
Overweight and Obesity: The Significance of A Depressed Mood
Overweight and Obesity: The Significance of A Depressed Mood
You might also like
- PM-3000 Section 1 To 7 ManualDocument52 pagesPM-3000 Section 1 To 7 Manualpablo100% (1)
- The Non-Diet Approach Guidebook for Dietitians (2013): A how-to guide for applying the Non-Diet Approach to Individualised Dietetic CounsellingFrom EverandThe Non-Diet Approach Guidebook for Dietitians (2013): A how-to guide for applying the Non-Diet Approach to Individualised Dietetic CounsellingNo ratings yet
- Cognitive Behavior Therapy For Patients With Diabetes and DepressionDocument11 pagesCognitive Behavior Therapy For Patients With Diabetes and DepressionmaidaNo ratings yet
- Final Research Presentation 1Document14 pagesFinal Research Presentation 1api-298607729No ratings yet
- Diabetes Distress Journal Review FINAL 2Document12 pagesDiabetes Distress Journal Review FINAL 2ZeroNine. TvNo ratings yet
- Review Journal 4Document14 pagesReview Journal 4Debby Syahru RomadlonNo ratings yet
- Research ProposalDocument22 pagesResearch Proposalapi-662212007No ratings yet
- Gibson Smith2018Document19 pagesGibson Smith2018Romeo IsaíasNo ratings yet
- Diet Quality in Persons With and Without Depressiv 2018 Journal of PsychiatrDocument7 pagesDiet Quality in Persons With and Without Depressiv 2018 Journal of Psychiatrgiulia.santinNo ratings yet
- Depression Among Diabetes Mellitus Patients: A Study of The Protective FactorsDocument6 pagesDepression Among Diabetes Mellitus Patients: A Study of The Protective FactorsIJPHSNo ratings yet
- Eating Disorder Effect Mental Health in PeopleDocument9 pagesEating Disorder Effect Mental Health in Peopleshizaarshad125No ratings yet
- Diabetik Dan KelainannyaDocument11 pagesDiabetik Dan Kelainannyalatifah zahrohNo ratings yet
- ST2 1.1.3 Noroozi, Et Al. 2017Document7 pagesST2 1.1.3 Noroozi, Et Al. 2017JemarcusNo ratings yet
- Diabetic Medicine - 2017 - Perrin - The Prevalence of Diabetes Specific Emotional Distress in People With Type 2 DiabetesDocument13 pagesDiabetic Medicine - 2017 - Perrin - The Prevalence of Diabetes Specific Emotional Distress in People With Type 2 Diabetesnirmala amirNo ratings yet
- Nutrients 09 01274Document11 pagesNutrients 09 01274Luisa BragançaNo ratings yet
- Anxiety-Depressive Disorders Among Irritable Bowel Syndrome Patients in Guilan, IranDocument7 pagesAnxiety-Depressive Disorders Among Irritable Bowel Syndrome Patients in Guilan, Iranapi-193771047No ratings yet
- Caregivers Consequences of Care Among Patients With Eating DisordersDocument10 pagesCaregivers Consequences of Care Among Patients With Eating DisordersVictoria PazNo ratings yet
- Alabi2018 Article DepressionBeforeAndAfterBariatDocument7 pagesAlabi2018 Article DepressionBeforeAndAfterBariatFrancisco TNo ratings yet
- A Randomised Controlled Trial of Dietary Improvement For Adults With Major Depression (The SMILES' Trial)Document13 pagesA Randomised Controlled Trial of Dietary Improvement For Adults With Major Depression (The SMILES' Trial)agalbimaNo ratings yet
- 128 FullDocument9 pages128 FullAhtarunnisa Fauzia HanifaNo ratings yet
- Diet in DepressionDocument7 pagesDiet in Depressionanwaarft123No ratings yet
