
Assignment 1 CD
Assignment 1 CD
You might also like
- Piper Mike - Surprisingly SimpleDocument54 pagesPiper Mike - Surprisingly SimpleMoona Wahab100% (2)
- MSM GrasDocument84 pagesMSM GrasGopalaKrishnan Sivaraman0% (1)
- Title: Children's Oral Health Strategy in The UKDocument8 pagesTitle: Children's Oral Health Strategy in The UKshahryar eskandarzadeNo ratings yet
- Literature Review On Prevalence of Dental CariesDocument5 pagesLiterature Review On Prevalence of Dental Cariesc5t0jsyn100% (1)
- Snack and ToothbrushingDocument8 pagesSnack and Toothbrushingsandra del pilarNo ratings yet
- Wong 2017Document24 pagesWong 2017Ngoc MinhNo ratings yet
- Dissertation Topics in Community DentistryDocument7 pagesDissertation Topics in Community DentistryOnlinePaperWritingServiceCanada100% (1)
- Almedleg 2021 - Causes N Diagnosis ECC - SRDocument12 pagesAlmedleg 2021 - Causes N Diagnosis ECC - SRDR ANKITA KHADENo ratings yet
- Dental Caries PandemicDocument5 pagesDental Caries PandemicKarla González GNo ratings yet
- Guideline On Caries-Risk Assessment and Management For Infants, Children, and AdolescentsDocument8 pagesGuideline On Caries-Risk Assessment and Management For Infants, Children, and AdolescentsPriscila Belén Chuhuaicura SotoNo ratings yet
- Children: Dental Caries and Oral Health in Children-Special IssueDocument3 pagesChildren: Dental Caries and Oral Health in Children-Special IssuecareNo ratings yet
- Managing C R in Adults: Aries ISKDocument6 pagesManaging C R in Adults: Aries ISKSOMVIR KUMARNo ratings yet
- Caries Temprana de La InfanciaDocument6 pagesCaries Temprana de La InfanciaAna CristernaNo ratings yet
- Jessicaleeliterature Review PaperDocument6 pagesJessicaleeliterature Review Paperapi-725689989No ratings yet
- Caries Risk AssessmentDocument8 pagesCaries Risk AssessmentGrace Shabrina HapsariNo ratings yet
- Foreign LiteratureDocument13 pagesForeign LiteratureJm. n BelNo ratings yet
- Ecc Lit Review - PDocument7 pagesEcc Lit Review - Papi-720438286No ratings yet
- Dental Health AustraliaDocument8 pagesDental Health AustraliajohnmccauleyNo ratings yet
- Comm Dent Oral Epid 2023 SharmaDocument15 pagesComm Dent Oral Epid 2023 SharmaNatalia DavilaNo ratings yet
- Taf PDFDocument14 pagesTaf PDFrania azzahraNo ratings yet
- Public Health Dentistry Thesis TopicsDocument5 pagesPublic Health Dentistry Thesis Topicss0kuzej0byn2100% (2)
- Obesity and Obesity Related Diseases, Sugar Consumption and Bad Oral Health: A Fatal Epidemic MixturesDocument8 pagesObesity and Obesity Related Diseases, Sugar Consumption and Bad Oral Health: A Fatal Epidemic MixturesAyu DamayNo ratings yet
- Sugar Intake and Dental Decay Results From A National Survey of Children in ScotlandDocument10 pagesSugar Intake and Dental Decay Results From A National Survey of Children in ScotlandAndrada IonescuNo ratings yet
- Caries Prevention in School ChildrenDocument12 pagesCaries Prevention in School ChildrenJatan KothariNo ratings yet
- P ProphylaxisDocument5 pagesP ProphylaxisLeticia Quiñonez VivasNo ratings yet
- Library Dissertation On Early Childhood CariesDocument4 pagesLibrary Dissertation On Early Childhood CariesPayToWritePaperBaltimore100% (1)
- Updated BSP BSPD Perio Guidelines For The Under 18s 2021 FINAL 270921 VC PDF VersionDocument45 pagesUpdated BSP BSPD Perio Guidelines For The Under 18s 2021 FINAL 270921 VC PDF VersionhanaNo ratings yet
- JDM 2018 004 Int@081-086Document6 pagesJDM 2018 004 Int@081-086Miguel Ángel De la Cruz GómezNo ratings yet
- Habits and Social Norms Leading To Childhood CariesDocument16 pagesHabits and Social Norms Leading To Childhood Cariesapi-522555065No ratings yet
