
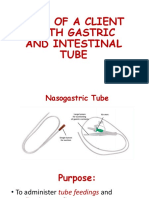
Blakemore Tubing
Blakemore Tubing
You might also like
- Surgery OsceDocument69 pagesSurgery OsceRebecca BrandonNo ratings yet
- Water Seal DrainageDocument6 pagesWater Seal DrainageAmit MartinNo ratings yet
- .archNG - Parenteral NutritionDocument77 pages.archNG - Parenteral NutritionBidhya GuptaNo ratings yet
- Objectives: at The End of The Discussion The Students Will Be Able ToDocument6 pagesObjectives: at The End of The Discussion The Students Will Be Able ToMichael Angelo SeñaNo ratings yet
- Ryle's Tube (Nasogastric Tube)Document41 pagesRyle's Tube (Nasogastric Tube)Sandhya BasnetNo ratings yet
- Chest IntubationDocument42 pagesChest IntubationdrusmanjamilhcmdNo ratings yet
- Nasogastric Intubation: DR - Efman.E.U.Manawan Mkes.,Spb-KbdDocument32 pagesNasogastric Intubation: DR - Efman.E.U.Manawan Mkes.,Spb-KbdNur Ilmi SofiahNo ratings yet
- Nursing Procedures 2003Document11 pagesNursing Procedures 2003jackson2494100% (1)
- NG Tube Lictures 2023Document22 pagesNG Tube Lictures 2023ALi NursingNo ratings yet
- Objectives: Intestinal Tube InsertionDocument28 pagesObjectives: Intestinal Tube Insertion2013SecBNo ratings yet
- Nasogastric Tube NGT 1215082454278959 8Document107 pagesNasogastric Tube NGT 1215082454278959 8Raquel M. MendozaNo ratings yet
- Common Respiratory InterventionsDocument10 pagesCommon Respiratory InterventionsAngel Joy CatalanNo ratings yet
- Administering An EnemaDocument17 pagesAdministering An EnemaAngela Faye CallejaNo ratings yet
- Care of Patient With: Chest DrainageDocument29 pagesCare of Patient With: Chest DrainageMSc. PreviousNo ratings yet
- Group 2 - Rose & Sadava - Chest Tube InsertionDocument19 pagesGroup 2 - Rose & Sadava - Chest Tube InsertionRay Anthony RoseNo ratings yet
- Inserting Nasogastric TubeDocument4 pagesInserting Nasogastric TubeLoveSheryNo ratings yet
- Enema 5Document22 pagesEnema 5meseretNo ratings yet
- Notes - Day 3 - MLB Class - FONDocument56 pagesNotes - Day 3 - MLB Class - FONVarsha ChudasmaNo ratings yet
- Gastric LavageDocument13 pagesGastric Lavagetibinj67No ratings yet
- Gastric LavageDocument11 pagesGastric LavageJay Villasoto100% (3)
- Management For CTD - MsDocument63 pagesManagement For CTD - MsNarz CupahanNo ratings yet
- Sarasota Memorial Hospital Nursing Procedure Title: Date: Reviewed: Pages: Issued For: ResponsibilityDocument5 pagesSarasota Memorial Hospital Nursing Procedure Title: Date: Reviewed: Pages: Issued For: Responsibilitybalab2311No ratings yet
- Enema AdministrationDocument37 pagesEnema Administrationapi-3722454100% (6)
- Water Sael DrainageDocument36 pagesWater Sael DrainageerlinaNo ratings yet
- Nursing Care For Clients With Chest TubeDocument21 pagesNursing Care For Clients With Chest TubeKayeNo ratings yet
- Nasogastric TubeDocument25 pagesNasogastric Tubekayse abtidoonNo ratings yet
- Chest DrainageDocument28 pagesChest DrainageCristy Guzman100% (1)
- Abdominal ParacentesisDocument4 pagesAbdominal Paracentesisgurneet kourNo ratings yet
- Nursing Managment of Chest Tubes: by Alice Leung RN, BSN, PCCNDocument55 pagesNursing Managment of Chest Tubes: by Alice Leung RN, BSN, PCCNFrancis Xavier S. Mendez0% (1)
- Nasogastric Intubation: DR - Efman.E.U.Manawan Mkes.,Spb-KbdDocument32 pagesNasogastric Intubation: DR - Efman.E.U.Manawan Mkes.,Spb-KbdBilly PeterNo ratings yet
- NG Tube IntubationDocument40 pagesNG Tube IntubationVed BratNo ratings yet
