Download as pdf or txt
You might also like
- Micro Econ 6 Principles of Microeconomics 6Th Edition William A Mceachern Full ChapterDocument67 pagesMicro Econ 6 Principles of Microeconomics 6Th Edition William A Mceachern Full Chapterchristine.parsons231100% (6)
- Osha 10-Hour Construction Industry: How To Use This Study GuideDocument39 pagesOsha 10-Hour Construction Industry: How To Use This Study GuideGabriel ParksNo ratings yet
- Credit Risk QuestionnaireDocument4 pagesCredit Risk QuestionnaireBhaumik Nayak100% (1)
- Invoice: P.T.Evergreen Shipping Agency IndonesiaDocument1 pageInvoice: P.T.Evergreen Shipping Agency IndonesiaDody DermawanNo ratings yet
- Association Between Psoriasis and Erectile Dysfunction: A Meta-AnalysisDocument14 pagesAssociation Between Psoriasis and Erectile Dysfunction: A Meta-AnalysisRista RiaNo ratings yet
- Dermatitis Atopic Kim2016Document18 pagesDermatitis Atopic Kim2016wulanNo ratings yet
- Opth 9 1719Document12 pagesOpth 9 1719Anggia BungaNo ratings yet
- Contoh SR1Document13 pagesContoh SR1Meutia SaraNo ratings yet
- A Systematic Review and Meta-Analysis of The Regional and Age-Related Differences in Atopic Dermatitis Clinical CharacteristicsDocument12 pagesA Systematic Review and Meta-Analysis of The Regional and Age-Related Differences in Atopic Dermatitis Clinical CharacteristicsLiliana DuqueNo ratings yet
- PIIS193945512030380XDocument17 pagesPIIS193945512030380XLarissa DiasNo ratings yet
- Journal of Affective Disorders Volume 142 Issue 2012 (Doi 10.1016/s0165-0327 (12) 70004-6) Roy, Tapash Lloyd, Cathy E. - Epidemiology of Depression and Diabetes - A Systematic ReviewDocument14 pagesJournal of Affective Disorders Volume 142 Issue 2012 (Doi 10.1016/s0165-0327 (12) 70004-6) Roy, Tapash Lloyd, Cathy E. - Epidemiology of Depression and Diabetes - A Systematic ReviewSinta Rahmah SariNo ratings yet
- 10 1111@ijd 14763Document17 pages10 1111@ijd 14763via_anggraeni15No ratings yet
- HHS Public Access: New Treatment Guidelines For Sjögren's DiseaseDocument24 pagesHHS Public Access: New Treatment Guidelines For Sjögren's DiseaseChon ChiNo ratings yet
- Hidradenitis Suppurativa and Metabolic Syndrome - Systematic Review and Adjusted Meta-AnalysisDocument6 pagesHidradenitis Suppurativa and Metabolic Syndrome - Systematic Review and Adjusted Meta-AnalysisKianeNo ratings yet
- Migraine As A Risk Factor For Primary Open Angle Glaucoma A Systematic Review and Meta-AnalysisDocument8 pagesMigraine As A Risk Factor For Primary Open Angle Glaucoma A Systematic Review and Meta-AnalysisEsteven Tanu GunawanNo ratings yet
- JournalDocument10 pagesJournalSalsabila Nur HamdiNo ratings yet
- Kuniyoshi 2021Document12 pagesKuniyoshi 2021Brisila PesantezNo ratings yet
- Allergic Contact Dermatitis To Personal Care Products and Topical Medications in Adults With Atopic DermatitisDocument12 pagesAllergic Contact Dermatitis To Personal Care Products and Topical Medications in Adults With Atopic DermatitisSyifa Rahmawati PutriNo ratings yet
- 10 1002@msc 1498Document13 pages10 1002@msc 1498Ricardo PietrobonNo ratings yet
- Beck 2018Document9 pagesBeck 2018Sung Soon ChangNo ratings yet