- Articulo ObeDocument9 pagesArticulo ObedennisNo ratings yet
- Chapter37 - Prevention of Periodontal - Dis94 PDFDocument13 pagesChapter37 - Prevention of Periodontal - Dis94 PDFDana DanielaNo ratings yet
- Guideline On Caries-Risk Assessment and Management For Infants, Children, and AdolescentsDocument8 pagesGuideline On Caries-Risk Assessment and Management For Infants, Children, and AdolescentsShruti SoodNo ratings yet
- Impact of Lifestyle Variables On Oral Diseases and Oral Health-Related Quality of Life in Children of Milan (Italy)Document16 pagesImpact of Lifestyle Variables On Oral Diseases and Oral Health-Related Quality of Life in Children of Milan (Italy)Zarah Hannah Leah DalmacioNo ratings yet
- Attitudes and Lifestyle Factors in Relation To Oral Health and Dental Care in Sweden A Cross Sectional StudyDocument9 pagesAttitudes and Lifestyle Factors in Relation To Oral Health and Dental Care in Sweden A Cross Sectional Studyasem sardyNo ratings yet
- Main StudyDocument127 pagesMain Studykuruvagadda sagarNo ratings yet
- Exploring The World of Science: Dental Caries: A ReviewDocument5 pagesExploring The World of Science: Dental Caries: A ReviewjulfikaNo ratings yet
- Tooth Wear 1Document11 pagesTooth Wear 1Kcl Knit A SocNo ratings yet
- Dental CariesDocument41 pagesDental Cariescopy smartNo ratings yet
- Early Childhood Caries: Etiology, Clinical Considerations, Consequences and ManagementDocument8 pagesEarly Childhood Caries: Etiology, Clinical Considerations, Consequences and ManagementPetrChalupaNo ratings yet
- Effective Interventions To Prevent Dental Caries in Preschool ChildrenDocument56 pagesEffective Interventions To Prevent Dental Caries in Preschool ChildrenDiego AzaedoNo ratings yet
- Rational Paper-Dental CareDocument11 pagesRational Paper-Dental Careapi-381876980No ratings yet
- Prevalence of Dental Caries Among School Going Children in Mixed Dentition Stage (6 To 15 Years of Age) in The Suburbs Schools of Islamabad, PakistanDocument6 pagesPrevalence of Dental Caries Among School Going Children in Mixed Dentition Stage (6 To 15 Years of Age) in The Suburbs Schools of Islamabad, PakistankajdfaskNo ratings yet
- Editorial June 2016Document3 pagesEditorial June 2016Risha faricha NabilaNo ratings yet
- The of Dental Caries in Children: ManagementDocument8 pagesThe of Dental Caries in Children: Managementسینا ایرانیNo ratings yet
- Black Stains An Update On EtiologiesDocument6 pagesBlack Stains An Update On EtiologiesGhimpu DanielaNo ratings yet
- Clinical E Oral-Health Promotion in Dental Caries Prevention Among Children: Systematic Review and Meta-AnalysisDocument33 pagesClinical E Oral-Health Promotion in Dental Caries Prevention Among Children: Systematic Review and Meta-Analysisnadia syestiNo ratings yet
- Guideline On Caries-Risk Assessment and Management For Infants, Children, and AdolescentsDocument8 pagesGuideline On Caries-Risk Assessment and Management For Infants, Children, and AdolescentsAkaul RukchonNo ratings yet
- Diet, Nutrition, and Prevention of Dental DiseaseDocument26 pagesDiet, Nutrition, and Prevention of Dental DiseaseMuhammad Benny SetiyadiNo ratings yet
- Dental Caries StrategiesDocument23 pagesDental Caries StrategiesCarlos Alberto CastañedaNo ratings yet
- The Global Burden of Oral Diseases and Risks To orDocument10 pagesThe Global Burden of Oral Diseases and Risks To orViviane GodoiNo ratings yet
- Prevalence of Dental Health Problems Among School Going Children in Rural KeralaDocument5 pagesPrevalence of Dental Health Problems Among School Going Children in Rural KeralaPrasun Sit SharmaNo ratings yet
