Download as pdf or txt
You might also like
- Toacs by ShireenDocument244 pagesToacs by ShireenMuhammad Zeeshan100% (1)
- AllofitST Surgical TechDocument16 pagesAllofitST Surgical TechAlexandru DumitrescuNo ratings yet
- Gastric Outlet ObstructionDocument9 pagesGastric Outlet ObstructionVivek AhanthemNo ratings yet
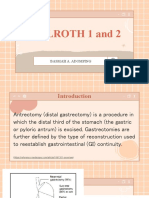
- Billroth 1 and 2: Basmah A. AdompingDocument31 pagesBillroth 1 and 2: Basmah A. AdompingBasmah A. AdompingNo ratings yet
- Enteral Stents1Document81 pagesEnteral Stents1Nikhil BhangaleNo ratings yet
- Stent in Gi DiseaseDocument18 pagesStent in Gi DiseaseAgung WidodoNo ratings yet
- Herford1998 Locking ReconstruccionDocument5 pagesHerford1998 Locking ReconstruccionAlejandra Del PilarNo ratings yet
- Dept. of Orthopaedics, KMC MangaloreDocument8 pagesDept. of Orthopaedics, KMC MangalorechinmayghaisasNo ratings yet
- 7 LaserLok 3Document20 pages7 LaserLok 3Wesam Al-SalmanNo ratings yet
- Management of d-PTFE Membrane Exposure For Having Final Clinical SuccessDocument3 pagesManagement of d-PTFE Membrane Exposure For Having Final Clinical SuccessNidia TorreaNo ratings yet
- Abutment Emergence Modification For Immediate ImplDocument6 pagesAbutment Emergence Modification For Immediate Implhkwgt7vskwNo ratings yet
- Contemporary Reviews in Interventional Cardiology: Bioabsorbable Coronary StentsDocument6 pagesContemporary Reviews in Interventional Cardiology: Bioabsorbable Coronary StentsKevin DermawanNo ratings yet
- 7 PDFDocument5 pages7 PDFRoja AllampallyNo ratings yet
- Middle Ear ImplantsDocument110 pagesMiddle Ear ImplantsRadhey SjhNo ratings yet
- Complicaciones Mini ImplantesDocument12 pagesComplicaciones Mini ImplantesNuvia PardoNo ratings yet
- Post Graduate Student: Dr. RahultiwariDocument158 pagesPost Graduate Student: Dr. RahultiwariVivek Sunil EdayathNo ratings yet
- Ic Rehabilitation of The Edentulous Patient Maxillectomy UiriDocument5 pagesIc Rehabilitation of The Edentulous Patient Maxillectomy Uiriayush srivastavaNo ratings yet
- ImplantDocument9 pagesImplantKhaled Abo ZaidNo ratings yet
- DeBoever 2001 TMD and RehabDocument4 pagesDeBoever 2001 TMD and RehabstercostasNo ratings yet
- Occlusal Considerations For Implant-Supported Prostheses - Implant-Protective OcclusionDocument39 pagesOcclusal Considerations For Implant-Supported Prostheses - Implant-Protective Occlusionandrea.lopp.paNo ratings yet
- Role of Mini-Implants in OrthodonticsDocument9 pagesRole of Mini-Implants in OrthodonticsRonald WilfredNo ratings yet
- Femoro-Acetabular Impingement. ClassificDocument10 pagesFemoro-Acetabular Impingement. ClassificPriscilla PriscillaNo ratings yet
- Dental ImplantsDocument6 pagesDental ImplantsSophia MolinaNo ratings yet
- An Esthetic Solution to the Screw-Retained Implant Restoration Introduction to the Implant Crown Adhesive Plug Clinical Docslide.us_an-esthetic-solution-To-The-screw-retained-implant-restoration-IntroductionDocument6 pagesAn Esthetic Solution to the Screw-Retained Implant Restoration Introduction to the Implant Crown Adhesive Plug Clinical Docslide.us_an-esthetic-solution-To-The-screw-retained-implant-restoration-IntroductionZahraDent EasyGrip Tfi ImplantNo ratings yet
- Wallflexbiliary Productinfo Brochure PDFDocument6 pagesWallflexbiliary Productinfo Brochure PDFhoneyworksNo ratings yet