- Alliance Matters But How Much A Systematic Review On Therapeutic Alliance and Outcome in Patients With Anorexia Nervosa and Bulimia NervosaDocument17 pagesAlliance Matters But How Much A Systematic Review On Therapeutic Alliance and Outcome in Patients With Anorexia Nervosa and Bulimia NervosaMario VillegasNo ratings yet
- MBSR For Chronic IllnessDocument5 pagesMBSR For Chronic IllnessYudith LouisaNo ratings yet
- Nuevos Tratamientos TCA SeverosDocument10 pagesNuevos Tratamientos TCA SeverosfranciscaikaNo ratings yet
- Binge-Eating Disorder in AdultsDocument19 pagesBinge-Eating Disorder in AdultsJaimeErGañanNo ratings yet
- Jackson2016 Well-Being in Chronic Fatigue SyndromeDocument11 pagesJackson2016 Well-Being in Chronic Fatigue SyndromeEszter BogádiNo ratings yet
- Diabetes and DepresiDocument218 pagesDiabetes and DepresiDaslan ToruntjuNo ratings yet
- Caluza, Zhyraine Iraj D. 1Document6 pagesCaluza, Zhyraine Iraj D. 1Zhyraine Iraj D. CaluzaNo ratings yet
- The Impact of Bariatric Surgery On DepressionDocument5 pagesThe Impact of Bariatric Surgery On DepressionSileimarNo ratings yet
- Jurnal Inggris 3Document10 pagesJurnal Inggris 3Mr. FernandoNo ratings yet
- Journal of Psychosomatic ResearchDocument6 pagesJournal of Psychosomatic ResearchAryaldy ZulkarnainiNo ratings yet
- Andersen Et Al (2010)Document7 pagesAndersen Et Al (2010)Justin Álvarez ZamoraNo ratings yet
- Reducing Diabetes Burnout Syndrome Using Self-Instructional TrainingDocument6 pagesReducing Diabetes Burnout Syndrome Using Self-Instructional TrainingIJPHSNo ratings yet
- Biopsychosocial Model of HealthDocument10 pagesBiopsychosocial Model of HealthDavin DoNo ratings yet
- AbstracteDocument4 pagesAbstractegrymberg5No ratings yet
- General Hospital Psychiatry: SciencedirectDocument8 pagesGeneral Hospital Psychiatry: SciencedirectFranciscoNo ratings yet
- Controlling Binge Eating and Weight A TRDocument5 pagesControlling Binge Eating and Weight A TRpsico.antonieliNo ratings yet
- IMPACT SummaryDocument17 pagesIMPACT SummaryinfojugamosjuntosNo ratings yet
- Is Cognitive Behavioural Therapy Focusing On Depression and Anxiety Effective For People With Long-Term Physical Health ConditionsDocument19 pagesIs Cognitive Behavioural Therapy Focusing On Depression and Anxiety Effective For People With Long-Term Physical Health ConditionsZhafirah SalsabilaNo ratings yet
- Nutrients: Different Facets of Body Image Disturbance in Binge Eating Disorder: A ReviewDocument24 pagesNutrients: Different Facets of Body Image Disturbance in Binge Eating Disorder: A ReviewSindy ChavarroNo ratings yet
- Case Study - Depression PDFDocument6 pagesCase Study - Depression PDFxiejie22590No ratings yet
- 2015 Article 118Document14 pages2015 Article 118Denisse DelgadoNo ratings yet
- Environmental Research and Public Health: International Journal ofDocument17 pagesEnvironmental Research and Public Health: International Journal ofNatalia BettancourtNo ratings yet
- HLTH 499Document7 pagesHLTH 499api-625956578No ratings yet
- Report About Individual WorkDocument2 pagesReport About Individual WorkМаша МихноNo ratings yet
- New Treatment Approaches For Severe and PDFDocument10 pagesNew Treatment Approaches For Severe and PDFlauraNo ratings yet