- Modern Thoughts On Fissure SealantsDocument5 pagesModern Thoughts On Fissure SealantsSaca AnastasiaNo ratings yet
- Ijerph 18 11539 v2Document14 pagesIjerph 18 11539 v2Mobolaji Ayowole victorNo ratings yet
- Arabia SaudiDocument7 pagesArabia SaudiKarin SteinmeyerNo ratings yet
- Dentist Question S and AnswersDocument4 pagesDentist Question S and AnswersLangai Elvis NyuyseniNo ratings yet
- Changing Trends in Dental Caries: Aubrey SheihamDocument6 pagesChanging Trends in Dental Caries: Aubrey Sheihamanejadental clinicNo ratings yet
- Association Between Dental Erosion and Diet in Brazilian Adolescents Aged From 15 To 19 - A Population-Based StudyDocument9 pagesAssociation Between Dental Erosion and Diet in Brazilian Adolescents Aged From 15 To 19 - A Population-Based StudyIgnacio PerloNo ratings yet
- Correlation of Caries Prevalence, Oral Health Behavior and Sweets Nutritional Habits Among 10 To 19-Year-Old Cluj-Napoca Romanian AdolescentsDocument12 pagesCorrelation of Caries Prevalence, Oral Health Behavior and Sweets Nutritional Habits Among 10 To 19-Year-Old Cluj-Napoca Romanian AdolescentsSalsasarah AlizaNo ratings yet
- Pediatric Restorative DentistryFrom EverandPediatric Restorative DentistrySoraya Coelho LealNo ratings yet
- Management of Deep Carious LesionsFrom EverandManagement of Deep Carious LesionsFalk SchwendickeNo ratings yet
- Understanding Periodontitis: A Comprehensive Guide to Periodontal Disease for Dentists, Dental Hygienists and Dental PatientsFrom EverandUnderstanding Periodontitis: A Comprehensive Guide to Periodontal Disease for Dentists, Dental Hygienists and Dental PatientsNo ratings yet
- Properties of Dental Materials (PART 5)Document29 pagesProperties of Dental Materials (PART 5)Moona WahabNo ratings yet
- Infection Control LecturDocument62 pagesInfection Control LecturMoona WahabNo ratings yet
- Tooth Numbering SystemDocument28 pagesTooth Numbering SystemMoona WahabNo ratings yet
- 3.classification of DM and RequirementsDocument21 pages3.classification of DM and RequirementsMoona WahabNo ratings yet
- Bacterial, GeneticsDocument21 pagesBacterial, GeneticsMoona WahabNo ratings yet
- Properties of Dental Materials (PART 4)Document13 pagesProperties of Dental Materials (PART 4)Moona WahabNo ratings yet
- Farahwahab Fatimatuzzehra: Prepared byDocument19 pagesFarahwahab Fatimatuzzehra: Prepared byMoona WahabNo ratings yet
- Properties of Dental Materials (Part 8)Document27 pagesProperties of Dental Materials (Part 8)Moona WahabNo ratings yet
- Unit1 D (A2)Document3 pagesUnit1 D (A2)Moona WahabNo ratings yet
- CEMENTs - Doc Version 1Document3 pagesCEMENTs - Doc Version 1Moona WahabNo ratings yet
- 2.3 Leadership and ManagementDocument3 pages2.3 Leadership and ManagementMoona WahabNo ratings yet
- Merit and Demerit GoodsDocument1 pageMerit and Demerit GoodsMoona WahabNo ratings yet
- Production and Cost in The Long RunDocument23 pagesProduction and Cost in The Long RunMoona WahabNo ratings yet
- Syllabus Wise List of Text Books and Reference Books XIDocument1 pageSyllabus Wise List of Text Books and Reference Books XIMoona WahabNo ratings yet
- Sat Sample Test 01Document23 pagesSat Sample Test 01Moona WahabNo ratings yet
- The Resons For Individuals, Organisations and Societies Having To Make ChoicesDocument8 pagesThe Resons For Individuals, Organisations and Societies Having To Make ChoicesMoona WahabNo ratings yet
- WWW - Studyguide.pk: Business GrowthDocument7 pagesWWW - Studyguide.pk: Business GrowthMoona WahabNo ratings yet
- Behavioural Change TheoriesDocument11 pagesBehavioural Change TheoriesMoona WahabNo ratings yet