- Fundamentals of NursingDocument42 pagesFundamentals of NursingFrancis James RigodonNo ratings yet
- NGT Insertion 2022Document41 pagesNGT Insertion 2022Krishna Faith P. DelaraNo ratings yet
- Bladder Irrigation (Cystoclysis)Document4 pagesBladder Irrigation (Cystoclysis)CJ Angeles100% (2)
- Activity and Case Study RF and RCMDocument2 pagesActivity and Case Study RF and RCMJarda julie DacuagNo ratings yet
- Providing Special CareDocument23 pagesProviding Special CareJan LagriaNo ratings yet
- Nasogastric Tube Insertion and FeedingDocument8 pagesNasogastric Tube Insertion and FeedingHiba V.ANo ratings yet
- Inserting A Nasogastric TubeDocument5 pagesInserting A Nasogastric TubeWendy EscalanteNo ratings yet
- NG and Foley Cath M2 2009Document54 pagesNG and Foley Cath M2 2009aditi268100% (1)
- Module 3 Nursing Skills Procedure On GI, Endo-Metab Concept (A)Document18 pagesModule 3 Nursing Skills Procedure On GI, Endo-Metab Concept (A)Nashebah A. BatuganNo ratings yet
- Iv PrimingDocument16 pagesIv PrimingZahra jane A.No ratings yet
- NG Tube InsertionDocument37 pagesNG Tube InsertionSarah BirechNo ratings yet
- Administering Tube FeedingsDocument48 pagesAdministering Tube FeedingsJan Federick BantayNo ratings yet
- Tracheostomy Suctioning SkillDocument6 pagesTracheostomy Suctioning Skill3thanKimNo ratings yet
- Care of Clients With Chest TubeDocument55 pagesCare of Clients With Chest TubeMarc Andreo MalalaNo ratings yet
- Suture MaterialsDocument42 pagesSuture MaterialsAmirudin SanipNo ratings yet
- Chest Tube, Urinary Catheter, Ryles Tube InsertionDocument60 pagesChest Tube, Urinary Catheter, Ryles Tube InsertionMohd Johari Mohd ShafuwanNo ratings yet
- Tracheostomy SlidesDocument24 pagesTracheostomy SlidesMohammed AdamNo ratings yet
- CTT ClaireDocument74 pagesCTT ClaireEmma IntiaNo ratings yet
- Fundamental Nsg-IiDocument46 pagesFundamental Nsg-IiabiyotNo ratings yet
- PARACENTESISDocument15 pagesPARACENTESISSoonh ChannaNo ratings yet
- CH 2 SuctioningDocument90 pagesCH 2 SuctioningMaherNo ratings yet
- Administration of An Enema: Prepared By: Salwa MaghrabiDocument16 pagesAdministration of An Enema: Prepared By: Salwa MaghrabiAnonymous 1EoKWlNo ratings yet
- Lect 8 SUTUREDocument33 pagesLect 8 SUTUREAbdisamed AllaaleNo ratings yet
- Nutrition: Procedure GuidelinesDocument33 pagesNutrition: Procedure GuidelinesAhmad SobihNo ratings yet
- Urology Case 10th March 2024Document35 pagesUrology Case 10th March 2024tamzidshafi78No ratings yet
- Assisting in Nasogastric Tube InsertionDocument11 pagesAssisting in Nasogastric Tube InsertionJan Federick BantayNo ratings yet
- Intercostal Tube Insertion: Dr. Uttpal DesaiDocument16 pagesIntercostal Tube Insertion: Dr. Uttpal DesaiMSc. PreviousNo ratings yet
- Rules and Directions for the Employment of Injections in Various DiseasesFrom EverandRules and Directions for the Employment of Injections in Various DiseasesNo ratings yet
- Transdermal Drug Delivery System1Document38 pagesTransdermal Drug Delivery System1shobhitNo ratings yet
- FonologiajapaneseDocument283 pagesFonologiajapanesepepegrillo100% (1)
- Tamez-Freedom in Paul and HayekDocument10 pagesTamez-Freedom in Paul and HayekRyan HayesNo ratings yet
- Lee - Chinese People's Diplomacy and Developmental Relations With East Asia - Trends in The Xi Jinping Era-Routledge (2020)Document181 pagesLee - Chinese People's Diplomacy and Developmental Relations With East Asia - Trends in The Xi Jinping Era-Routledge (2020)Ralph Romulus FrondozaNo ratings yet
