Download as docx, pdf, or txt
You might also like
- ZBORNIK NeurologijaDocument443 pagesZBORNIK NeurologijaSan KosNo ratings yet
- Referat MG Desya BismillahDocument20 pagesReferat MG Desya BismillahDesya BillaNo ratings yet
- 2 Myasthenia Gravis and MS 2Document50 pages2 Myasthenia Gravis and MS 2Rawbeena RamtelNo ratings yet
- Myasthenia Gravis: Assoc. Prof. Dr. Rodica BălașaDocument31 pagesMyasthenia Gravis: Assoc. Prof. Dr. Rodica BălașaIstván MáthéNo ratings yet
- Myasthenia Gravis: New Insights Into The Effect of Musk Antibodies and Acetylcholinesterase InhibitorsDocument23 pagesMyasthenia Gravis: New Insights Into The Effect of Musk Antibodies and Acetylcholinesterase InhibitorsDim SumNo ratings yet
- Physiology, Neuromuscular Junction of Skeletal MuscleDocument8 pagesPhysiology, Neuromuscular Junction of Skeletal Musclemethmal subasingheNo ratings yet
- Review: Myasthenic CrisisDocument11 pagesReview: Myasthenic CrisisRaisha TriasariNo ratings yet
- Diagnosis and Management of Myasthenia Gravis: ReviewDocument9 pagesDiagnosis and Management of Myasthenia Gravis: ReviewnetifarhatiiNo ratings yet
- 51.differential Diagnosis of Myasthenia Gravis - A ReviewDocument11 pages51.differential Diagnosis of Myasthenia Gravis - A ReviewSeptime TyasNo ratings yet
- Miastenia GravisDocument28 pagesMiastenia Gravismariateresajijon7No ratings yet
- Myasthenia GravisDocument25 pagesMyasthenia GravisIka Wulan PermataNo ratings yet
- Journal of Autoimmunity: Sonia Berrih-Aknin, Rozen Le PanseDocument11 pagesJournal of Autoimmunity: Sonia Berrih-Aknin, Rozen Le PanseHelen SobczykNo ratings yet
- Myasthenia Gravis and Other Neuromuscular Junction DisordersDocument8 pagesMyasthenia Gravis and Other Neuromuscular Junction Disordersidno1008No ratings yet
- Myastheni Gravis TheoryDocument3 pagesMyastheni Gravis Theoryjohnlester_jlfNo ratings yet
- (DONE) Peripheral LesionsDocument11 pages(DONE) Peripheral LesionsAstha Tusharbhai PatelNo ratings yet
- Myasthenia Gravis - PathophysiologyDocument3 pagesMyasthenia Gravis - PathophysiologyDill BadaróNo ratings yet
- Myasthenia Gravis: PathophysiologyDocument7 pagesMyasthenia Gravis: PathophysiologyAmrit Preet KaurNo ratings yet
- 1 SMDocument6 pages1 SMAjeng Ratna HaryantiNo ratings yet
- Myasthenia Gravis and Lambert-Eaton Myasthenic Syndrome - Continuum December 2016Document28 pagesMyasthenia Gravis and Lambert-Eaton Myasthenic Syndrome - Continuum December 2016Habib G. Moutran BarrosoNo ratings yet
- 35 - Neuromuscular Junction Disorders LectureDocument45 pages35 - Neuromuscular Junction Disorders LectureRanjit SharmaNo ratings yet
- Neuromuscular TransmissionDocument24 pagesNeuromuscular TransmissionAshima FarrukhNo ratings yet
- Mia SteniaDocument7 pagesMia Steniamilenerato2240No ratings yet
- Ocular Myasthenia Gravis: A Review Review Article: Epidemiology and DemographicsDocument8 pagesOcular Myasthenia Gravis: A Review Review Article: Epidemiology and DemographicsMunteanu AlexandruNo ratings yet
- CME Article 2010 JulyDocument10 pagesCME Article 2010 JulyIlda EscalanteNo ratings yet
- Motor Endplate Disorders Myasthenia Gravis Overview and DefinitionDocument4 pagesMotor Endplate Disorders Myasthenia Gravis Overview and DefinitionPJHGNo ratings yet
