothicMazana ÁngelNo ratings yet
- TOPIC 2. Protocol and Amenities in The Uniformed Service - 104604Document2 pagesTOPIC 2. Protocol and Amenities in The Uniformed Service - 104604Khalvinclyde BernabeNo ratings yet
- Positive PsychDocument2 pagesPositive PsychZirah Lee ValledorNo ratings yet
- Leap Study Matter-5Document40 pagesLeap Study Matter-5Ravi SatyapalNo ratings yet
- Effects of A Capacitive-Resistive Electric Transfer Therapy OnDocument8 pagesEffects of A Capacitive-Resistive Electric Transfer Therapy OnAnna Lygia LunardiNo ratings yet
- Artikel 3Document23 pagesArtikel 3Hadian UwuoNo ratings yet
- 5 - Outstanding 4 - Very Satisfactory 3 - Satisfactory 2 - Unsatisfactory 1 - PoorDocument4 pages5 - Outstanding 4 - Very Satisfactory 3 - Satisfactory 2 - Unsatisfactory 1 - PoorJohnny Bananao jrNo ratings yet
- Gibbon Brochure IngDocument21 pagesGibbon Brochure Ingkanhaiya kumarNo ratings yet
- QuestionnaireDocument4 pagesQuestionnaireIan AtienzaNo ratings yet
























































































Download as pdf or txt
You might also like
- Common JCI CBAHI Survey QuestionsDocument371 pagesCommon JCI CBAHI Survey Questionsshadi alshadafan100% (4)
- Executive Order - Municipal Rdana Team (Reorganization)Document2 pagesExecutive Order - Municipal Rdana Team (Reorganization)June E. Jaramillo100% (8)
- Spears Opposition Jan 14Document36 pagesSpears Opposition Jan 14THROnline100% (1)
- Company Profile PT KEIDocument6 pagesCompany Profile PT KEIMochammad IrchamNo ratings yet
- MCQs Developmental PsychologyDocument28 pagesMCQs Developmental PsychologyUrooj Jamil Ahmad50% (4)
- Iop HT 7Document9 pagesIop HT 7Peer TutorNo ratings yet
- What Is NTGDocument4 pagesWhat Is NTGSonia RogersNo ratings yet
- Normal Tension Glaucoma: A Different Disease?: Kuldev SinghDocument3 pagesNormal Tension Glaucoma: A Different Disease?: Kuldev SinghRasha Mounir Abdel-Kader El-TanamlyNo ratings yet
- Normal Tension GlaucomaDocument7 pagesNormal Tension GlaucomaSonia RogersNo ratings yet
- Palmberg 2004Document14 pagesPalmberg 2004nishtha singhNo ratings yet
- Normal-Tension (Low-Tension) GlaucomaDocument13 pagesNormal-Tension (Low-Tension) GlaucomaFidela OliviaNo ratings yet
- NTG Practical ApproachDocument6 pagesNTG Practical ApproachRasha Mounir Abdel-Kader El-TanamlyNo ratings yet
- 2018 Heart Rate Variability - The Comparison Between High Tension and Normal Tension GlaucomaDocument11 pages2018 Heart Rate Variability - The Comparison Between High Tension and Normal Tension GlaucomaAlex KwanNo ratings yet
- The Need To Maintain IOP Over 24hrs ... Article From Journal of Current Glaucoma Practice Sep-Dec2012Document4 pagesThe Need To Maintain IOP Over 24hrs ... Article From Journal of Current Glaucoma Practice Sep-Dec2012Tanmoy SinghaNo ratings yet
- J Curr Glauc 2015Document6 pagesJ Curr Glauc 2015Widya azharNo ratings yet
- Fnmol 07 00038Document15 pagesFnmol 07 00038Ratih Kusuma DewiNo ratings yet