- Grilo, Reas y Mitchell 2016Document11 pagesGrilo, Reas y Mitchell 2016lauramarin25No ratings yet
- IndianJEndocrMetab Diabetes y Trastornos MentalesDocument4 pagesIndianJEndocrMetab Diabetes y Trastornos MentalesFran UlNo ratings yet
- Depression, Anxiety, and Stress Levels in Patients With Type 2 Diabetes MellitusDocument3 pagesDepression, Anxiety, and Stress Levels in Patients With Type 2 Diabetes MellitusMarturia DrifanyNo ratings yet
- 10 11648 J Ajpn 20170504 11 PDFDocument5 pages10 11648 J Ajpn 20170504 11 PDFAsti DwiningsihNo ratings yet
- Role of Anxiety, Depression and Anger in Eating Disorders-Structural ModelDocument5 pagesRole of Anxiety, Depression and Anger in Eating Disorders-Structural ModelAsti DwiningsihNo ratings yet
- Physiotherapy Improves Eating Disorders and Quality of Life in Bulimia and Anorexia NervosaDocument3 pagesPhysiotherapy Improves Eating Disorders and Quality of Life in Bulimia and Anorexia NervosaAzul MarinoNo ratings yet
- Mindfulness Training in A Heterogeneous Psychiatric Sample: Outcome Evaluation and Comparison of Different Diagnostic GroupsDocument13 pagesMindfulness Training in A Heterogeneous Psychiatric Sample: Outcome Evaluation and Comparison of Different Diagnostic Groups290971No ratings yet
- Gastrointestinal Symptoms in Primary Care Prevalence and Association With Depression and AnxietyDocument8 pagesGastrointestinal Symptoms in Primary Care Prevalence and Association With Depression and AnxietyJuan Carlos LrNo ratings yet
- RetrieveDocument12 pagesRetrieveAyla CoberoNo ratings yet
- Illness Perceptions Mediate The Relationship Between Bowel Symptom Severity and Health-Related Quality of Life in IBS PatientsDocument12 pagesIllness Perceptions Mediate The Relationship Between Bowel Symptom Severity and Health-Related Quality of Life in IBS Patientsapi-193771047No ratings yet
- The Confidence in Diabetes Self-Care Scale (Adultos) (Alemania y USA)Document6 pagesThe Confidence in Diabetes Self-Care Scale (Adultos) (Alemania y USA)Verónica MelgarejoNo ratings yet
- Pokrajac-Bulian2015 Article QualityOfLifeAsAMediatorInTheADocument9 pagesPokrajac-Bulian2015 Article QualityOfLifeAsAMediatorInTheAAisah indrawatiNo ratings yet
- Engelmann 2021Document14 pagesEngelmann 2021Julivert JasminNo ratings yet
- Depression Medication Author: Jerry L Halverson, MD Chief Editor: David Bienenfeld, MD Practice EssentialsDocument128 pagesDepression Medication Author: Jerry L Halverson, MD Chief Editor: David Bienenfeld, MD Practice EssentialsLauria Cindika SariNo ratings yet
- Mindfulness Therapy For Somatization Disorder and Functional Somatic Syndromes - Randomized Trial With One-Year Follow-UpDocument10 pagesMindfulness Therapy For Somatization Disorder and Functional Somatic Syndromes - Randomized Trial With One-Year Follow-UpHelena AlessiNo ratings yet
- The Stiff Elbow: Review Articles of TopicsDocument12 pagesThe Stiff Elbow: Review Articles of TopicsArif Kurniawan ListiantoNo ratings yet
- Jurnal JkmsDocument8 pagesJurnal JkmsArif Kurniawan ListiantoNo ratings yet
- Jurnal4Body Mass Index and Depressive Symptoms in Older AdultsDocument14 pagesJurnal4Body Mass Index and Depressive Symptoms in Older AdultsArif Kurniawan ListiantoNo ratings yet