- Update On Ocular Myasthenia GravisDocument12 pagesUpdate On Ocular Myasthenia GravisAnonymous QLadTClydkNo ratings yet
- NMJ Disorders: For Clinical I StudentsDocument49 pagesNMJ Disorders: For Clinical I StudentsdenekeNo ratings yet
- Definition of TermssDocument8 pagesDefinition of TermssMariel AbatayoNo ratings yet
- Myasthenia Gravis in Clinical Practice: Miastenia Gravis Na Prática ClínicaDocument9 pagesMyasthenia Gravis in Clinical Practice: Miastenia Gravis Na Prática ClínicaMasDhedotNo ratings yet
- Anaesthesia and Myasthenia GravisDocument12 pagesAnaesthesia and Myasthenia Gravis37435rlcNo ratings yet
- Cases For Review For CH 567-SignedDocument2 pagesCases For Review For CH 567-SignedGhieGhie TPNo ratings yet
- Myasthenia Gravis Lecture 12Document59 pagesMyasthenia Gravis Lecture 12Pop D. MadalinaNo ratings yet
- PharmaDocument9 pagesPharmaمحسن حدوان عليخانNo ratings yet
- Myasthenia Gravis - A Review of Current TherapeutiDocument7 pagesMyasthenia Gravis - A Review of Current TherapeutiZainal AbidinNo ratings yet
- Multifocal Motor Neuropathy - StatPearls - NCBI BookshelfDocument6 pagesMultifocal Motor Neuropathy - StatPearls - NCBI BookshelfAnakin SkywalkerNo ratings yet
- Diagnostic Workup: CNS Diplopia Dysarthria Dysphagia Multiple SclerosisDocument2 pagesDiagnostic Workup: CNS Diplopia Dysarthria Dysphagia Multiple SclerosisvirtualNo ratings yet
- Myasthenia Gravis: A Review: Hideyuki Matsumoto, MD, PHD and Yoshikazu Ugawa, MD, PHDDocument7 pagesMyasthenia Gravis: A Review: Hideyuki Matsumoto, MD, PHD and Yoshikazu Ugawa, MD, PHDZainal AbidinNo ratings yet
- Cells 08 01578Document22 pagesCells 08 01578dasNo ratings yet
- Physio Essay #4Document2 pagesPhysio Essay #4Maria Margarita Chon100% (1)
- RJN 2017 2 Art-04Document3 pagesRJN 2017 2 Art-04Ana GabrielaNo ratings yet
- Sindrome Paraneoplasico Neurologico NejmDocument12 pagesSindrome Paraneoplasico Neurologico NejmFernando Rodriguez BayonaNo ratings yet
- Myasthenia Gravis: Murali Thavasothy DCH MRCP FRCA Nicholas Hirsch FRCADocument3 pagesMyasthenia Gravis: Murali Thavasothy DCH MRCP FRCA Nicholas Hirsch FRCAMirela CiobanescuNo ratings yet
- Neuromuscular Junction DisorderDocument10 pagesNeuromuscular Junction DisorderZosmita Shane GalgaoNo ratings yet
- Lambert-Eaton Myasthenic SyndromeDocument5 pagesLambert-Eaton Myasthenic SyndromeNeil Philip MaturanNo ratings yet
- Myasthenia Gravis, PemeriksaanDocument11 pagesMyasthenia Gravis, PemeriksaansandapuspariniNo ratings yet
- Congenital Myasthenic Syndromes - Symptoms, Causes, Treatment - NORDDocument27 pagesCongenital Myasthenic Syndromes - Symptoms, Causes, Treatment - NORDFlavia BertolozziNo ratings yet
- Step 7 1. Mengapa Pada Skenario Pasien Merasakan Lemah Pada Kelopak Mata Dan Mengapa Paling Berat Dirasakan?Document11 pagesStep 7 1. Mengapa Pada Skenario Pasien Merasakan Lemah Pada Kelopak Mata Dan Mengapa Paling Berat Dirasakan?novkar9No ratings yet
- Review Article Ocular Myasthenia Gravis: A Review: Epidemiology and DemographicsDocument7 pagesReview Article Ocular Myasthenia Gravis: A Review: Epidemiology and DemographicsMaxend Arselino SilooyNo ratings yet
