Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- PD Gyne ReviewerDocument2 pagesPD Gyne ReviewerKristine Boholst100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 14-15 Peds Key Word Analysis NbomeDocument3 pages14-15 Peds Key Word Analysis NbomeChris Dubuque0% (1)
- MCQs For Prometric Examination PDFDocument155 pagesMCQs For Prometric Examination PDFYacine Tarik AizelNo ratings yet
- Best Evidence Statement (Best) : DefinitionsDocument6 pagesBest Evidence Statement (Best) : DefinitionsFungky AnthonyNo ratings yet
- AnxietyDocument3 pagesAnxietyFungky AnthonyNo ratings yet
- Infant Formula: NINA R. O'CONNOR, MD, Chestnut Hill Family Practice Residency, Philadelphia, PennslyvaniaDocument6 pagesInfant Formula: NINA R. O'CONNOR, MD, Chestnut Hill Family Practice Residency, Philadelphia, PennslyvaniaFungky AnthonyNo ratings yet
- Drug Safety AlertDocument92 pagesDrug Safety AlertFungky AnthonyNo ratings yet
- Bab 4 Capaian Rs NovDocument14 pagesBab 4 Capaian Rs NovInggrid MonicaNo ratings yet
- Signs and Symptoms: Wart Bottom Foot Toes SkinDocument3 pagesSigns and Symptoms: Wart Bottom Foot Toes SkinIana CovaliovNo ratings yet
- Abstract Comparison Between Albendazole and MebendazoleDocument25 pagesAbstract Comparison Between Albendazole and MebendazoleluzNo ratings yet
- Pertussis: PDF, 667kbDocument2 pagesPertussis: PDF, 667kbRaissa DeaNo ratings yet
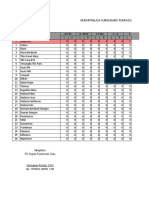
- Rekapitulasi 20 Besar Kunjungan Pasien PuskesmasDocument1 pageRekapitulasi 20 Besar Kunjungan Pasien Puskesmasghaniangga11No ratings yet
- Dios Tu Solamente Es Dios AutosavedDocument531 pagesDios Tu Solamente Es Dios AutosavedIan LimNo ratings yet
- Hirschsprung DiseaseDocument14 pagesHirschsprung DiseaseFlordelyn Anuales100% (2)
- TCL For Nutrition & Epi Program Part 1Document23 pagesTCL For Nutrition & Epi Program Part 1Johnmark DubdubanNo ratings yet
- Diarrhea: See Complete List of ChartsDocument4 pagesDiarrhea: See Complete List of ChartsIndera Noor AchmadNo ratings yet
- Dysfunctional Labor As One of The Intrapartal ComplicationsDocument23 pagesDysfunctional Labor As One of The Intrapartal ComplicationsKenje Kate AgripoNo ratings yet
- Kode IcdDocument4 pagesKode IcdhanapiahNo ratings yet
- The Urine FEME Turn Out To Be Positive On Nitrite and Leucocyte 4+Document12 pagesThe Urine FEME Turn Out To Be Positive On Nitrite and Leucocyte 4+navenNo ratings yet
- List Produk PT - MBS (September)Document94 pagesList Produk PT - MBS (September)clara shinta dilapanga50% (2)
- Pathophysiology and Etiology of Sudden Cardiac Arrest: Author: Section Editors: Deputy EditorDocument23 pagesPathophysiology and Etiology of Sudden Cardiac Arrest: Author: Section Editors: Deputy EditorAnca StanNo ratings yet
- Daftar Obat "High Alert" (Termasuk Lasa & Elektrolit Konsentrat) - Lakukan Double CheckDocument2 pagesDaftar Obat "High Alert" (Termasuk Lasa & Elektrolit Konsentrat) - Lakukan Double CheckBenk Nurhidayat SusiloNo ratings yet
- Laporan Bulanan Rekapitulasi Surveilans Terpadu Penyakit (STP) Baru Di Puskesmas Dan Jejaringnya Puskesmas SoliuDocument37 pagesLaporan Bulanan Rekapitulasi Surveilans Terpadu Penyakit (STP) Baru Di Puskesmas Dan Jejaringnya Puskesmas SoliuVictoria YanersNo ratings yet
- Citra Farm Hungary PDFDocument22 pagesCitra Farm Hungary PDFvdvedNo ratings yet
- Maternity Newborn Diagnoses ICD-9 To ICD-10-CM Code TranslationDocument3 pagesMaternity Newborn Diagnoses ICD-9 To ICD-10-CM Code TranslationNathanael ReyesNo ratings yet
- Ca1 Nursing Care Management 102Document8 pagesCa1 Nursing Care Management 102raul nino MoranNo ratings yet
- Common Parasites and Diseases of ManDocument14 pagesCommon Parasites and Diseases of Manpramodrp2007No ratings yet
- Case Presentation of Acute PyelonephritisDocument1 pageCase Presentation of Acute PyelonephritisANALYN ANUBNo ratings yet
- Drug Study IbuprofenDocument2 pagesDrug Study Ibuprofendawnscribd80% (5)
- Divine Healing Codes and How To Use Them: Friday, June 13, 2014Document32 pagesDivine Healing Codes and How To Use Them: Friday, June 13, 2014Dheeraj KumarNo ratings yet
- GastritisDocument10 pagesGastritisEka Puspa100% (1)
- Adenoviridae & Papovaviridae: R. Lia K. Iswara, DR, MS, SPMK Dept. Microbiology FK UsuDocument16 pagesAdenoviridae & Papovaviridae: R. Lia K. Iswara, DR, MS, SPMK Dept. Microbiology FK UsuMuhammad AslamNo ratings yet
- Pediatrics QuestionsDocument3 pagesPediatrics QuestionssparkleNo ratings yet
- IST's - HPVDocument17 pagesIST's - HPVCaio BarbosaNo ratings yet