- CognitipDocument2 pagesCognitipArif Kurniawan ListiantoNo ratings yet
- 1689920643.neko-Eclipse17 Freedom RoadDocument8 pages1689920643.neko-Eclipse17 Freedom RoadAdam NelonNo ratings yet
- Madam Butterfly (Okusama Chou) - Erotic PoetryDocument22 pagesMadam Butterfly (Okusama Chou) - Erotic PoetrygamahucherNo ratings yet
- 2 Changing Our Vision From Material Outlook To Spiritual Outlook PDFDocument4 pages2 Changing Our Vision From Material Outlook To Spiritual Outlook PDFvarun7salunkheNo ratings yet
- Eti 1980 01 80Document124 pagesEti 1980 01 80Adiel RicciNo ratings yet
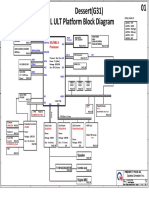
- Quanta G31a Dag31amb6d0 Y61x-6l Rev 1aDocument49 pagesQuanta G31a Dag31amb6d0 Y61x-6l Rev 1aKrystian PalaciosNo ratings yet
- Electrical Conductivity of Aqueous SolutionsDocument1 pageElectrical Conductivity of Aqueous SolutionsTing-Ting PanNo ratings yet
- AC 43.13-1B Section 5 Penetrant InspectionDocument8 pagesAC 43.13-1B Section 5 Penetrant Inspection320338100% (1)
- DMSCO Log Book Vol.8 6/1930-5/1931Document49 pagesDMSCO Log Book Vol.8 6/1930-5/1931Des Moines University Archives and Rare Book RoomNo ratings yet
- Техническая документация B2412S-1WR2 PDFDocument6 pagesТехническая документация B2412S-1WR2 PDFИльнур ТагировNo ratings yet
- Anti-Inflammatory and Analgesic Activities of Flavonoid and Saponin Fractions From Zizyphus Lotus (L.) LamDocument5 pagesAnti-Inflammatory and Analgesic Activities of Flavonoid and Saponin Fractions From Zizyphus Lotus (L.) LamDaris UntoroNo ratings yet
- Sohbi Kohgei - Solar Power System Proposal (Toshiba325W)Document4 pagesSohbi Kohgei - Solar Power System Proposal (Toshiba325W)Jeffcaster ComelNo ratings yet
- Fess 102Document13 pagesFess 102Shivani YadavNo ratings yet
- Han Longyu 200322255 MASC PSE Fall2015 PDFDocument139 pagesHan Longyu 200322255 MASC PSE Fall2015 PDFnajib amienNo ratings yet
- Brochure Compressor Series MX 600Document2 pagesBrochure Compressor Series MX 600Samir ShahNo ratings yet
- CG-Full-Note For PU PDFDocument77 pagesCG-Full-Note For PU PDFirusha0% (1)
- TB Chapter1Document3 pagesTB Chapter1fayeNo ratings yet
- PowerSuite 03 Dec 2018 Recommended Generator Report (EGY 057VET 0238)Document1 pagePowerSuite 03 Dec 2018 Recommended Generator Report (EGY 057VET 0238)Andres BetancourtNo ratings yet
- Q-PCF-12-30-PN 6Document1 pageQ-PCF-12-30-PN 6Camilo Maya PodestaNo ratings yet
- Product News: Cat C12 ACERT™ Marine Propulsion EngineDocument6 pagesProduct News: Cat C12 ACERT™ Marine Propulsion EnginericardoNo ratings yet
- Lecture 11 Energy Transport With Energy DissipationDocument16 pagesLecture 11 Energy Transport With Energy DissipationFarahin Burhan100% (1)
- Published Article 2Document17 pagesPublished Article 2Bharathi RajaNo ratings yet
- Types of PelvisDocument23 pagesTypes of PelvisChinju Jose SajithNo ratings yet
- Systems of Alternate Current Motors and Transformers / TeslaDocument20 pagesSystems of Alternate Current Motors and Transformers / Teslaalexis.testrfNo ratings yet
- Automotive Rubber Spare Parts and Rubber-to-Metal Bonded PartsDocument14 pagesAutomotive Rubber Spare Parts and Rubber-to-Metal Bonded PartsПавел СкорецNo ratings yet