- The Glymphatic System and New Etiopathogenic Hypotheses Concerning Glaucoma Based On Pilot Study On Glaucoma Patients Who Underwent Osteopathic Manipulative Treatment (OMT)Document7 pagesThe Glymphatic System and New Etiopathogenic Hypotheses Concerning Glaucoma Based On Pilot Study On Glaucoma Patients Who Underwent Osteopathic Manipulative Treatment (OMT)BOHR International Journal of Current Research in Optometry and Ophthalmology (BIJCROO)No ratings yet
- Perfusionpressure GLAUCOMA IOPDocument1 pagePerfusionpressure GLAUCOMA IOPJuan Andrés Castaño CisfNo ratings yet
- DM Dan GlaukomaDocument5 pagesDM Dan GlaukomaYandhie RahmanNo ratings yet
- Ceo 12718Document2 pagesCeo 12718fdfvzcr6qdNo ratings yet
- Lutfi-Full Paper-Pit 2024Document6 pagesLutfi-Full Paper-Pit 2024Lutfi MaulanaNo ratings yet
- Gfad 118Document10 pagesGfad 118pepegiovannyNo ratings yet
- ACNRJA10 Review ArticleDocument3 pagesACNRJA10 Review ArticleNouchan NoupNo ratings yet
- Lens-Based Glaucoma Surgery: Using Cataract Surgery To Reduce Intraocular PressureDocument8 pagesLens-Based Glaucoma Surgery: Using Cataract Surgery To Reduce Intraocular PressureSehat JanuarNo ratings yet
- Target IopDocument18 pagesTarget IopdrheriNo ratings yet
- Normal-Tension Glaucoma and Obstructive Sleep Apnea SyndromeDocument6 pagesNormal-Tension Glaucoma and Obstructive Sleep Apnea SyndromeyuliNo ratings yet
- Glaucoma ArticleDocument5 pagesGlaucoma ArticleNikhil PaulNo ratings yet
- 86 Normal Low Tension Glaucoma PDFDocument4 pages86 Normal Low Tension Glaucoma PDFSherZalattha KuchikiElfNo ratings yet
- Erc e HtaDocument10 pagesErc e HtamiguelalmenarezNo ratings yet
- Pressure Fluctuations in GlaucomaDocument6 pagesPressure Fluctuations in GlaucomaTushar BatraNo ratings yet
- Am J Ophthalmol 2004 - p401Document6 pagesAm J Ophthalmol 2004 - p401Abrilia OctafijayantiNo ratings yet
- Tugas Akademik 13-Journal Reading 4-Glaukoma-Galuh Yulieta - 240215 - 072026Document8 pagesTugas Akademik 13-Journal Reading 4-Glaukoma-Galuh Yulieta - 240215 - 072026Arina SetyaningrumNo ratings yet
- Glaucoma and Diabetes - Is There An Association? Jain Shashi, Lakhtakia Sujata, Tirkey Eva Rani, Jain Sheel ChandraDocument5 pagesGlaucoma and Diabetes - Is There An Association? Jain Shashi, Lakhtakia Sujata, Tirkey Eva Rani, Jain Sheel ChandranjmdrNo ratings yet
- GlaucomaDocument11 pagesGlaucomaerkalemNo ratings yet
- Pubmed 3Document11 pagesPubmed 3Adam PrabataNo ratings yet
- Imp Landmark Glauc StudiesDocument100 pagesImp Landmark Glauc StudiesASHOK KUMAR SINGHNo ratings yet
- Biomedicines 11 03146Document10 pagesBiomedicines 11 03146Andrés HpNo ratings yet
- Statin and GalucomaDocument6 pagesStatin and Galucomawimakrifah istiqomahNo ratings yet
- 2017 Article 1861Document12 pages2017 Article 1861nanaNo ratings yet
- Cataract Surgery and Intraocular Pressure in Glaucoma: ReviewDocument8 pagesCataract Surgery and Intraocular Pressure in Glaucoma: ReviewJackNo ratings yet
- I1552 5783 60 14 4548 PDFDocument8 pagesI1552 5783 60 14 4548 PDFNetflix DheaNo ratings yet