- Analysis of 356 Pterygomaxillary Implants - Balshi Et AlDocument9 pagesAnalysis of 356 Pterygomaxillary Implants - Balshi Et AlNiaz AhammedNo ratings yet
- Zygoma ImplantDocument63 pagesZygoma ImplantKristina Robles100% (2)
- Tads - KomalDocument100 pagesTads - KomalRohini TondaNo ratings yet
- Silicone Suspension of External Prostheses: From The Chaim Sheba Medical Centre, Tel Hashomer, IsraelDocument3 pagesSilicone Suspension of External Prostheses: From The Chaim Sheba Medical Centre, Tel Hashomer, IsraelMohammad RezaNo ratings yet
- Ehlinger (2010)Document6 pagesEhlinger (2010)TommysNo ratings yet
- Maxillary Major ConnectorsDocument14 pagesMaxillary Major ConnectorsHiba SaadNo ratings yet
- Airway StentingDocument6 pagesAirway StentingROHAN BHATTNo ratings yet
- Abutment Selection For Anterior Implant-Supported RestorationsDocument5 pagesAbutment Selection For Anterior Implant-Supported RestorationsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Periodontology 2000 - 2022 - Sailer - Prosthetic Failures in Dental Implant TherapyDocument15 pagesPeriodontology 2000 - 2022 - Sailer - Prosthetic Failures in Dental Implant TherapyAndrea KauffmerNo ratings yet
- Tissue Preservation and Maintenance of Optimum Esthetics: A Clinical ReportDocument7 pagesTissue Preservation and Maintenance of Optimum Esthetics: A Clinical ReportBagis Emre GulNo ratings yet
- A Novel Technique For The Removal of Cementless Large Diameter MOM Acetabulum TIPDocument3 pagesA Novel Technique For The Removal of Cementless Large Diameter MOM Acetabulum TIPana starcevicNo ratings yet
- Nasal Stents Are They Really Useful ?Document9 pagesNasal Stents Are They Really Useful ?Dr. T. BalasubramanianNo ratings yet
- Pi Is 0889540615013311Document5 pagesPi Is 0889540615013311msoaresmirandaNo ratings yet
- Obturator Tehnology Curs Vi EnglDocument35 pagesObturator Tehnology Curs Vi EnglOlgutZa BoianNo ratings yet
- Transpalatal, Nance & Lingual Arch Appliances: Clinical Tips and ApplicationsDocument9 pagesTranspalatal, Nance & Lingual Arch Appliances: Clinical Tips and ApplicationsbanyubiruNo ratings yet
- Instrumentation and Techniques in Equine Fracture Fixation: Joerg Auer, OMV, MS and Jeffrey P Watkins, DVM, MSDocument20 pagesInstrumentation and Techniques in Equine Fracture Fixation: Joerg Auer, OMV, MS and Jeffrey P Watkins, DVM, MSSergio Nieves MoranNo ratings yet
- Study Relating To Biomedical SubjectsDocument8 pagesStudy Relating To Biomedical Subjectsyisixo8693No ratings yet
- Feldmann2015 Significado AnclajeDocument7 pagesFeldmann2015 Significado AnclajeGILBERTO AGUDELO JIMENEZNo ratings yet
- Extraction Site Reconstruction For Alveolar Ridge Preservation. Part 2: Membrane-Assisted Surgical TechniqueDocument4 pagesExtraction Site Reconstruction For Alveolar Ridge Preservation. Part 2: Membrane-Assisted Surgical TechniqueLuis MonteroNo ratings yet
- 1.3 SutureDocument10 pages1.3 SutureJerry XingNo ratings yet
- (Case Report) A Simplified Approach To Semi-Precision AttachmentDocument7 pages(Case Report) A Simplified Approach To Semi-Precision AttachmentYouju ChouNo ratings yet
- Overview of Innovative Advances in Bioresorbable Plate Systems For Oral and Maxillofacial SurgeryDocument12 pagesOverview of Innovative Advances in Bioresorbable Plate Systems For Oral and Maxillofacial SurgeryAshish PandaNo ratings yet
- Materi OSC DamonDocument20 pagesMateri OSC Damonfika_khayanNo ratings yet
- Paper JBME Muftu Bozkaya 2004Document10 pagesPaper JBME Muftu Bozkaya 2004Bùi Mạnh MạnhNo ratings yet