- Joint Seminar With SFEMG/QEMG Group: Single Fiber EMG and Quantitative EMGDocument1 pageJoint Seminar With SFEMG/QEMG Group: Single Fiber EMG and Quantitative EMGShauki AliNo ratings yet
- PBL 10Document4 pagesPBL 10lliioNo ratings yet
- Autoimmunity and Immunotherapy in Narcolepsy: Review ArticleDocument7 pagesAutoimmunity and Immunotherapy in Narcolepsy: Review Articleece142No ratings yet
- Neuromuscular Junction DisordersDocument20 pagesNeuromuscular Junction DisordersMunteanu AlexandruNo ratings yet
- Paraneoplastic Neurologic Syndromes Are Defined and Characterized by An Inappropriate Immune Response Targeting Native Nervous System Antigens That Are Ectopically Expressed by A Systemic TumorDocument11 pagesParaneoplastic Neurologic Syndromes Are Defined and Characterized by An Inappropriate Immune Response Targeting Native Nervous System Antigens That Are Ectopically Expressed by A Systemic TumorAnonymous ZUaUz1wwNo ratings yet
- Presented By: VIVEK DEVDocument38 pagesPresented By: VIVEK DEVFranchesca LugoNo ratings yet
- Neuromuscular DisordersDocument3 pagesNeuromuscular DisordersMaharaniDewiNo ratings yet
- Myasthenia Gravis (MG) : AnatomyDocument12 pagesMyasthenia Gravis (MG) : AnatomyCici Novelia ManurungNo ratings yet
- Neuromuscular Junction DisordersDocument32 pagesNeuromuscular Junction Disordersepic sound everNo ratings yet
- Multifocal Motor NeuropathyDocument11 pagesMultifocal Motor Neuropathymedana5No ratings yet
- Constitutive Activation of MAPK Cascade in Acute Quadriplegic MyopathyDocument12 pagesConstitutive Activation of MAPK Cascade in Acute Quadriplegic MyopathyEviNo ratings yet
- FdvfebvterbtfdvDocument9 pagesFdvfebvterbtfdvDesya BillaNo ratings yet
- 2 PDFDocument12 pages2 PDFDesya BillaNo ratings yet
- Tilda: Presentation TemplateDocument25 pagesTilda: Presentation TemplateDesya BillaNo ratings yet
- FdvfebvterbtfdvDocument5 pagesFdvfebvterbtfdvDesya BillaNo ratings yet
- Abstract Floral PPT DesignDocument3 pagesAbstract Floral PPT DesignDesya BillaNo ratings yet
- TH 5 ThyDocument2 pagesTH 5 ThyDesya BillaNo ratings yet
- KORTIKOSTEROID TOPIKAL - Koass Kulit & Kelamin Kelompok 17Document11 pagesKORTIKOSTEROID TOPIKAL - Koass Kulit & Kelamin Kelompok 17Desya BillaNo ratings yet
- Journal Reading: Oleh: Nurul Imaniar 2013730081Document11 pagesJournal Reading: Oleh: Nurul Imaniar 2013730081Desya BillaNo ratings yet
- Ujian Kepaniteraan Klinik Ilmu Penyakit DalamDocument16 pagesUjian Kepaniteraan Klinik Ilmu Penyakit DalamDesya BillaNo ratings yet
- Referat MG Desya BismillahDocument20 pagesReferat MG Desya BismillahDesya BillaNo ratings yet
- Diagnosis and Management of Myasthenia Gravis: By: Desya Billa Kusuma AnindhiraDocument38 pagesDiagnosis and Management of Myasthenia Gravis: By: Desya Billa Kusuma AnindhiraDesya BillaNo ratings yet
- Msds en Shell Tellus s2 M 68Document15 pagesMsds en Shell Tellus s2 M 68Debora Septania PurbaNo ratings yet
- Training Updated RaytoDocument116 pagesTraining Updated RaytoJared GongoraNo ratings yet
- Ilovepdf Merged 2Document41 pagesIlovepdf Merged 2api-533764142No ratings yet
- Fine Love Dolls User ManualDocument11 pagesFine Love Dolls User ManualFine Love Dolls (Ultra Realistic TPE Dolls)33% (3)
- Sem - Ii Pharmacology Lab ManualDocument36 pagesSem - Ii Pharmacology Lab ManualLokesh MahataNo ratings yet