- The Quiet TED-A Special Subgroup of Thyroid Eye DiseaseDocument5 pagesThe Quiet TED-A Special Subgroup of Thyroid Eye DiseaseFachri PadmaridhoNo ratings yet
- Int Endodontic J - 2016 - Berlin Broner - Association Between Apical Periodontitis and Cardiovascular Diseases ADocument13 pagesInt Endodontic J - 2016 - Berlin Broner - Association Between Apical Periodontitis and Cardiovascular Diseases ANaireeNo ratings yet
- JournalDocument7 pagesJournalhashiNo ratings yet
- 1 s2.0 S0190962222000809 MainDocument20 pages1 s2.0 S0190962222000809 MainChristina IndrayantiNo ratings yet
- Song 2013Document5 pagesSong 2013VioNo ratings yet
- Amino Sharia e 2017Document6 pagesAmino Sharia e 2017Heba AtefNo ratings yet
- Shi2017 PDFDocument6 pagesShi2017 PDFEka FaridaNo ratings yet
- Jamadermatology Wan 2021 Oi 210001 1623774356.72355Document7 pagesJamadermatology Wan 2021 Oi 210001 1623774356.72355Meilani MelaNo ratings yet
- Various Diagnostic Criteria For Atopic Dermatitis (AD) : A Proposal of Reliable Estimation of Atopic Dermatitis in Childhood (REACH) Criteria, A Novel Questionnaire-Based Diagnostic Tool For ADDocument9 pagesVarious Diagnostic Criteria For Atopic Dermatitis (AD) : A Proposal of Reliable Estimation of Atopic Dermatitis in Childhood (REACH) Criteria, A Novel Questionnaire-Based Diagnostic Tool For ADJuliana SusantioNo ratings yet
- Frequency, Severity and Related Factors of Androgenetic Alopecia in Dermatology Outpatient Clinic: Hospital-Based Cross-Sectional Study in TurkeyDocument6 pagesFrequency, Severity and Related Factors of Androgenetic Alopecia in Dermatology Outpatient Clinic: Hospital-Based Cross-Sectional Study in TurkeyFilza AldinaNo ratings yet
- Epidemiology and Genetics of Hypodontia and Microdontia A Study of Twin FamiliesDocument6 pagesEpidemiology and Genetics of Hypodontia and Microdontia A Study of Twin FamiliesSTEFANNY MERELONo ratings yet
- Literature Review On Rheumatoid ArthritisDocument6 pagesLiterature Review On Rheumatoid Arthritispib0b1nisyj2100% (1)
- PIIS1063458413004020Document2 pagesPIIS1063458413004020edo adimastaNo ratings yet
- Meta AnalisisDocument23 pagesMeta AnalisisLORENA MONSERRAT MANCERA - HERNANDEZNo ratings yet
- Cutoff 4-5Document7 pagesCutoff 4-5Ian HuangNo ratings yet
- Low Vitamin D Levels Are Associated With Atopic Dermatitis, But Not Allergic Rhinitis, Asthma, or Ige Sensitization, in The Adult Korean PopulationDocument15 pagesLow Vitamin D Levels Are Associated With Atopic Dermatitis, But Not Allergic Rhinitis, Asthma, or Ige Sensitization, in The Adult Korean PopulationJundi Agung SamjayaNo ratings yet
- Insight On Pathogenesis of Lifelong Premature Ejaculation: Inverse Relationship Between Lifelong Premature Ejaculation and ObesityDocument4 pagesInsight On Pathogenesis of Lifelong Premature Ejaculation: Inverse Relationship Between Lifelong Premature Ejaculation and ObesitymaithamNo ratings yet
- Atopic Eczema in Adulthood and Risk of Depression and Anxiety: A Population-Based Cohort StudyDocument26 pagesAtopic Eczema in Adulthood and Risk of Depression and Anxiety: A Population-Based Cohort Studyyenny handayani sihiteNo ratings yet
- Iej 12710Document13 pagesIej 12710oanaNo ratings yet