- Implant ResearchDocument8 pagesImplant ResearchFBI LUC1FeRNo ratings yet
- Implant-Retained Cantilever Fixed Prosthesis: Where and WhenDocument4 pagesImplant-Retained Cantilever Fixed Prosthesis: Where and WhenSitiKhadijahNo ratings yet
- Implantes SubperiosticosDocument8 pagesImplantes SubperiosticosJondalys LópezNo ratings yet
- JEsthetRestorDent 2023 Pelekanos TranslucentmonolithiczirconiatitaniumsupportedFP1fullarchprosthesisADocument11 pagesJEsthetRestorDent 2023 Pelekanos TranslucentmonolithiczirconiatitaniumsupportedFP1fullarchprosthesisAJorge AlvaradoNo ratings yet
- Artigo 11Document22 pagesArtigo 11rhuanaNo ratings yet
- Crown Removers A ReviewDocument5 pagesCrown Removers A ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Prosthetic Management of An Existing Transmandibular Implant: A Clinical ReportDocument5 pagesProsthetic Management of An Existing Transmandibular Implant: A Clinical ReportDragos CiongaruNo ratings yet
- Mini ScrewsDocument29 pagesMini ScrewsdrsankhyaNo ratings yet
- Dental Implants Introduction To Dental ImplantDocument7 pagesDental Implants Introduction To Dental Implantsherif shafeyNo ratings yet
- Silver Coating On Dental Implant-Abutment ConnectiDocument9 pagesSilver Coating On Dental Implant-Abutment ConnectiJose Manuel Quintero RomeroNo ratings yet
- Dental Implants Introduction To Dental ImplantDocument7 pagesDental Implants Introduction To Dental ImplantJavaria IftekharNo ratings yet
- Crown Removers A ReviewDocument5 pagesCrown Removers A ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Magnetic and Snap AttachmentDocument16 pagesMagnetic and Snap AttachmentleniotogniNo ratings yet
- Case Report: A Case Report of Peritoneal Tuberculosis: A Challenging DiagnosisDocument4 pagesCase Report: A Case Report of Peritoneal Tuberculosis: A Challenging DiagnosisDumitru RadulescuNo ratings yet
- Caz Bun 3Document7 pagesCaz Bun 3Dumitru RadulescuNo ratings yet
- Caz Bun 7Document2 pagesCaz Bun 7Dumitru RadulescuNo ratings yet
- Thinking Outside The Lungs: A Case of Disseminated Abdominal TuberculosisDocument6 pagesThinking Outside The Lungs: A Case of Disseminated Abdominal TuberculosisDumitru RadulescuNo ratings yet
- Journal of Medical Case ReportsDocument5 pagesJournal of Medical Case ReportsDumitru RadulescuNo ratings yet
- Analysis of Recent Cases of Intestinal Tuberculosis in JapanDocument6 pagesAnalysis of Recent Cases of Intestinal Tuberculosis in JapanDumitru RadulescuNo ratings yet
- Peritoneal Carcinomatosis and Its Mimics - Review of CT Findings For Differential DiagnosisDocument6 pagesPeritoneal Carcinomatosis and Its Mimics - Review of CT Findings For Differential DiagnosisDumitru RadulescuNo ratings yet
- Pooled Analysis of 163 Published Tuberculous Peritonitis Cases From TurkeyDocument7 pagesPooled Analysis of 163 Published Tuberculous Peritonitis Cases From TurkeyDumitru RadulescuNo ratings yet
- Tuberculous Peritonitis Presenting As An Acute Abdomen: A Case ReportDocument4 pagesTuberculous Peritonitis Presenting As An Acute Abdomen: A Case ReportDumitru RadulescuNo ratings yet
- Endoscopia: Diagnostic Approach of Intestinal Tuberculosis: Case and Literature ReviewDocument4 pagesEndoscopia: Diagnostic Approach of Intestinal Tuberculosis: Case and Literature ReviewDumitru RadulescuNo ratings yet