- 350 ML (Amount of Beer) × 0.05 (Alcoholic Content) × 0.792 (Alcoholic Density) 13.860 G Theoretical Blood Alcohol Concentration 13,860 MG / 52,500 ML 0.264 MG/MLDocument5 pages350 ML (Amount of Beer) × 0.05 (Alcoholic Content) × 0.792 (Alcoholic Density) 13.860 G Theoretical Blood Alcohol Concentration 13,860 MG / 52,500 ML 0.264 MG/MLSava VijakNo ratings yet
- Pathology Lecture 2, Cell Injury (Notes/tafree3')Document18 pagesPathology Lecture 2, Cell Injury (Notes/tafree3')Ali Al-Qudsi100% (3)
- 2014 Ftir LabDocument10 pages2014 Ftir LabAnurak OnnnoomNo ratings yet
- Lec 1 Introduction To Nutrition For HealthDocument26 pagesLec 1 Introduction To Nutrition For HealthSherif AliNo ratings yet
- Paranthropology Journal of Anthropologic PDFDocument72 pagesParanthropology Journal of Anthropologic PDFCarlos José Lacava Fernández100% (1)
- Anatomy and Physiology: University of San Agustin Review Center Iloilo City, PhilippinesDocument74 pagesAnatomy and Physiology: University of San Agustin Review Center Iloilo City, PhilippinesChristine Joy MolinaNo ratings yet
- Taps Valves Showers Pipes Gratings Sanitaryware Bath Fittings AccessoriesDocument54 pagesTaps Valves Showers Pipes Gratings Sanitaryware Bath Fittings AccessoriesRAJESHNo ratings yet
- Milky Malunggay PolvoronDocument6 pagesMilky Malunggay PolvoronJohn Kirby PerezNo ratings yet
- Bio-Botany Vol-2 - EM PDFDocument216 pagesBio-Botany Vol-2 - EM PDFsudha1987No ratings yet
- 1.1 CC Civil BrochureDocument4 pages1.1 CC Civil BrochureLuis Larry Bocanegra GomezNo ratings yet
- Design of Exploitation of Quarry For AggregatesDocument3 pagesDesign of Exploitation of Quarry For AggregatesAnonymous IEu0pR5TNo ratings yet
- Answers Quiz2Document3 pagesAnswers Quiz2Salim MattarNo ratings yet
- Research PaperDocument3 pagesResearch PaperKeitu QuijalvoNo ratings yet
- Conversation Review1Document37 pagesConversation Review1Tikie PiyapornNo ratings yet
- Reading Tháng 8-23Document11 pagesReading Tháng 8-23Phạm LinhNo ratings yet
- AV157 ManualDocument8 pagesAV157 ManualtbelhumeurNo ratings yet
- CP 2 Vibration Monitoring and Analysis GuideDocument5 pagesCP 2 Vibration Monitoring and Analysis GuideCristian GarciaNo ratings yet
- Dying Without A Will in PennsylvaniaDocument2 pagesDying Without A Will in PennsylvaniaStephen Garrett100% (7)
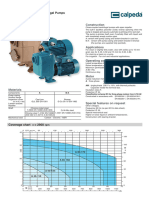
- 1 - A 40-110A - B Self-Priming Centrifugal PumpDocument6 pages1 - A 40-110A - B Self-Priming Centrifugal Pump3dpshabbirNo ratings yet
- Where Does The Glycolysis OccourDocument2 pagesWhere Does The Glycolysis OccourMaria Claudette Andres AggasidNo ratings yet
- Interim Valuation 1Document11 pagesInterim Valuation 1musthaqhassan100% (1)
- Ibadan - Nigeria - Reconnaissance - Visit - KopieDocument10 pagesIbadan - Nigeria - Reconnaissance - Visit - KopieAgung BudiantoNo ratings yet
- Across National Tax Jurisdictions. Hence, A Company's Transfer-Pricing PoliciesDocument2 pagesAcross National Tax Jurisdictions. Hence, A Company's Transfer-Pricing PoliciesLJBernardoNo ratings yet
- Lung AbscessDocument28 pagesLung AbscessBobet ReñaNo ratings yet
- TKN - VELP Application NoteDocument4 pagesTKN - VELP Application NoteAshraf MohamedNo ratings yet