- T.E. (2019 Pattern) Insem Exam. Timetable For March-April-2024Document13 pagesT.E. (2019 Pattern) Insem Exam. Timetable For March-April-2024rauthrishikesh009No ratings yet
- LX - Advance Diploma in Medical Laboratory TechnologyDocument62 pagesLX - Advance Diploma in Medical Laboratory TechnologyGopal Ghuge RawsahebNo ratings yet
- Modeling and Simulation of A Distillation Column Using MatlabDocument15 pagesModeling and Simulation of A Distillation Column Using Matlabrajtharun48No ratings yet
- Package FaultsDocument6 pagesPackage FaultsArunraj Arumugam100% (1)
- 2022 Damat (Co Author) Kajian Aktivitas Antioksidan Mi BasahDocument15 pages2022 Damat (Co Author) Kajian Aktivitas Antioksidan Mi BasahDamatNo ratings yet




























































































Download as pdf or txt
You might also like
- PM-3000 Section 1 To 7 ManualDocument52 pagesPM-3000 Section 1 To 7 Manualpablo100% (1)
- The Non-Diet Approach Guidebook for Dietitians (2013): A how-to guide for applying the Non-Diet Approach to Individualised Dietetic CounsellingFrom EverandThe Non-Diet Approach Guidebook for Dietitians (2013): A how-to guide for applying the Non-Diet Approach to Individualised Dietetic CounsellingNo ratings yet
- Cognitive Behavior Therapy For Patients With Diabetes and DepressionDocument11 pagesCognitive Behavior Therapy For Patients With Diabetes and DepressionmaidaNo ratings yet
- Final Research Presentation 1Document14 pagesFinal Research Presentation 1api-298607729No ratings yet
- Diabetes Distress Journal Review FINAL 2Document12 pagesDiabetes Distress Journal Review FINAL 2ZeroNine. TvNo ratings yet
- Review Journal 4Document14 pagesReview Journal 4Debby Syahru RomadlonNo ratings yet
- Research ProposalDocument22 pagesResearch Proposalapi-662212007No ratings yet
- Gibson Smith2018Document19 pagesGibson Smith2018Romeo IsaíasNo ratings yet
- Diet Quality in Persons With and Without Depressiv 2018 Journal of PsychiatrDocument7 pagesDiet Quality in Persons With and Without Depressiv 2018 Journal of Psychiatrgiulia.santinNo ratings yet
- Depression Among Diabetes Mellitus Patients: A Study of The Protective FactorsDocument6 pagesDepression Among Diabetes Mellitus Patients: A Study of The Protective FactorsIJPHSNo ratings yet
- Eating Disorder Effect Mental Health in PeopleDocument9 pagesEating Disorder Effect Mental Health in Peopleshizaarshad125No ratings yet
- Diabetik Dan KelainannyaDocument11 pagesDiabetik Dan Kelainannyalatifah zahrohNo ratings yet
- ST2 1.1.3 Noroozi, Et Al. 2017Document7 pagesST2 1.1.3 Noroozi, Et Al. 2017JemarcusNo ratings yet
- Diabetic Medicine - 2017 - Perrin - The Prevalence of Diabetes Specific Emotional Distress in People With Type 2 DiabetesDocument13 pagesDiabetic Medicine - 2017 - Perrin - The Prevalence of Diabetes Specific Emotional Distress in People With Type 2 Diabetesnirmala amirNo ratings yet
- Nutrients 09 01274Document11 pagesNutrients 09 01274Luisa BragançaNo ratings yet
- Anxiety-Depressive Disorders Among Irritable Bowel Syndrome Patients in Guilan, IranDocument7 pagesAnxiety-Depressive Disorders Among Irritable Bowel Syndrome Patients in Guilan, Iranapi-193771047No ratings yet