- Phyto-Nutritional Profiles of Broom Weed (Sida Acuta) Leaf ExtractDocument6 pagesPhyto-Nutritional Profiles of Broom Weed (Sida Acuta) Leaf ExtractresearchparksNo ratings yet
- Nutrition Education: Linking Research, Theory, and Practice: Review ArticleDocument4 pagesNutrition Education: Linking Research, Theory, and Practice: Review ArticleMeitriana PangestutiNo ratings yet
- Physical and Behavioral Development of Laboratory Rats On Modified ConditionsDocument38 pagesPhysical and Behavioral Development of Laboratory Rats On Modified ConditionslisaNo ratings yet
- 5-Day Step Into Fasting Jumpstart (Max Effect Fitness)Document13 pages5-Day Step Into Fasting Jumpstart (Max Effect Fitness)Cypher CryptoNo ratings yet
- Management of Broiler FarmsDocument47 pagesManagement of Broiler FarmssmoubarakNo ratings yet
- 2013 Annual Keysie Ball!: Director's DeskDocument16 pages2013 Annual Keysie Ball!: Director's DeskAaron EdwardsNo ratings yet
- Fisiologi StarvasiDocument47 pagesFisiologi Starvasicynthia maharaniNo ratings yet
- Chapter 6Document11 pagesChapter 6Siamak HeshmatiNo ratings yet
- Effect of Feeding Concentrate Diets Containing Graded Levels of Groundnut Haulms On The Performance of Friesian X Bunaji Cattle PDFDocument224 pagesEffect of Feeding Concentrate Diets Containing Graded Levels of Groundnut Haulms On The Performance of Friesian X Bunaji Cattle PDFmekyno320% (1)
- Digital Unit Plan TemplateDocument4 pagesDigital Unit Plan Templateapi-238672103No ratings yet
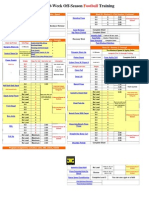
- Workout - Sheet - Football 30-Week Off-Season Training Week20-24Document9 pagesWorkout - Sheet - Football 30-Week Off-Season Training Week20-24Tom HochhalterNo ratings yet
- Kettlebell ProgramDocument1 pageKettlebell ProgramsteNo ratings yet
- Actividad Should-Shouldn't GAFDocument3 pagesActividad Should-Shouldn't GAFAntonio100% (1)
- Fluid and ElectrolytesDocument14 pagesFluid and Electrolytesstring44100% (2)
- 1.starship Troopers: Book vs. MovieDocument6 pages1.starship Troopers: Book vs. MovieThea BaquilarNo ratings yet
- Ethnobotanical and Pharmacological Activity of Arthrospira PlatensisDocument7 pagesEthnobotanical and Pharmacological Activity of Arthrospira PlatensisIJRASETPublicationsNo ratings yet
- kIDS BOOKDocument2 pageskIDS BOOKHassan Tahir SialNo ratings yet
- Umi Fahmida and Otte SantikaDocument8 pagesUmi Fahmida and Otte Santikaston777No ratings yet
- Environmental Diseases, (PowerPoint File)Document49 pagesEnvironmental Diseases, (PowerPoint File)imtiazali2008No ratings yet
- Lesson 1 Physical Fitness Its Meaning and Importance: TargetDocument29 pagesLesson 1 Physical Fitness Its Meaning and Importance: TargetDeth Evangelista100% (1)
- Calcium N JointsDocument12 pagesCalcium N JointsDisha RataniNo ratings yet
- Bodybuilding Routines For Complete RecoveryDocument4 pagesBodybuilding Routines For Complete Recoverybamabob1100% (1)
- LactationDocument11 pagesLactationWan SakinahNo ratings yet
- Midterm Examination in EAPPDocument7 pagesMidterm Examination in EAPPRenee Kristen Tapia100% (1)
- The Nutrition Care Process Related To HypertensionDocument22 pagesThe Nutrition Care Process Related To HypertensionNita SeptianaNo ratings yet
- Summary of ReportDocument13 pagesSummary of ReportCindy Mae CamohoyNo ratings yet
- GB GrowingDocument3 pagesGB GrowingCn SumantNo ratings yet
- The 10 Best Plyometric Exercises For Athletes: 1. Front Box JumpDocument21 pagesThe 10 Best Plyometric Exercises For Athletes: 1. Front Box Jumparmaan100% (1)
- Therapeutic Diets in The ElderlyDocument9 pagesTherapeutic Diets in The ElderlyJoanne Cristie TolopiaNo ratings yet











































































