- Prevod: Treacherous, I Didn't Ever Believe You'd Put Yourself Into This Sort of Squalid MuddleDocument17 pagesPrevod: Treacherous, I Didn't Ever Believe You'd Put Yourself Into This Sort of Squalid MuddleMarina TanovićNo ratings yet
- Golden Root Complex Review: Does Golden Root Complex Work?Document2 pagesGolden Root Complex Review: Does Golden Root Complex Work?lleejohn85% (13)
- Categorizations of Behavioral BiasesDocument9 pagesCategorizations of Behavioral BiasesKartikay GoswamiNo ratings yet
- NITIE DGMP-3 BrochureDocument28 pagesNITIE DGMP-3 BrochureAmrut GodboleNo ratings yet
- ExerciseDocument9 pagesExercisegundadanNo ratings yet
- Kelsey - 700 Places To Volunteer Before You DieDocument534 pagesKelsey - 700 Places To Volunteer Before You DieCecilia M100% (3)
- Digital Signal Processor Based Vbyf Control of Speed of Induction MotorDocument24 pagesDigital Signal Processor Based Vbyf Control of Speed of Induction MotorManu JainNo ratings yet
- Rotenberg, The Metropolis and Everyday LifeDocument9 pagesRotenberg, The Metropolis and Everyday LifeAngie Tatiana Camelo BautistaNo ratings yet
- Assessing Students' Reading Comprehension Through Rubrics1 PDFDocument5 pagesAssessing Students' Reading Comprehension Through Rubrics1 PDFDetox MarmanNo ratings yet
- The Effect of Oral Care With Chlorhexidine PDFDocument7 pagesThe Effect of Oral Care With Chlorhexidine PDFALISSON DAYAN CHICA HERRERANo ratings yet
- Brigada Dos and DontsDocument15 pagesBrigada Dos and DontsNoel PolaronNo ratings yet
- 1 - Financial Report Analysis v.5Document55 pages1 - Financial Report Analysis v.5Joi Pia Sison SantosNo ratings yet
- Open Society Barometer Can Democracy Deliver 20230911Document48 pagesOpen Society Barometer Can Democracy Deliver 20230911yosue7dNo ratings yet
- An Illustrated Guide To Arthur Danto's - The End of ArtDocument14 pagesAn Illustrated Guide To Arthur Danto's - The End of ArtAnderson BogéaNo ratings yet
- Rezumat Scurt Teza BaitelDocument12 pagesRezumat Scurt Teza BaitelBaitel IrinaNo ratings yet
- Pol. Sci. Ch-3 Electoral Politics WorksheetDocument3 pagesPol. Sci. Ch-3 Electoral Politics WorksheetSiddhant NarayanNo ratings yet
- 正宗的维多利亚时代模板设计Document68 pages正宗的维多利亚时代模板设计Hen Lau100% (1)
- Gre Arch&Landsc Catalogue2013Document98 pagesGre Arch&Landsc Catalogue2013Gre_Architecture0% (2)
- Instructions For Seminar PaperDocument2 pagesInstructions For Seminar PaperSelmir LjevakovićNo ratings yet
- Targa ControllingrunoutDocument2 pagesTarga Controllingrunoutsaleempasha24No ratings yet
- Goli InfluencerTalkingPoints 20201106-USDocument5 pagesGoli InfluencerTalkingPoints 20201106-USOnline StoreNo ratings yet
- Humour in Advertising ThesisDocument7 pagesHumour in Advertising Thesissprxzfugg100% (1)
- Ingles Prueba PracticaDocument5 pagesIngles Prueba PracticaNoa SauraNo ratings yet
- Speech Writing and Delivery RubricDocument2 pagesSpeech Writing and Delivery RubricKrezia Erica CorpinNo ratings yet
- Performance Evaluation of Parallel ComputersDocument37 pagesPerformance Evaluation of Parallel Computersswapnil dwivediNo ratings yet
- Compare and Contrast Essay Assignment Week 4 Coronavirus Versus Influenza GHead8538Document5 pagesCompare and Contrast Essay Assignment Week 4 Coronavirus Versus Influenza GHead8538iqbaloktavianNo ratings yet






















































