- Caregivers Consequences of Care Among Patients With Eating DisordersDocument10 pagesCaregivers Consequences of Care Among Patients With Eating DisordersVictoria PazNo ratings yet
- Alabi2018 Article DepressionBeforeAndAfterBariatDocument7 pagesAlabi2018 Article DepressionBeforeAndAfterBariatFrancisco TNo ratings yet
- A Randomised Controlled Trial of Dietary Improvement For Adults With Major Depression (The SMILES' Trial)Document13 pagesA Randomised Controlled Trial of Dietary Improvement For Adults With Major Depression (The SMILES' Trial)agalbimaNo ratings yet
- 128 FullDocument9 pages128 FullAhtarunnisa Fauzia HanifaNo ratings yet
- Diet in DepressionDocument7 pagesDiet in Depressionanwaarft123No ratings yet
- Alliance Matters But How Much A Systematic Review On Therapeutic Alliance and Outcome in Patients With Anorexia Nervosa and Bulimia NervosaDocument17 pagesAlliance Matters But How Much A Systematic Review On Therapeutic Alliance and Outcome in Patients With Anorexia Nervosa and Bulimia NervosaMario VillegasNo ratings yet
- MBSR For Chronic IllnessDocument5 pagesMBSR For Chronic IllnessYudith LouisaNo ratings yet
- Nuevos Tratamientos TCA SeverosDocument10 pagesNuevos Tratamientos TCA SeverosfranciscaikaNo ratings yet
- Binge-Eating Disorder in AdultsDocument19 pagesBinge-Eating Disorder in AdultsJaimeErGañanNo ratings yet
- Jackson2016 Well-Being in Chronic Fatigue SyndromeDocument11 pagesJackson2016 Well-Being in Chronic Fatigue SyndromeEszter BogádiNo ratings yet
- Diabetes and DepresiDocument218 pagesDiabetes and DepresiDaslan ToruntjuNo ratings yet
- Caluza, Zhyraine Iraj D. 1Document6 pagesCaluza, Zhyraine Iraj D. 1Zhyraine Iraj D. CaluzaNo ratings yet
- The Impact of Bariatric Surgery On DepressionDocument5 pagesThe Impact of Bariatric Surgery On DepressionSileimarNo ratings yet
- Jurnal Inggris 3Document10 pagesJurnal Inggris 3Mr. FernandoNo ratings yet
- Journal of Psychosomatic ResearchDocument6 pagesJournal of Psychosomatic ResearchAryaldy ZulkarnainiNo ratings yet
- Andersen Et Al (2010)Document7 pagesAndersen Et Al (2010)Justin Álvarez ZamoraNo ratings yet
- Reducing Diabetes Burnout Syndrome Using Self-Instructional TrainingDocument6 pagesReducing Diabetes Burnout Syndrome Using Self-Instructional TrainingIJPHSNo ratings yet
- Biopsychosocial Model of HealthDocument10 pagesBiopsychosocial Model of HealthDavin DoNo ratings yet
- AbstracteDocument4 pagesAbstractegrymberg5No ratings yet
- General Hospital Psychiatry: SciencedirectDocument8 pagesGeneral Hospital Psychiatry: SciencedirectFranciscoNo ratings yet
- Controlling Binge Eating and Weight A TRDocument5 pagesControlling Binge Eating and Weight A TRpsico.antonieliNo ratings yet
- IMPACT SummaryDocument17 pagesIMPACT SummaryinfojugamosjuntosNo ratings yet
- Is Cognitive Behavioural Therapy Focusing On Depression and Anxiety Effective For People With Long-Term Physical Health ConditionsDocument19 pagesIs Cognitive Behavioural Therapy Focusing On Depression and Anxiety Effective For People With Long-Term Physical Health ConditionsZhafirah SalsabilaNo ratings yet