Download as docx, pdf, or txt
You might also like
- Piper Mike - Surprisingly SimpleDocument54 pagesPiper Mike - Surprisingly SimpleMoona Wahab100% (2)
- MSM GrasDocument84 pagesMSM GrasGopalaKrishnan Sivaraman0% (1)
- Title: Children's Oral Health Strategy in The UKDocument8 pagesTitle: Children's Oral Health Strategy in The UKshahryar eskandarzadeNo ratings yet
- Literature Review On Prevalence of Dental CariesDocument5 pagesLiterature Review On Prevalence of Dental Cariesc5t0jsyn100% (1)
- Snack and ToothbrushingDocument8 pagesSnack and Toothbrushingsandra del pilarNo ratings yet
- Wong 2017Document24 pagesWong 2017Ngoc MinhNo ratings yet
- Dissertation Topics in Community DentistryDocument7 pagesDissertation Topics in Community DentistryOnlinePaperWritingServiceCanada100% (1)
- Almedleg 2021 - Causes N Diagnosis ECC - SRDocument12 pagesAlmedleg 2021 - Causes N Diagnosis ECC - SRDR ANKITA KHADENo ratings yet
- Dental Caries PandemicDocument5 pagesDental Caries PandemicKarla González GNo ratings yet
- Guideline On Caries-Risk Assessment and Management For Infants, Children, and AdolescentsDocument8 pagesGuideline On Caries-Risk Assessment and Management For Infants, Children, and AdolescentsPriscila Belén Chuhuaicura SotoNo ratings yet
- Children: Dental Caries and Oral Health in Children-Special IssueDocument3 pagesChildren: Dental Caries and Oral Health in Children-Special IssuecareNo ratings yet
- Managing C R in Adults: Aries ISKDocument6 pagesManaging C R in Adults: Aries ISKSOMVIR KUMARNo ratings yet
- Caries Temprana de La InfanciaDocument6 pagesCaries Temprana de La InfanciaAna CristernaNo ratings yet
- Jessicaleeliterature Review PaperDocument6 pagesJessicaleeliterature Review Paperapi-725689989No ratings yet
- Caries Risk AssessmentDocument8 pagesCaries Risk AssessmentGrace Shabrina HapsariNo ratings yet
- Foreign LiteratureDocument13 pagesForeign LiteratureJm. n BelNo ratings yet
- Ecc Lit Review - PDocument7 pagesEcc Lit Review - Papi-720438286No ratings yet
- Dental Health AustraliaDocument8 pagesDental Health AustraliajohnmccauleyNo ratings yet
- Comm Dent Oral Epid 2023 SharmaDocument15 pagesComm Dent Oral Epid 2023 SharmaNatalia DavilaNo ratings yet
- Taf PDFDocument14 pagesTaf PDFrania azzahraNo ratings yet
- Public Health Dentistry Thesis TopicsDocument5 pagesPublic Health Dentistry Thesis Topicss0kuzej0byn2100% (2)
- Obesity and Obesity Related Diseases, Sugar Consumption and Bad Oral Health: A Fatal Epidemic MixturesDocument8 pagesObesity and Obesity Related Diseases, Sugar Consumption and Bad Oral Health: A Fatal Epidemic MixturesAyu DamayNo ratings yet
- Sugar Intake and Dental Decay Results From A National Survey of Children in ScotlandDocument10 pagesSugar Intake and Dental Decay Results From A National Survey of Children in ScotlandAndrada IonescuNo ratings yet
- Caries Prevention in School ChildrenDocument12 pagesCaries Prevention in School ChildrenJatan KothariNo ratings yet
- P ProphylaxisDocument5 pagesP ProphylaxisLeticia Quiñonez VivasNo ratings yet
- Library Dissertation On Early Childhood CariesDocument4 pagesLibrary Dissertation On Early Childhood CariesPayToWritePaperBaltimore100% (1)
- Updated BSP BSPD Perio Guidelines For The Under 18s 2021 FINAL 270921 VC PDF VersionDocument45 pagesUpdated BSP BSPD Perio Guidelines For The Under 18s 2021 FINAL 270921 VC PDF VersionhanaNo ratings yet
- JDM 2018 004 Int@081-086Document6 pagesJDM 2018 004 Int@081-086Miguel Ángel De la Cruz GómezNo ratings yet
