Download as doc, pdf, or txt
You might also like
- Occupational Therapy Assessments Quick TableDocument5 pagesOccupational Therapy Assessments Quick Tableredsmartie100% (3)
- Training Design MatrixDocument6 pagesTraining Design Matrixflorlijosol100% (2)
- Passmedicine Mcqs-Surgical and Musculoskeletal ProblemsDocument346 pagesPassmedicine Mcqs-Surgical and Musculoskeletal ProblemsMohammad Saleh100% (1)
- Jadwal Pelatihan BtclsDocument6 pagesJadwal Pelatihan BtclsManuriatiNo ratings yet
- Bioetik 1Document28 pagesBioetik 1Ilham AkbarNo ratings yet
- Rencana Acara Resertifikasi Pelath ICU KomprehensifDocument4 pagesRencana Acara Resertifikasi Pelath ICU KomprehensifWbNo ratings yet
- Jadwal Btcls Psik Ulm FixDocument10 pagesJadwal Btcls Psik Ulm FixHafiz RizkiNo ratings yet
- Jadwal BTCLS RS JIWA Desember 2021Document8 pagesJadwal BTCLS RS JIWA Desember 2021sinagaNo ratings yet
- Study PlanDocument19 pagesStudy PlanMuhammad Musa HaiderNo ratings yet
- MatrixDocument1 pageMatrixjaycynNo ratings yet
- Rundown AclsDocument4 pagesRundown AclsIndRa KaBhuomNo ratings yet
- Time TableDocument1 pageTime TableCybertechNo ratings yet
- 01 - Jadwal Praktikum Prakt KA 19-20Document1 page01 - Jadwal Praktikum Prakt KA 19-20Anisa FitriNo ratings yet
- Scientific Schedule InaACC 2020Document3 pagesScientific Schedule InaACC 2020Faradiba NoviandiniNo ratings yet
- Sophia Mitante Journal EntryDocument13 pagesSophia Mitante Journal EntryJeynald AmbataNo ratings yet
- Jadwal BT&CLS UNMUH PONOROGO GEL 1Document4 pagesJadwal BT&CLS UNMUH PONOROGO GEL 1Rizqi FANo ratings yet
- Jadwal Penggunaan Ruang Lab IPADocument1 pageJadwal Penggunaan Ruang Lab IPAelisabethohoilulin64No ratings yet
- PAS I Summer Block Schedule 2023 06012023Document2 pagesPAS I Summer Block Schedule 2023 06012023rosemaryma777No ratings yet
- Bataan Peninsula State UniversityDocument1 pageBataan Peninsula State Universityanon-600341100% (2)
- Jadwal Ump Ponorogo-1Document4 pagesJadwal Ump Ponorogo-1Aris nugraheniNo ratings yet
- 3rd Day Time Information InstructorDocument2 pages3rd Day Time Information InstructorBram Surya Widi GamanNo ratings yet
- ICEER 2020-ProgramDocument2 pagesICEER 2020-ProgramNidia CaetanoNo ratings yet
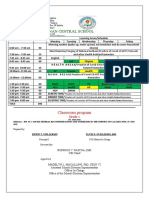
- Angadanan Central School: Classroom ProgramDocument2 pagesAngadanan Central School: Classroom ProgramHerros William Briones TorresNo ratings yet
- Simposium NeuropediatriDocument3 pagesSimposium Neuropediatrineurologi Juli2021No ratings yet
- Second Announcement Sunshine 2019Document20 pagesSecond Announcement Sunshine 2019alvinNo ratings yet
- Basic First Aid and Basic Life Support with AED Training (1)Document2 pagesBasic First Aid and Basic Life Support with AED Training (1)chotropicalunitNo ratings yet
- Basic First Aid and Basic Life Support with AED TrainingDocument2 pagesBasic First Aid and Basic Life Support with AED TrainingchotropicalunitNo ratings yet
- Monday Tuesday Wednesday Thursday Friday Saturday Sunday: Gym Gym Gym Gym GymDocument1 pageMonday Tuesday Wednesday Thursday Friday Saturday Sunday: Gym Gym Gym Gym GymCKNo ratings yet
- TRAINING MATRIX ChessDocument1 pageTRAINING MATRIX Chessaljohn esplana100% (1)
- Jadwal ACLS D' Garden Resto, PurwokertoDocument2 pagesJadwal ACLS D' Garden Resto, PurwokertoRobert HarrisNo ratings yet
- ECG Workshop Program 2024 - Irish TimesDocument2 pagesECG Workshop Program 2024 - Irish TimesAmmar AliNo ratings yet
- Jadwal Blok 22 Ked. Keluarga 2012Document6 pagesJadwal Blok 22 Ked. Keluarga 2012Arif Tantri HNo ratings yet
- BCS Study Guide Ii CoronaDocument15 pagesBCS Study Guide Ii CoronaJocelin NathanielaNo ratings yet