- Nutrients: Different Facets of Body Image Disturbance in Binge Eating Disorder: A ReviewDocument24 pagesNutrients: Different Facets of Body Image Disturbance in Binge Eating Disorder: A ReviewSindy ChavarroNo ratings yet
- Case Study - Depression PDFDocument6 pagesCase Study - Depression PDFxiejie22590No ratings yet
- 2015 Article 118Document14 pages2015 Article 118Denisse DelgadoNo ratings yet
- Environmental Research and Public Health: International Journal ofDocument17 pagesEnvironmental Research and Public Health: International Journal ofNatalia BettancourtNo ratings yet
- HLTH 499Document7 pagesHLTH 499api-625956578No ratings yet
- Report About Individual WorkDocument2 pagesReport About Individual WorkМаша МихноNo ratings yet
- New Treatment Approaches For Severe and PDFDocument10 pagesNew Treatment Approaches For Severe and PDFlauraNo ratings yet
- Grilo, Reas y Mitchell 2016Document11 pagesGrilo, Reas y Mitchell 2016lauramarin25No ratings yet
- IndianJEndocrMetab Diabetes y Trastornos MentalesDocument4 pagesIndianJEndocrMetab Diabetes y Trastornos MentalesFran UlNo ratings yet
- Depression, Anxiety, and Stress Levels in Patients With Type 2 Diabetes MellitusDocument3 pagesDepression, Anxiety, and Stress Levels in Patients With Type 2 Diabetes MellitusMarturia DrifanyNo ratings yet
- 10 11648 J Ajpn 20170504 11 PDFDocument5 pages10 11648 J Ajpn 20170504 11 PDFAsti DwiningsihNo ratings yet
- Role of Anxiety, Depression and Anger in Eating Disorders-Structural ModelDocument5 pagesRole of Anxiety, Depression and Anger in Eating Disorders-Structural ModelAsti DwiningsihNo ratings yet
- Physiotherapy Improves Eating Disorders and Quality of Life in Bulimia and Anorexia NervosaDocument3 pagesPhysiotherapy Improves Eating Disorders and Quality of Life in Bulimia and Anorexia NervosaAzul MarinoNo ratings yet
- Mindfulness Training in A Heterogeneous Psychiatric Sample: Outcome Evaluation and Comparison of Different Diagnostic GroupsDocument13 pagesMindfulness Training in A Heterogeneous Psychiatric Sample: Outcome Evaluation and Comparison of Different Diagnostic Groups290971No ratings yet
- Gastrointestinal Symptoms in Primary Care Prevalence and Association With Depression and AnxietyDocument8 pagesGastrointestinal Symptoms in Primary Care Prevalence and Association With Depression and AnxietyJuan Carlos LrNo ratings yet
- RetrieveDocument12 pagesRetrieveAyla CoberoNo ratings yet
- Illness Perceptions Mediate The Relationship Between Bowel Symptom Severity and Health-Related Quality of Life in IBS PatientsDocument12 pagesIllness Perceptions Mediate The Relationship Between Bowel Symptom Severity and Health-Related Quality of Life in IBS Patientsapi-193771047No ratings yet
- The Confidence in Diabetes Self-Care Scale (Adultos) (Alemania y USA)Document6 pagesThe Confidence in Diabetes Self-Care Scale (Adultos) (Alemania y USA)Verónica MelgarejoNo ratings yet
- Pokrajac-Bulian2015 Article QualityOfLifeAsAMediatorInTheADocument9 pagesPokrajac-Bulian2015 Article QualityOfLifeAsAMediatorInTheAAisah indrawatiNo ratings yet
- Engelmann 2021Document14 pagesEngelmann 2021Julivert JasminNo ratings yet
- Depression Medication Author: Jerry L Halverson, MD Chief Editor: David Bienenfeld, MD Practice EssentialsDocument128 pagesDepression Medication Author: Jerry L Halverson, MD Chief Editor: David Bienenfeld, MD Practice EssentialsLauria Cindika SariNo ratings yet