- Lesiones Del SPAIN. Rev Esp Cardiol 2018Document3 pagesLesiones Del SPAIN. Rev Esp Cardiol 2018Ernesto J. Rocha ReyesNo ratings yet
- Intraocular Pressure in An American Community: The Deover Dom Eye StudyDocument5 pagesIntraocular Pressure in An American Community: The Deover Dom Eye StudyAngkat Prasetya Abdi NegaraNo ratings yet
- ETM 2021-03-Association of Obstructive Sleep Apnea-Hypopnea Syndrome With Glaucomatous Optic Neuropathy and Ocular Blood FlowDocument7 pagesETM 2021-03-Association of Obstructive Sleep Apnea-Hypopnea Syndrome With Glaucomatous Optic Neuropathy and Ocular Blood FlowMarcos FerrazNo ratings yet
- CRST1111 Cs Mini ZabriskieDocument2 pagesCRST1111 Cs Mini ZabriskieTyasBanggaPribadieNo ratings yet
- Link Between Neurodegeneration and Trabecular Meshwork Injury in Glaucomatous PatientsDocument7 pagesLink Between Neurodegeneration and Trabecular Meshwork Injury in Glaucomatous Patientsfaruq azmiNo ratings yet
- Simplifying Target Intraocular Pressure For.4Document11 pagesSimplifying Target Intraocular Pressure For.4syntacs skNo ratings yet
- Jovr 17 27Document6 pagesJovr 17 27fdfvzcr6qdNo ratings yet
- Glaucoma Suspect: Diagnosis and Management: Risk FactorsDocument5 pagesGlaucoma Suspect: Diagnosis and Management: Risk FactorsKrisno ParammanganNo ratings yet
- PIIS0002939422003774Document10 pagesPIIS0002939422003774Anca Florina GaceaNo ratings yet
- Nutritional Supplementation in The Treatment of Glaucoma - A Systematic Review 2018 PDFDocument64 pagesNutritional Supplementation in The Treatment of Glaucoma - A Systematic Review 2018 PDFjvprasad100% (1)
- The Effect of Prostaglandin Analogues On Central Corneal Thickness in Patients With GlaucomaDocument4 pagesThe Effect of Prostaglandin Analogues On Central Corneal Thickness in Patients With GlaucomarandyhermawanNo ratings yet
- Iop HT 8Document11 pagesIop HT 8Peer TutorNo ratings yet
- Jurnal GlaukomaDocument6 pagesJurnal GlaukomaIntan NarariaNo ratings yet
- Gfad118 231203 161822Document10 pagesGfad118 231203 161822eduardo veNo ratings yet
- Jurnal Mata 3Document4 pagesJurnal Mata 3Ami AntariksawatiNo ratings yet
- 196 FullDocument7 pages196 FullPeer TutorNo ratings yet
- More Cardiovascular Outcome Trials in DiabetesDocument1 pageMore Cardiovascular Outcome Trials in Diabetesianelli93No ratings yet
- Steriod Cataract PDFDocument4 pagesSteriod Cataract PDFLisa IskandarNo ratings yet
- Update On Normal Tension Glaucoma: Review ArticleDocument5 pagesUpdate On Normal Tension Glaucoma: Review ArticleNur Rakhma AkmaliaNo ratings yet
- PRIMARY OPEN ANGLE GLAUCOMA AND RELEVANT CLINICAL STUDIES NotesDocument16 pagesPRIMARY OPEN ANGLE GLAUCOMA AND RELEVANT CLINICAL STUDIES Notessarjak shahNo ratings yet
- gt0513 LandmarkDocument5 pagesgt0513 Landmarkjoe lopasoNo ratings yet
- Landmark Studies in GlaucomaDocument53 pagesLandmark Studies in GlaucomaDrEknathPawarNo ratings yet
- Jurnal Mata 2Document30 pagesJurnal Mata 2Reza AryantiNo ratings yet