- Session0 Presentation UE ProgrammeDocument19 pagesSession0 Presentation UE Programmehienjuliette10No ratings yet
- Jadwal Klinik Cuti BersamaDocument1 pageJadwal Klinik Cuti BersamaandyNo ratings yet
- Booklet Bcu Revisi 5Document8 pagesBooklet Bcu Revisi 5irza nasutionNo ratings yet
- NCNW AgendaDocument1 pageNCNW Agendaapi-391188303No ratings yet
- HoraDocument2 pagesHoraYorh Espinoza RojasNo ratings yet
- Neonatal Gastric Perforation: A Single Center Experience: Observational StudyDocument6 pagesNeonatal Gastric Perforation: A Single Center Experience: Observational StudyagusNo ratings yet
- Schedule Training BTCLS Daring: Day 1 Time Subject Instructure MediaDocument3 pagesSchedule Training BTCLS Daring: Day 1 Time Subject Instructure MediaRahmad Harizky putraNo ratings yet
- 2023 2024 General Class ProgramDocument10 pages2023 2024 General Class ProgramImelda Obedoza AquinoNo ratings yet
- Rossi Pool San Francisco Hours and RatesDocument1 pageRossi Pool San Francisco Hours and Ratesiriesergio100% (6)
- Jadwal X Nkpi 1Document18 pagesJadwal X Nkpi 1RichanNo ratings yet
- Main Conference ProgrammeDocument7 pagesMain Conference ProgrammeFaadhilah HussainNo ratings yet
- Oak Park and River Forest High School: 2020-2021 Schedule Pickup WeekDocument2 pagesOak Park and River Forest High School: 2020-2021 Schedule Pickup WeekTerria OnealNo ratings yet
- 1011 Ice ScheduleDocument7 pages1011 Ice ScheduleRomach De ValletortNo ratings yet
- 3 253 3 Dds Summer Sem 2010 11Document2 pages3 253 3 Dds Summer Sem 2010 11Yi-po LiaoNo ratings yet
- Off Season Schedule 2010: BC Centre of ExcellenceDocument1 pageOff Season Schedule 2010: BC Centre of Excellenceapi-26484533No ratings yet
- Workshop BUAS ISMOAC RevisiDocument2 pagesWorkshop BUAS ISMOAC Revisibidangpengembangan123No ratings yet
- Revisi TIME TABLE FisilogiDocument6 pagesRevisi TIME TABLE FisilogibaramaNo ratings yet
- Building Learning Commitment: Hari / Tanggal Materi NarasumberDocument1 pageBuilding Learning Commitment: Hari / Tanggal Materi NarasumberVikramawardaniNo ratings yet
- Foundation Program FinalDocument15 pagesFoundation Program FinalKleven Carl GindapNo ratings yet
- Jadwal Uts Genap Pergantian JumatDocument1 pageJadwal Uts Genap Pergantian JumatDina PanjaitanNo ratings yet
- Objectives BQMH-DRDocument1 pageObjectives BQMH-DRaiera angelique LagdamenNo ratings yet
- EB Time Table 18th To 23rd March 2024Document1 pageEB Time Table 18th To 23rd March 2024Max KaleNo ratings yet
- May CalendarDocument2 pagesMay Calendarcrew_johnstonNo ratings yet
- 2011ooPediatricHandbook PDFDocument146 pages2011ooPediatricHandbook PDFSven OrdanzaNo ratings yet
- Time Table Cardiology: Da y Date Topic Learning Situation English Class Regular Class PICDocument5 pagesTime Table Cardiology: Da y Date Topic Learning Situation English Class Regular Class PICSheryl ElitaNo ratings yet
- USMLE Step I Study ScheduleDocument1 pageUSMLE Step I Study ScheduleThara Foreste-MagloireNo ratings yet
- EYC 2011 ScheduleDocument3 pagesEYC 2011 ScheduleephraimyachtclubNo ratings yet
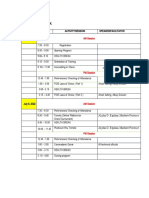
- Plan of ActivitiesDocument1 pagePlan of ActivitiesYum CNo ratings yet
- Nicu HebhkDocument44 pagesNicu HebhkEuniceSimNo ratings yet
- Csmu How: Recommended Practical Check List For Students 2010Document4 pagesCsmu How: Recommended Practical Check List For Students 2010EuniceSimNo ratings yet
- Paeds HebhkDocument8 pagesPaeds HebhkEuniceSimNo ratings yet
- Renal Control of Acid Base BalanceDocument5 pagesRenal Control of Acid Base BalanceEuniceSimNo ratings yet