- Environmental Factors Associated With Autism SpectrumDocument23 pagesEnvironmental Factors Associated With Autism SpectrumElaineBaptistaNo ratings yet
- Prediction Models For The Diagnosis of AsthmaDocument11 pagesPrediction Models For The Diagnosis of AsthmaIJRASETPublicationsNo ratings yet
- jad_2018_64-1_jad-64-1-jad180013_jad-64-jad180013Document13 pagesjad_2018_64-1_jad-64-1-jad180013_jad-64-jad180013ThormmmNo ratings yet
- The Association Between Iron Deficiency and Otitis Media With EffusionDocument4 pagesThe Association Between Iron Deficiency and Otitis Media With EffusionFelicia FloraNo ratings yet
- Effects of Risk Factors On Periodontal Disease Defined by Calibrated Community Periodontal Index and Loss of Attachment ScoresDocument23 pagesEffects of Risk Factors On Periodontal Disease Defined by Calibrated Community Periodontal Index and Loss of Attachment ScoresinkaNo ratings yet
- Rheumatoid Arthritis Literature ReviewDocument8 pagesRheumatoid Arthritis Literature Reviewc5qz47sm100% (1)
- "Clinical Features of Women With Gout Arthritis." A Systematic ReviewDocument8 pages"Clinical Features of Women With Gout Arthritis." A Systematic Reviewsyahrul ridengNo ratings yet
- HHS Public Access: Achalasia Treatment, Outcomes, Utilization, and Costs: A Population-Based Study From The United StatesDocument12 pagesHHS Public Access: Achalasia Treatment, Outcomes, Utilization, and Costs: A Population-Based Study From The United StatesInomy ClaudiaNo ratings yet
- Meta Analysis - Degree of Myopia and Glaucoma Risk A Dose ResponseDocument13 pagesMeta Analysis - Degree of Myopia and Glaucoma Risk A Dose ResponseMade DesmantaNo ratings yet
- Epidemiology of OsteoarthritisDocument12 pagesEpidemiology of Osteoarthritisdhimas satriaNo ratings yet
- Thyroid Eye Disease- Therapy in the Active PhaseDocument12 pagesThyroid Eye Disease- Therapy in the Active PhasediegomcrespoNo ratings yet
- Population-Wide Analysis of Differences in Disease Progression Patterns in Men and WomenDocument14 pagesPopulation-Wide Analysis of Differences in Disease Progression Patterns in Men and WomenSagar SononeNo ratings yet
- Billings Et Al-2018-Journal of Clinical PeriodontologyDocument19 pagesBillings Et Al-2018-Journal of Clinical PeriodontologyCristian CulcitchiNo ratings yet
- Does Endometriosis Disturb Mental Health and Quality of Life - A Systematic Review and Meta-AnalysisDocument21 pagesDoes Endometriosis Disturb Mental Health and Quality of Life - A Systematic Review and Meta-AnalysisAdamastor MessiasNo ratings yet
- Stapleton 2017Document32 pagesStapleton 2017Anggia BungaNo ratings yet
- IJD - Volume 24 - Issue 3 - Pages 172-178Document7 pagesIJD - Volume 24 - Issue 3 - Pages 172-178Tony BusiNo ratings yet
- Body Mass Index and Susceptibility To Knee Osteoarthritis: A Systematic Review and Meta-AnalysisDocument7 pagesBody Mass Index and Susceptibility To Knee Osteoarthritis: A Systematic Review and Meta-AnalysisAmalia RosaNo ratings yet
- Jurnal JkmsDocument8 pagesJurnal JkmsArif Kurniawan ListiantoNo ratings yet
- Dewi Iramayana - Physical Activity and Risk of Age Related CataractDocument7 pagesDewi Iramayana - Physical Activity and Risk of Age Related Cataractbudi haryadiNo ratings yet