- Habits and Social Norms Leading To Childhood CariesDocument16 pagesHabits and Social Norms Leading To Childhood Cariesapi-522555065No ratings yet
- Articulo ObeDocument9 pagesArticulo ObedennisNo ratings yet
- Chapter37 - Prevention of Periodontal - Dis94 PDFDocument13 pagesChapter37 - Prevention of Periodontal - Dis94 PDFDana DanielaNo ratings yet
- Guideline On Caries-Risk Assessment and Management For Infants, Children, and AdolescentsDocument8 pagesGuideline On Caries-Risk Assessment and Management For Infants, Children, and AdolescentsShruti SoodNo ratings yet
- Impact of Lifestyle Variables On Oral Diseases and Oral Health-Related Quality of Life in Children of Milan (Italy)Document16 pagesImpact of Lifestyle Variables On Oral Diseases and Oral Health-Related Quality of Life in Children of Milan (Italy)Zarah Hannah Leah DalmacioNo ratings yet
- Attitudes and Lifestyle Factors in Relation To Oral Health and Dental Care in Sweden A Cross Sectional StudyDocument9 pagesAttitudes and Lifestyle Factors in Relation To Oral Health and Dental Care in Sweden A Cross Sectional Studyasem sardyNo ratings yet
- Main StudyDocument127 pagesMain Studykuruvagadda sagarNo ratings yet
- Exploring The World of Science: Dental Caries: A ReviewDocument5 pagesExploring The World of Science: Dental Caries: A ReviewjulfikaNo ratings yet
- Tooth Wear 1Document11 pagesTooth Wear 1Kcl Knit A SocNo ratings yet
- Dental CariesDocument41 pagesDental Cariescopy smartNo ratings yet
- Early Childhood Caries: Etiology, Clinical Considerations, Consequences and ManagementDocument8 pagesEarly Childhood Caries: Etiology, Clinical Considerations, Consequences and ManagementPetrChalupaNo ratings yet
- Effective Interventions To Prevent Dental Caries in Preschool ChildrenDocument56 pagesEffective Interventions To Prevent Dental Caries in Preschool ChildrenDiego AzaedoNo ratings yet
- Rational Paper-Dental CareDocument11 pagesRational Paper-Dental Careapi-381876980No ratings yet
- Prevalence of Dental Caries Among School Going Children in Mixed Dentition Stage (6 To 15 Years of Age) in The Suburbs Schools of Islamabad, PakistanDocument6 pagesPrevalence of Dental Caries Among School Going Children in Mixed Dentition Stage (6 To 15 Years of Age) in The Suburbs Schools of Islamabad, PakistankajdfaskNo ratings yet
- Editorial June 2016Document3 pagesEditorial June 2016Risha faricha NabilaNo ratings yet
- The of Dental Caries in Children: ManagementDocument8 pagesThe of Dental Caries in Children: Managementسینا ایرانیNo ratings yet
- Black Stains An Update On EtiologiesDocument6 pagesBlack Stains An Update On EtiologiesGhimpu DanielaNo ratings yet
- Clinical E Oral-Health Promotion in Dental Caries Prevention Among Children: Systematic Review and Meta-AnalysisDocument33 pagesClinical E Oral-Health Promotion in Dental Caries Prevention Among Children: Systematic Review and Meta-Analysisnadia syestiNo ratings yet
- Guideline On Caries-Risk Assessment and Management For Infants, Children, and AdolescentsDocument8 pagesGuideline On Caries-Risk Assessment and Management For Infants, Children, and AdolescentsAkaul RukchonNo ratings yet
- Diet, Nutrition, and Prevention of Dental DiseaseDocument26 pagesDiet, Nutrition, and Prevention of Dental DiseaseMuhammad Benny SetiyadiNo ratings yet
- Dental Caries StrategiesDocument23 pagesDental Caries StrategiesCarlos Alberto CastañedaNo ratings yet
- The Global Burden of Oral Diseases and Risks To orDocument10 pagesThe Global Burden of Oral Diseases and Risks To orViviane GodoiNo ratings yet
- Prevalence of Dental Health Problems Among School Going Children in Rural KeralaDocument5 pagesPrevalence of Dental Health Problems Among School Going Children in Rural KeralaPrasun Sit SharmaNo ratings yet