- Biophysical Properties in Glaucoma: Diagnostic TechnologiesFrom EverandBiophysical Properties in Glaucoma: Diagnostic TechnologiesIngrida JanulevicieneNo ratings yet
- Imm Rota NewDocument1 pageImm Rota NewdrshariquennazirNo ratings yet
- National Security Threats in The PhilippinesDocument1 pageNational Security Threats in The PhilippinesJonahweine BarramedaNo ratings yet
- Water Safety Search and Rescue ManualDocument8 pagesWater Safety Search and Rescue ManualRico Astillero100% (1)
- Normal 5fc8e5cc9d923Document3 pagesNormal 5fc8e5cc9d923sidra darNo ratings yet
- Planning Cours Wellness Sport Club VIlleurbanneDocument1 pagePlanning Cours Wellness Sport Club VIlleurbanneAno NymeNo ratings yet
- NeurotransmittersDocument11 pagesNeurotransmittersapi-286518624100% (1)
- Dalair LimitedHealthSafetyManualDocument25 pagesDalair LimitedHealthSafetyManualRidarto LubisNo ratings yet
- EVIS-X1 E-Brochure EN 86578Document15 pagesEVIS-X1 E-Brochure EN 86578rq yNo ratings yet
- Sexual Orientation Scale 2020Document10 pagesSexual Orientation Scale 2020MaqboolNo ratings yet
- NTS Sample Past Papers Audit Department Analytical ReasoningDocument8 pagesNTS Sample Past Papers Audit Department Analytical ReasoningZia Ur RehmanNo ratings yet
- 10 1016@j JDSR 2020 08 003Document8 pages10 1016@j JDSR 2020 08 003maulana harahapNo ratings yet
- OrthoNeuro's Mark Gittins Is One of Three Orthopedic Surgeons Worldwide To Utilize New Handheld Robotics PlatformDocument3 pagesOrthoNeuro's Mark Gittins Is One of Three Orthopedic Surgeons Worldwide To Utilize New Handheld Robotics PlatformPR.comNo ratings yet
- Physical AssessmentDocument37 pagesPhysical AssessmentMaria ThereseNo ratings yet
- 2023 Grade 9 Lo Final ExaminationDocument9 pages2023 Grade 9 Lo Final Examinationmapulacatherine33No ratings yet
- Consent in Pediatric Urology First Edition Prasad Godbole Duncan PDFDocument284 pagesConsent in Pediatric Urology First Edition Prasad Godbole Duncan PDFMarcela Osorio DugandNo ratings yet
- Argumentative EssayDocument4 pagesArgumentative Essayapi-331227590No ratings yet
- Project On GothicDocument14 pagesProject On GothicMazana ÁngelNo ratings yet
- TOPIC 2. Protocol and Amenities in The Uniformed Service - 104604Document2 pagesTOPIC 2. Protocol and Amenities in The Uniformed Service - 104604Khalvinclyde BernabeNo ratings yet
- Positive PsychDocument2 pagesPositive PsychZirah Lee ValledorNo ratings yet
- Leap Study Matter-5Document40 pagesLeap Study Matter-5Ravi SatyapalNo ratings yet
- Effects of A Capacitive-Resistive Electric Transfer Therapy OnDocument8 pagesEffects of A Capacitive-Resistive Electric Transfer Therapy OnAnna Lygia LunardiNo ratings yet
- Artikel 3Document23 pagesArtikel 3Hadian UwuoNo ratings yet
- 5 - Outstanding 4 - Very Satisfactory 3 - Satisfactory 2 - Unsatisfactory 1 - PoorDocument4 pages5 - Outstanding 4 - Very Satisfactory 3 - Satisfactory 2 - Unsatisfactory 1 - PoorJohnny Bananao jrNo ratings yet
- Gibbon Brochure IngDocument21 pagesGibbon Brochure Ingkanhaiya kumarNo ratings yet
- QuestionnaireDocument4 pagesQuestionnaireIan AtienzaNo ratings yet