Download as doc, pdf, or txt
You might also like
- Surgery OsceDocument69 pagesSurgery OsceRebecca BrandonNo ratings yet
- Water Seal DrainageDocument6 pagesWater Seal DrainageAmit MartinNo ratings yet
- .archNG - Parenteral NutritionDocument77 pages.archNG - Parenteral NutritionBidhya GuptaNo ratings yet
- Objectives: at The End of The Discussion The Students Will Be Able ToDocument6 pagesObjectives: at The End of The Discussion The Students Will Be Able ToMichael Angelo SeñaNo ratings yet
- Ryle's Tube (Nasogastric Tube)Document41 pagesRyle's Tube (Nasogastric Tube)Sandhya BasnetNo ratings yet
- Chest IntubationDocument42 pagesChest IntubationdrusmanjamilhcmdNo ratings yet
- Nasogastric Intubation: DR - Efman.E.U.Manawan Mkes.,Spb-KbdDocument32 pagesNasogastric Intubation: DR - Efman.E.U.Manawan Mkes.,Spb-KbdNur Ilmi SofiahNo ratings yet
- Nursing Procedures 2003Document11 pagesNursing Procedures 2003jackson2494100% (1)
- NG Tube Lictures 2023Document22 pagesNG Tube Lictures 2023ALi NursingNo ratings yet
- Objectives: Intestinal Tube InsertionDocument28 pagesObjectives: Intestinal Tube Insertion2013SecBNo ratings yet
- Nasogastric Tube NGT 1215082454278959 8Document107 pagesNasogastric Tube NGT 1215082454278959 8Raquel M. MendozaNo ratings yet
- Common Respiratory InterventionsDocument10 pagesCommon Respiratory InterventionsAngel Joy CatalanNo ratings yet
- Administering An EnemaDocument17 pagesAdministering An EnemaAngela Faye CallejaNo ratings yet
- Care of Patient With: Chest DrainageDocument29 pagesCare of Patient With: Chest DrainageMSc. PreviousNo ratings yet
- Group 2 - Rose & Sadava - Chest Tube InsertionDocument19 pagesGroup 2 - Rose & Sadava - Chest Tube InsertionRay Anthony RoseNo ratings yet
- Inserting Nasogastric TubeDocument4 pagesInserting Nasogastric TubeLoveSheryNo ratings yet
- Enema 5Document22 pagesEnema 5meseretNo ratings yet
- Notes - Day 3 - MLB Class - FONDocument56 pagesNotes - Day 3 - MLB Class - FONVarsha ChudasmaNo ratings yet
- Gastric LavageDocument13 pagesGastric Lavagetibinj67No ratings yet
- Gastric LavageDocument11 pagesGastric LavageJay Villasoto100% (3)
- Management For CTD - MsDocument63 pagesManagement For CTD - MsNarz CupahanNo ratings yet
- Sarasota Memorial Hospital Nursing Procedure Title: Date: Reviewed: Pages: Issued For: ResponsibilityDocument5 pagesSarasota Memorial Hospital Nursing Procedure Title: Date: Reviewed: Pages: Issued For: Responsibilitybalab2311No ratings yet
- Enema AdministrationDocument37 pagesEnema Administrationapi-3722454100% (6)
- Water Sael DrainageDocument36 pagesWater Sael DrainageerlinaNo ratings yet
- Nursing Care For Clients With Chest TubeDocument21 pagesNursing Care For Clients With Chest TubeKayeNo ratings yet
- Nasogastric TubeDocument25 pagesNasogastric Tubekayse abtidoonNo ratings yet
- Chest DrainageDocument28 pagesChest DrainageCristy Guzman100% (1)
- Abdominal ParacentesisDocument4 pagesAbdominal Paracentesisgurneet kourNo ratings yet
- Nursing Managment of Chest Tubes: by Alice Leung RN, BSN, PCCNDocument55 pagesNursing Managment of Chest Tubes: by Alice Leung RN, BSN, PCCNFrancis Xavier S. Mendez0% (1)
- Nasogastric Intubation: DR - Efman.E.U.Manawan Mkes.,Spb-KbdDocument32 pagesNasogastric Intubation: DR - Efman.E.U.Manawan Mkes.,Spb-KbdBilly PeterNo ratings yet
- NG Tube IntubationDocument40 pagesNG Tube IntubationVed BratNo ratings yet