- Modern Thoughts On Fissure SealantsDocument5 pagesModern Thoughts On Fissure SealantsSaca AnastasiaNo ratings yet
- Ijerph 18 11539 v2Document14 pagesIjerph 18 11539 v2Mobolaji Ayowole victorNo ratings yet
- Arabia SaudiDocument7 pagesArabia SaudiKarin SteinmeyerNo ratings yet
- Dentist Question S and AnswersDocument4 pagesDentist Question S and AnswersLangai Elvis NyuyseniNo ratings yet
- Changing Trends in Dental Caries: Aubrey SheihamDocument6 pagesChanging Trends in Dental Caries: Aubrey Sheihamanejadental clinicNo ratings yet
- Association Between Dental Erosion and Diet in Brazilian Adolescents Aged From 15 To 19 - A Population-Based StudyDocument9 pagesAssociation Between Dental Erosion and Diet in Brazilian Adolescents Aged From 15 To 19 - A Population-Based StudyIgnacio PerloNo ratings yet
- Correlation of Caries Prevalence, Oral Health Behavior and Sweets Nutritional Habits Among 10 To 19-Year-Old Cluj-Napoca Romanian AdolescentsDocument12 pagesCorrelation of Caries Prevalence, Oral Health Behavior and Sweets Nutritional Habits Among 10 To 19-Year-Old Cluj-Napoca Romanian AdolescentsSalsasarah AlizaNo ratings yet
- Pediatric Restorative DentistryFrom EverandPediatric Restorative DentistrySoraya Coelho LealNo ratings yet
- Management of Deep Carious LesionsFrom EverandManagement of Deep Carious LesionsFalk SchwendickeNo ratings yet
- Understanding Periodontitis: A Comprehensive Guide to Periodontal Disease for Dentists, Dental Hygienists and Dental PatientsFrom EverandUnderstanding Periodontitis: A Comprehensive Guide to Periodontal Disease for Dentists, Dental Hygienists and Dental PatientsNo ratings yet
- Properties of Dental Materials (PART 5)Document29 pagesProperties of Dental Materials (PART 5)Moona WahabNo ratings yet
- Infection Control LecturDocument62 pagesInfection Control LecturMoona WahabNo ratings yet
- Tooth Numbering SystemDocument28 pagesTooth Numbering SystemMoona WahabNo ratings yet
- 3.classification of DM and RequirementsDocument21 pages3.classification of DM and RequirementsMoona WahabNo ratings yet
- Bacterial, GeneticsDocument21 pagesBacterial, GeneticsMoona WahabNo ratings yet
- Properties of Dental Materials (PART 4)Document13 pagesProperties of Dental Materials (PART 4)Moona WahabNo ratings yet
- Farahwahab Fatimatuzzehra: Prepared byDocument19 pagesFarahwahab Fatimatuzzehra: Prepared byMoona WahabNo ratings yet
- Properties of Dental Materials (Part 8)Document27 pagesProperties of Dental Materials (Part 8)Moona WahabNo ratings yet
- Unit1 D (A2)Document3 pagesUnit1 D (A2)Moona WahabNo ratings yet
- CEMENTs - Doc Version 1Document3 pagesCEMENTs - Doc Version 1Moona WahabNo ratings yet
- 2.3 Leadership and ManagementDocument3 pages2.3 Leadership and ManagementMoona WahabNo ratings yet
- Merit and Demerit GoodsDocument1 pageMerit and Demerit GoodsMoona WahabNo ratings yet
- Production and Cost in The Long RunDocument23 pagesProduction and Cost in The Long RunMoona WahabNo ratings yet
- Syllabus Wise List of Text Books and Reference Books XIDocument1 pageSyllabus Wise List of Text Books and Reference Books XIMoona WahabNo ratings yet
- Sat Sample Test 01Document23 pagesSat Sample Test 01Moona WahabNo ratings yet
- The Resons For Individuals, Organisations and Societies Having To Make ChoicesDocument8 pagesThe Resons For Individuals, Organisations and Societies Having To Make ChoicesMoona WahabNo ratings yet
- WWW - Studyguide.pk: Business GrowthDocument7 pagesWWW - Studyguide.pk: Business GrowthMoona WahabNo ratings yet
- Behavioural Change TheoriesDocument11 pagesBehavioural Change TheoriesMoona WahabNo ratings yet
