Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5825)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Meconium Aspiration Syndrome Case PresentationDocument26 pagesMeconium Aspiration Syndrome Case Presentationkis100% (2)
- Aseptic Technique Lab ReportDocument7 pagesAseptic Technique Lab ReportEugenTutunaru100% (2)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Testosterone A Mans Guide Second EditionDocument204 pagesTestosterone A Mans Guide Second EditionMatteo Panciroli100% (3)
- Canna DispensariesDocument35 pagesCanna DispensariesWaf Etano100% (1)
- CXR ABC by DR ShamolDocument139 pagesCXR ABC by DR Shamolazar103100% (3)
- FT Ethno-Healing Practices & Medical Beliefs of Folk Healers in Bongao, Tawi-TawiDocument91 pagesFT Ethno-Healing Practices & Medical Beliefs of Folk Healers in Bongao, Tawi-TawiAnonymous IVn5yBbv50% (2)
- Urschel - How To AnalyzeDocument4 pagesUrschel - How To Analyzek1988No ratings yet
- TNSOP 6 Clinical GuidelinesDocument14 pagesTNSOP 6 Clinical Guidelinesazar103No ratings yet
- COVID - English Final PDFDocument2 pagesCOVID - English Final PDFazar103No ratings yet
- TNSOP 2 Sample Collection PDFDocument4 pagesTNSOP 2 Sample Collection PDFazar103No ratings yet
- Contact Follow Up: Identify Contacts of Lab Confirmed COVID-19 Patients by District EOC (Use FORM 3A)Document1 pageContact Follow Up: Identify Contacts of Lab Confirmed COVID-19 Patients by District EOC (Use FORM 3A)azar103No ratings yet
- TNSOP 4 Home Care PDFDocument1 pageTNSOP 4 Home Care PDFazar103No ratings yet
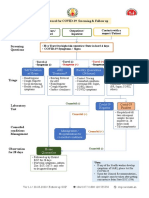
- Protocol For COVID 19 Screening and Followup PDFDocument1 pageProtocol For COVID 19 Screening and Followup PDFazar103No ratings yet
- Clinical Refraction QuizDocument3 pagesClinical Refraction QuizLLido Cathyrine S.No ratings yet
- Gpat-Niper Topics-BookwiseDocument11 pagesGpat-Niper Topics-Bookwiseapi-230055654No ratings yet
- CAE Use of EnglishDocument10 pagesCAE Use of Englishali_nusNo ratings yet
- Critical Aprraisal DR - Cholis Nur Mutaslimah MPHDocument16 pagesCritical Aprraisal DR - Cholis Nur Mutaslimah MPHAyashaa BelleNo ratings yet
- Go Meta To Change Your Personal HistoryDocument3 pagesGo Meta To Change Your Personal HistoryKANGKURUNo ratings yet
- Abdominal MassDocument5 pagesAbdominal MassArthana PutraNo ratings yet
- Attention Ce Tableau Indique Les Présentations Disponibles Dans Les Chariots de Réa Du DEA Et Au Box 10 Du SAUP Uniquement !Document1 pageAttention Ce Tableau Indique Les Présentations Disponibles Dans Les Chariots de Réa Du DEA Et Au Box 10 Du SAUP Uniquement !mihalcea alinNo ratings yet
- Cow GheeDocument4 pagesCow Gheeamol_raoNo ratings yet
- Patient Satisfaction SurveyDocument3 pagesPatient Satisfaction SurveyGlady Jane Teves0% (1)
- Ba Duan JinDocument5 pagesBa Duan JinpenfoNo ratings yet
- Psychiatric Nursing Practice Test IDocument19 pagesPsychiatric Nursing Practice Test Igirl_fenolNo ratings yet
- FDA - ICH M7 (R1) - Control of Mutagenic Impurities in Pharmaceuticals 03.2018Document131 pagesFDA - ICH M7 (R1) - Control of Mutagenic Impurities in Pharmaceuticals 03.2018Catrinescu OanaNo ratings yet
- Lesson 1: Overview and Principles of Resuscitation: Neonatal Resuscitation Program Slide Presentation KitDocument32 pagesLesson 1: Overview and Principles of Resuscitation: Neonatal Resuscitation Program Slide Presentation KitChauthiran AgamudaiyarNo ratings yet
- Sop Mouse Injection SubcutaneousDocument4 pagesSop Mouse Injection SubcutaneousAmalia WardatulNo ratings yet
- Aversive ConditioningDocument4 pagesAversive Conditioningiulia9gavrisNo ratings yet
- Contoh Morning ReportDocument23 pagesContoh Morning ReportDaondy Friarsa SoehartoNo ratings yet
- ReflDocument5 pagesReflEdmar ReyesNo ratings yet
- AP Psychology Forest Grove High School Mr. TusowDocument81 pagesAP Psychology Forest Grove High School Mr. TusowIsabella TNo ratings yet
- Ocular Response Analyzer BrochureDocument6 pagesOcular Response Analyzer BrochureLotte Lotte BalotNo ratings yet
- Buy Crystal Methamphetamine OnlineDocument7 pagesBuy Crystal Methamphetamine Onlinezoe saldana100% (1)
- Template Diglap LplpoDocument12 pagesTemplate Diglap LplpoNurul Elisa 'cHa'No ratings yet
- Final EditedDocument40 pagesFinal Editednikita takiarNo ratings yet
- Rizal Provincial Hospital Ok NaDocument51 pagesRizal Provincial Hospital Ok NaNURSETOPNOTCHER100% (1)
- Lesinurad For The Treatment of Hyperuricaemia in People With GoutDocument24 pagesLesinurad For The Treatment of Hyperuricaemia in People With GoutPharmaEducationNo ratings yet