- Are Alexithymia and Empathy Predicting FactorsDocument7 pagesAre Alexithymia and Empathy Predicting FactorsRicardoNo ratings yet
- Fimmu 15 1356714Document15 pagesFimmu 15 1356714KEVIN ALEXANDER LLIVICURA CURILLONo ratings yet
- Combining Orthopedic Special Tests To ImDocument6 pagesCombining Orthopedic Special Tests To ImVladislav KotovNo ratings yet
- ADHD Asthma MainDocument11 pagesADHD Asthma MainGyík EmberNo ratings yet
- Noutati Din Diagnosticarea AstmuluiDocument1 pageNoutati Din Diagnosticarea AstmuluiPetrescu MihaiNo ratings yet
- Nicole Elyse NelsonDocument3 pagesNicole Elyse Nelsonapi-331206184No ratings yet
- Garden Growers Nursery Technician: Job DescriptionDocument2 pagesGarden Growers Nursery Technician: Job DescriptionKevin PittNo ratings yet
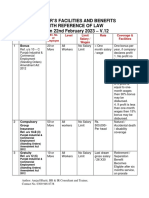
- V 12 - Schedule of Important Labor Laws - 22.02.2023Document6 pagesV 12 - Schedule of Important Labor Laws - 22.02.2023haris hafeezNo ratings yet
- Cmis5103 Assignment Usty-Sept16Document5 pagesCmis5103 Assignment Usty-Sept16Hamood AliNo ratings yet
- How To Install A Light FixtureDocument5 pagesHow To Install A Light FixtureMarc RiomalosNo ratings yet
- Advertising 5Document41 pagesAdvertising 5Sông HươngNo ratings yet
- Accounting Question BankDocument217 pagesAccounting Question BankFaiza TahreemNo ratings yet
- Weaving, Knitting, Poy, CP, TexturisingDocument78 pagesWeaving, Knitting, Poy, CP, TexturisingBULTAN SARKAR100% (2)
- 20 Preparation Question: Contract: Contract 1 Contract 2 Contract 3 Contract 4Document2 pages20 Preparation Question: Contract: Contract 1 Contract 2 Contract 3 Contract 4SerenaNo ratings yet
- I-765 Online Filing Instructions - FINALDocument13 pagesI-765 Online Filing Instructions - FINALTrân LêNo ratings yet
- Omml 0416 19Document14 pagesOmml 0416 19ahmed nasserNo ratings yet
- Manuals PDFDocument65 pagesManuals PDFRafael NievesNo ratings yet
- Nantes2018 FLV VerrieresV4Document9 pagesNantes2018 FLV VerrieresV4Fikri Bin Abdul ShukorNo ratings yet
- Flyback ConverterDocument18 pagesFlyback Converter25Krishnapriya S SNo ratings yet
- Prospectus 2014Document12 pagesProspectus 2014PhaniKumarChodavarapuNo ratings yet
- TPC Repository Whitepaper v1 2Document55 pagesTPC Repository Whitepaper v1 2buxabuxa32No ratings yet
- Conduct Award RubricsDocument12 pagesConduct Award RubricsMark Antony M. CaseroNo ratings yet
- 2010-2016: Formation and Pre-Debut Activities: The X FactorDocument1 page2010-2016: Formation and Pre-Debut Activities: The X FactorHQNo ratings yet
- Annual ReportSummary 2012Document2 pagesAnnual ReportSummary 2012Erick Antonio Castillo GurdianNo ratings yet
- CE409 Quantity Surveying and ValuationDocument2 pagesCE409 Quantity Surveying and ValuationBala GopalNo ratings yet
- Using MySQL With LabVIEWDocument49 pagesUsing MySQL With LabVIEWsion2010363650% (2)
- Moy Ya Lim Yao DIGEST, Angelique AquinoDocument2 pagesMoy Ya Lim Yao DIGEST, Angelique AquinoAngeliqueAquinoNo ratings yet
- ContinueDocument5 pagesContinueuWu uWuNo ratings yet
- DMTR DataDocument3 pagesDMTR DataŽiga PosediNo ratings yet
- 2010 11 11 EreDocument3 pages2010 11 11 Eremet140No ratings yet
- 05 - Quiz - 1 - HRMDocument3 pages05 - Quiz - 1 - HRMMillania ThanaNo ratings yet