- Phyto-Nutritional Profiles of Broom Weed (Sida Acuta) Leaf ExtractDocument6 pagesPhyto-Nutritional Profiles of Broom Weed (Sida Acuta) Leaf ExtractresearchparksNo ratings yet
- Nutrition Education: Linking Research, Theory, and Practice: Review ArticleDocument4 pagesNutrition Education: Linking Research, Theory, and Practice: Review ArticleMeitriana PangestutiNo ratings yet
- Physical and Behavioral Development of Laboratory Rats On Modified ConditionsDocument38 pagesPhysical and Behavioral Development of Laboratory Rats On Modified ConditionslisaNo ratings yet
- 5-Day Step Into Fasting Jumpstart (Max Effect Fitness)Document13 pages5-Day Step Into Fasting Jumpstart (Max Effect Fitness)Cypher CryptoNo ratings yet
- Management of Broiler FarmsDocument47 pagesManagement of Broiler FarmssmoubarakNo ratings yet
- 2013 Annual Keysie Ball!: Director's DeskDocument16 pages2013 Annual Keysie Ball!: Director's DeskAaron EdwardsNo ratings yet
- Fisiologi StarvasiDocument47 pagesFisiologi Starvasicynthia maharaniNo ratings yet
- Chapter 6Document11 pagesChapter 6Siamak HeshmatiNo ratings yet
- Effect of Feeding Concentrate Diets Containing Graded Levels of Groundnut Haulms On The Performance of Friesian X Bunaji Cattle PDFDocument224 pagesEffect of Feeding Concentrate Diets Containing Graded Levels of Groundnut Haulms On The Performance of Friesian X Bunaji Cattle PDFmekyno320% (1)
- Digital Unit Plan TemplateDocument4 pagesDigital Unit Plan Templateapi-238672103No ratings yet
- Workout - Sheet - Football 30-Week Off-Season Training Week20-24Document9 pagesWorkout - Sheet - Football 30-Week Off-Season Training Week20-24Tom HochhalterNo ratings yet
- Kettlebell ProgramDocument1 pageKettlebell ProgramsteNo ratings yet
- Actividad Should-Shouldn't GAFDocument3 pagesActividad Should-Shouldn't GAFAntonio100% (1)
- Fluid and ElectrolytesDocument14 pagesFluid and Electrolytesstring44100% (2)
- 1.starship Troopers: Book vs. MovieDocument6 pages1.starship Troopers: Book vs. MovieThea BaquilarNo ratings yet
- Ethnobotanical and Pharmacological Activity of Arthrospira PlatensisDocument7 pagesEthnobotanical and Pharmacological Activity of Arthrospira PlatensisIJRASETPublicationsNo ratings yet
- kIDS BOOKDocument2 pageskIDS BOOKHassan Tahir SialNo ratings yet
- Umi Fahmida and Otte SantikaDocument8 pagesUmi Fahmida and Otte Santikaston777No ratings yet
- Environmental Diseases, (PowerPoint File)Document49 pagesEnvironmental Diseases, (PowerPoint File)imtiazali2008No ratings yet
- Lesson 1 Physical Fitness Its Meaning and Importance: TargetDocument29 pagesLesson 1 Physical Fitness Its Meaning and Importance: TargetDeth Evangelista100% (1)
- Calcium N JointsDocument12 pagesCalcium N JointsDisha RataniNo ratings yet
- Bodybuilding Routines For Complete RecoveryDocument4 pagesBodybuilding Routines For Complete Recoverybamabob1100% (1)
- LactationDocument11 pagesLactationWan SakinahNo ratings yet
- Midterm Examination in EAPPDocument7 pagesMidterm Examination in EAPPRenee Kristen Tapia100% (1)
- The Nutrition Care Process Related To HypertensionDocument22 pagesThe Nutrition Care Process Related To HypertensionNita SeptianaNo ratings yet
- Summary of ReportDocument13 pagesSummary of ReportCindy Mae CamohoyNo ratings yet
- GB GrowingDocument3 pagesGB GrowingCn SumantNo ratings yet
- The 10 Best Plyometric Exercises For Athletes: 1. Front Box JumpDocument21 pagesThe 10 Best Plyometric Exercises For Athletes: 1. Front Box Jumparmaan100% (1)
- Therapeutic Diets in The ElderlyDocument9 pagesTherapeutic Diets in The ElderlyJoanne Cristie TolopiaNo ratings yet