- Tuberculous Peritonitis The Effectiveness of Diagnostic Laparoscopy and The Perioperative Infectious Prevention - A Case ReportDocument4 pagesTuberculous Peritonitis The Effectiveness of Diagnostic Laparoscopy and The Perioperative Infectious Prevention - A Case ReportDumitru RadulescuNo ratings yet
- Peritoneal Tuberculosis: The Great Mimicker: Case StudyDocument5 pagesPeritoneal Tuberculosis: The Great Mimicker: Case StudyDumitru RadulescuNo ratings yet
- A Prospective Comparative Study Between Staplers and Conventional Hand-Sewn Anastomosis in Gastrointestinal SurgeryDocument126 pagesA Prospective Comparative Study Between Staplers and Conventional Hand-Sewn Anastomosis in Gastrointestinal SurgeryDumitru RadulescuNo ratings yet
- De TradusDocument13 pagesDe TradusDumitru RadulescuNo ratings yet
- NLR Blood Neutrophil To Lymphocyte Count As A Prognostic Marker in Liver Cirrhosis PDFDocument124 pagesNLR Blood Neutrophil To Lymphocyte Count As A Prognostic Marker in Liver Cirrhosis PDFDumitru RadulescuNo ratings yet
- Factors Contributing To SMALL INTESTINE Suture Line Disruption PDFDocument117 pagesFactors Contributing To SMALL INTESTINE Suture Line Disruption PDFDumitru RadulescuNo ratings yet
- Articol Pneumonii 2016Document18 pagesArticol Pneumonii 2016Dumitru RadulescuNo ratings yet
- Gastric Outlet ObstructionDocument59 pagesGastric Outlet Obstructionmaryam tariqNo ratings yet
- Adult Pyloric StenosisDocument2 pagesAdult Pyloric StenosiszapomannNo ratings yet
- 65 Stenoza GDDDocument7 pages65 Stenoza GDDGabriela MilitaruNo ratings yet
- Surgery OspeDocument129 pagesSurgery Ospeudvash2024No ratings yet
- 3-Approach To Epigastric PainDocument62 pages3-Approach To Epigastric PainAbdulrahman NanakaliNo ratings yet
- Surgical Management of Peptic Ulcer Disease - UpToDateDocument29 pagesSurgical Management of Peptic Ulcer Disease - UpToDatenoskovNo ratings yet
- A Clinical Study of Gastric Outlet Obstruction in Adults''Document19 pagesA Clinical Study of Gastric Outlet Obstruction in Adults''safasayedNo ratings yet
- Clinical Factors Responsible For Gastric Outlet Obstruction in Patients From Bihar RegionDocument4 pagesClinical Factors Responsible For Gastric Outlet Obstruction in Patients From Bihar RegionzapomannNo ratings yet
- Gastric Outlet ObstructionDocument25 pagesGastric Outlet ObstructionDr Shahzad Alam ShahNo ratings yet
- Gastric Outlet ObstructionDocument35 pagesGastric Outlet ObstructionsiddhantaNo ratings yet
- Gastric Outlet Obstruction: Its Surgical ManagementDocument40 pagesGastric Outlet Obstruction: Its Surgical ManagementGudeta shegerNo ratings yet
- Tuberculosis Gastrointestinal PDFDocument11 pagesTuberculosis Gastrointestinal PDFRafael Andrés Hanssen HargitayNo ratings yet
- Question Bank: Chapterwise (Wbuhs)Document188 pagesQuestion Bank: Chapterwise (Wbuhs)Saikat MondalNo ratings yet
- 1.40 (Surgery) GIT Surgical Diseases - Diagnostics - Obesity ManagementDocument10 pages1.40 (Surgery) GIT Surgical Diseases - Diagnostics - Obesity ManagementLeo Mari Go LimNo ratings yet
- Gastric Outlet ObstructionDocument10 pagesGastric Outlet ObstructionMpanso Ahmad AlhijjNo ratings yet
- Gastric Outlet Obstruction Due To Peptic Ulcer DiseaseDocument4 pagesGastric Outlet Obstruction Due To Peptic Ulcer DiseaseTeguh RahNo ratings yet
- Overview of The Complications of Peptic Ulcer DiseaseDocument27 pagesOverview of The Complications of Peptic Ulcer DiseaseIulia OpreaNo ratings yet