- Fundamentals of NursingDocument42 pagesFundamentals of NursingFrancis James RigodonNo ratings yet
- NGT Insertion 2022Document41 pagesNGT Insertion 2022Krishna Faith P. DelaraNo ratings yet
- Bladder Irrigation (Cystoclysis)Document4 pagesBladder Irrigation (Cystoclysis)CJ Angeles100% (2)
- Activity and Case Study RF and RCMDocument2 pagesActivity and Case Study RF and RCMJarda julie DacuagNo ratings yet
- Providing Special CareDocument23 pagesProviding Special CareJan LagriaNo ratings yet
- Nasogastric Tube Insertion and FeedingDocument8 pagesNasogastric Tube Insertion and FeedingHiba V.ANo ratings yet
- Inserting A Nasogastric TubeDocument5 pagesInserting A Nasogastric TubeWendy EscalanteNo ratings yet
- NG and Foley Cath M2 2009Document54 pagesNG and Foley Cath M2 2009aditi268100% (1)
- Module 3 Nursing Skills Procedure On GI, Endo-Metab Concept (A)Document18 pagesModule 3 Nursing Skills Procedure On GI, Endo-Metab Concept (A)Nashebah A. BatuganNo ratings yet
- Iv PrimingDocument16 pagesIv PrimingZahra jane A.No ratings yet
- NG Tube InsertionDocument37 pagesNG Tube InsertionSarah BirechNo ratings yet
- Administering Tube FeedingsDocument48 pagesAdministering Tube FeedingsJan Federick BantayNo ratings yet
- Tracheostomy Suctioning SkillDocument6 pagesTracheostomy Suctioning Skill3thanKimNo ratings yet
- Care of Clients With Chest TubeDocument55 pagesCare of Clients With Chest TubeMarc Andreo MalalaNo ratings yet
- Suture MaterialsDocument42 pagesSuture MaterialsAmirudin SanipNo ratings yet
- Chest Tube, Urinary Catheter, Ryles Tube InsertionDocument60 pagesChest Tube, Urinary Catheter, Ryles Tube InsertionMohd Johari Mohd ShafuwanNo ratings yet
- Tracheostomy SlidesDocument24 pagesTracheostomy SlidesMohammed AdamNo ratings yet
- CTT ClaireDocument74 pagesCTT ClaireEmma IntiaNo ratings yet
- Fundamental Nsg-IiDocument46 pagesFundamental Nsg-IiabiyotNo ratings yet
- PARACENTESISDocument15 pagesPARACENTESISSoonh ChannaNo ratings yet
- CH 2 SuctioningDocument90 pagesCH 2 SuctioningMaherNo ratings yet
- Administration of An Enema: Prepared By: Salwa MaghrabiDocument16 pagesAdministration of An Enema: Prepared By: Salwa MaghrabiAnonymous 1EoKWlNo ratings yet
- Lect 8 SUTUREDocument33 pagesLect 8 SUTUREAbdisamed AllaaleNo ratings yet
- Nutrition: Procedure GuidelinesDocument33 pagesNutrition: Procedure GuidelinesAhmad SobihNo ratings yet
- Urology Case 10th March 2024Document35 pagesUrology Case 10th March 2024tamzidshafi78No ratings yet
- Assisting in Nasogastric Tube InsertionDocument11 pagesAssisting in Nasogastric Tube InsertionJan Federick BantayNo ratings yet
- Intercostal Tube Insertion: Dr. Uttpal DesaiDocument16 pagesIntercostal Tube Insertion: Dr. Uttpal DesaiMSc. PreviousNo ratings yet
- Rules and Directions for the Employment of Injections in Various DiseasesFrom EverandRules and Directions for the Employment of Injections in Various DiseasesNo ratings yet
- Transdermal Drug Delivery System1Document38 pagesTransdermal Drug Delivery System1shobhitNo ratings yet
- FonologiajapaneseDocument283 pagesFonologiajapanesepepegrillo100% (1)
- Tamez-Freedom in Paul and HayekDocument10 pagesTamez-Freedom in Paul and HayekRyan HayesNo ratings yet
- Lee - Chinese People's Diplomacy and Developmental Relations With East Asia - Trends in The Xi Jinping Era-Routledge (2020)Document181 pagesLee - Chinese People's Diplomacy and Developmental Relations With East Asia - Trends in The Xi Jinping Era-Routledge (2020)Ralph Romulus FrondozaNo ratings yet