- Mitral ValveDocument48 pagesMitral Valvesinghal296% (23)
- Microbiology PDFDocument237 pagesMicrobiology PDFchioNo ratings yet
- Dental Radiology: A Guide To Radiographic InterpretationDocument16 pagesDental Radiology: A Guide To Radiographic InterpretationCeline BerjotNo ratings yet
- Jurnal Hiperplasia EndometriumDocument5 pagesJurnal Hiperplasia Endometriumperussi pranadiptaNo ratings yet
- 3rd and 6th Le Coverage v1Document2 pages3rd and 6th Le Coverage v1api-257172337No ratings yet
- Chronic Kidney Diseases (CKD) - 2Document43 pagesChronic Kidney Diseases (CKD) - 2Victoria DadaNo ratings yet
- Amiodarone Atrial Fibrillation BerberinDocument10 pagesAmiodarone Atrial Fibrillation Berberinharold jitschak bueno de mesquitaNo ratings yet
- Liver, Biliary Tract and Pancreas PathologyDocument50 pagesLiver, Biliary Tract and Pancreas PathologybonadnadineNo ratings yet
- Drugs in Pregnancy: An Update: Journal of SAFOG December 2014Document6 pagesDrugs in Pregnancy: An Update: Journal of SAFOG December 2014BhefHarmoniLoveNo ratings yet
- Ankylosing SpondylitisDocument21 pagesAnkylosing SpondylitisPaul Kelner100% (2)
- Task 2 Case Notes: Brendan CrossDocument4 pagesTask 2 Case Notes: Brendan Crossprakash poudelNo ratings yet
- Zuhaib Best and Better BookDocument877 pagesZuhaib Best and Better BookabhishekNo ratings yet
- ALGLUCOSIDASE ALFA 50 MG-VIAL (Myiztme)Document2 pagesALGLUCOSIDASE ALFA 50 MG-VIAL (Myiztme)asdwasdNo ratings yet
- Complement: Kathleen Basa Kris Nicole de Guzman Jessica Mae Ong 3HmtDocument70 pagesComplement: Kathleen Basa Kris Nicole de Guzman Jessica Mae Ong 3HmtCherry Reyes-Principe100% (1)
- Informant: Grandmother (70 %) Reliability General DataDocument8 pagesInformant: Grandmother (70 %) Reliability General Dataemely p. tangoNo ratings yet
- Chapter 80 - Headache DisordersDocument41 pagesChapter 80 - Headache Disordersalina ignatNo ratings yet
- Ronco - Textbook of Cardiorenal Medicine 2021Document381 pagesRonco - Textbook of Cardiorenal Medicine 2021Adiel OjedaNo ratings yet
- Dementia & Alzheimer's Care: Planning and Preparing For The Road AheadDocument14 pagesDementia & Alzheimer's Care: Planning and Preparing For The Road AheadblurrmieNo ratings yet
- Antiphospholipid Syndrome and Pregnancy (Dengan Foto Punya DR RositaDocument9 pagesAntiphospholipid Syndrome and Pregnancy (Dengan Foto Punya DR RositadidongNo ratings yet
- Childhood Anaemia: Paediatric Haematologist and Oncologist Deparment of Paediatrics & Child Health MustDocument34 pagesChildhood Anaemia: Paediatric Haematologist and Oncologist Deparment of Paediatrics & Child Health MustSsenyonga DominicNo ratings yet
- Overview On Peripheral Artery Disease - FinalDocument78 pagesOverview On Peripheral Artery Disease - FinalMITHA100% (1)
- Cognitive Reserve and Long-Term Change in Cognition in Aging and Preclinical Alzheimer's DiseaseDocument9 pagesCognitive Reserve and Long-Term Change in Cognition in Aging and Preclinical Alzheimer's Diseasechepin ChangNo ratings yet
- Alzheimer DiseaseDocument47 pagesAlzheimer DiseaseveraveroNo ratings yet
- Sarcoidosis DR WinnieDocument33 pagesSarcoidosis DR WinniewinnieNo ratings yet
- 0002 9343 (80) 90428 3Document1 page0002 9343 (80) 90428 3Dela RismawatiNo ratings yet
- Major Intra and Extracellular IonsDocument29 pagesMajor Intra and Extracellular IonsRasel IslamNo ratings yet
- Low Back Pain Dr. Hardhi PRanataDocument57 pagesLow Back Pain Dr. Hardhi PRanataPerwita ArumingtyasNo ratings yet
- Cottenden - Wagg - Supplementary - 23551 ASW Edited Again PDFDocument74 pagesCottenden - Wagg - Supplementary - 23551 ASW Edited Again PDFrohiniNo ratings yet