- Prevod: Treacherous, I Didn't Ever Believe You'd Put Yourself Into This Sort of Squalid MuddleDocument17 pagesPrevod: Treacherous, I Didn't Ever Believe You'd Put Yourself Into This Sort of Squalid MuddleMarina TanovićNo ratings yet
- Golden Root Complex Review: Does Golden Root Complex Work?Document2 pagesGolden Root Complex Review: Does Golden Root Complex Work?lleejohn85% (13)
- Categorizations of Behavioral BiasesDocument9 pagesCategorizations of Behavioral BiasesKartikay GoswamiNo ratings yet
- NITIE DGMP-3 BrochureDocument28 pagesNITIE DGMP-3 BrochureAmrut GodboleNo ratings yet
- ExerciseDocument9 pagesExercisegundadanNo ratings yet
- Kelsey - 700 Places To Volunteer Before You DieDocument534 pagesKelsey - 700 Places To Volunteer Before You DieCecilia M100% (3)
- Digital Signal Processor Based Vbyf Control of Speed of Induction MotorDocument24 pagesDigital Signal Processor Based Vbyf Control of Speed of Induction MotorManu JainNo ratings yet
- Rotenberg, The Metropolis and Everyday LifeDocument9 pagesRotenberg, The Metropolis and Everyday LifeAngie Tatiana Camelo BautistaNo ratings yet
- Assessing Students' Reading Comprehension Through Rubrics1 PDFDocument5 pagesAssessing Students' Reading Comprehension Through Rubrics1 PDFDetox MarmanNo ratings yet
- The Effect of Oral Care With Chlorhexidine PDFDocument7 pagesThe Effect of Oral Care With Chlorhexidine PDFALISSON DAYAN CHICA HERRERANo ratings yet
- Brigada Dos and DontsDocument15 pagesBrigada Dos and DontsNoel PolaronNo ratings yet
- 1 - Financial Report Analysis v.5Document55 pages1 - Financial Report Analysis v.5Joi Pia Sison SantosNo ratings yet
- Open Society Barometer Can Democracy Deliver 20230911Document48 pagesOpen Society Barometer Can Democracy Deliver 20230911yosue7dNo ratings yet
- An Illustrated Guide To Arthur Danto's - The End of ArtDocument14 pagesAn Illustrated Guide To Arthur Danto's - The End of ArtAnderson BogéaNo ratings yet
- Rezumat Scurt Teza BaitelDocument12 pagesRezumat Scurt Teza BaitelBaitel IrinaNo ratings yet
- Pol. Sci. Ch-3 Electoral Politics WorksheetDocument3 pagesPol. Sci. Ch-3 Electoral Politics WorksheetSiddhant NarayanNo ratings yet
- 正宗的维多利亚时代模板设计Document68 pages正宗的维多利亚时代模板设计Hen Lau100% (1)
- Gre Arch&Landsc Catalogue2013Document98 pagesGre Arch&Landsc Catalogue2013Gre_Architecture0% (2)
- Instructions For Seminar PaperDocument2 pagesInstructions For Seminar PaperSelmir LjevakovićNo ratings yet
- Targa ControllingrunoutDocument2 pagesTarga Controllingrunoutsaleempasha24No ratings yet
- Goli InfluencerTalkingPoints 20201106-USDocument5 pagesGoli InfluencerTalkingPoints 20201106-USOnline StoreNo ratings yet
- Humour in Advertising ThesisDocument7 pagesHumour in Advertising Thesissprxzfugg100% (1)
- Ingles Prueba PracticaDocument5 pagesIngles Prueba PracticaNoa SauraNo ratings yet
- Speech Writing and Delivery RubricDocument2 pagesSpeech Writing and Delivery RubricKrezia Erica CorpinNo ratings yet
- Performance Evaluation of Parallel ComputersDocument37 pagesPerformance Evaluation of Parallel Computersswapnil dwivediNo ratings yet
- Compare and Contrast Essay Assignment Week 4 Coronavirus Versus Influenza GHead8538Document5 pagesCompare and Contrast Essay Assignment Week 4 Coronavirus Versus Influenza GHead8538iqbaloktavianNo ratings yet