- Mindfulness Therapy For Somatization Disorder and Functional Somatic Syndromes - Randomized Trial With One-Year Follow-UpDocument10 pagesMindfulness Therapy For Somatization Disorder and Functional Somatic Syndromes - Randomized Trial With One-Year Follow-UpHelena AlessiNo ratings yet
- The Stiff Elbow: Review Articles of TopicsDocument12 pagesThe Stiff Elbow: Review Articles of TopicsArif Kurniawan ListiantoNo ratings yet
- Jurnal JkmsDocument8 pagesJurnal JkmsArif Kurniawan ListiantoNo ratings yet
- Jurnal4Body Mass Index and Depressive Symptoms in Older AdultsDocument14 pagesJurnal4Body Mass Index and Depressive Symptoms in Older AdultsArif Kurniawan ListiantoNo ratings yet
- CognitipDocument2 pagesCognitipArif Kurniawan ListiantoNo ratings yet
- 1689920643.neko-Eclipse17 Freedom RoadDocument8 pages1689920643.neko-Eclipse17 Freedom RoadAdam NelonNo ratings yet
- Madam Butterfly (Okusama Chou) - Erotic PoetryDocument22 pagesMadam Butterfly (Okusama Chou) - Erotic PoetrygamahucherNo ratings yet
- 2 Changing Our Vision From Material Outlook To Spiritual Outlook PDFDocument4 pages2 Changing Our Vision From Material Outlook To Spiritual Outlook PDFvarun7salunkheNo ratings yet
- Eti 1980 01 80Document124 pagesEti 1980 01 80Adiel RicciNo ratings yet
- Quanta G31a Dag31amb6d0 Y61x-6l Rev 1aDocument49 pagesQuanta G31a Dag31amb6d0 Y61x-6l Rev 1aKrystian PalaciosNo ratings yet
- Electrical Conductivity of Aqueous SolutionsDocument1 pageElectrical Conductivity of Aqueous SolutionsTing-Ting PanNo ratings yet
- AC 43.13-1B Section 5 Penetrant InspectionDocument8 pagesAC 43.13-1B Section 5 Penetrant Inspection320338100% (1)
- DMSCO Log Book Vol.8 6/1930-5/1931Document49 pagesDMSCO Log Book Vol.8 6/1930-5/1931Des Moines University Archives and Rare Book RoomNo ratings yet
- Техническая документация B2412S-1WR2 PDFDocument6 pagesТехническая документация B2412S-1WR2 PDFИльнур ТагировNo ratings yet
- Anti-Inflammatory and Analgesic Activities of Flavonoid and Saponin Fractions From Zizyphus Lotus (L.) LamDocument5 pagesAnti-Inflammatory and Analgesic Activities of Flavonoid and Saponin Fractions From Zizyphus Lotus (L.) LamDaris UntoroNo ratings yet
- Sohbi Kohgei - Solar Power System Proposal (Toshiba325W)Document4 pagesSohbi Kohgei - Solar Power System Proposal (Toshiba325W)Jeffcaster ComelNo ratings yet
- Fess 102Document13 pagesFess 102Shivani YadavNo ratings yet
- Han Longyu 200322255 MASC PSE Fall2015 PDFDocument139 pagesHan Longyu 200322255 MASC PSE Fall2015 PDFnajib amienNo ratings yet
- Brochure Compressor Series MX 600Document2 pagesBrochure Compressor Series MX 600Samir ShahNo ratings yet
- CG-Full-Note For PU PDFDocument77 pagesCG-Full-Note For PU PDFirusha0% (1)
- TB Chapter1Document3 pagesTB Chapter1fayeNo ratings yet
- PowerSuite 03 Dec 2018 Recommended Generator Report (EGY 057VET 0238)Document1 pagePowerSuite 03 Dec 2018 Recommended Generator Report (EGY 057VET 0238)Andres BetancourtNo ratings yet
- Q-PCF-12-30-PN 6Document1 pageQ-PCF-12-30-PN 6Camilo Maya PodestaNo ratings yet
- Product News: Cat C12 ACERT™ Marine Propulsion EngineDocument6 pagesProduct News: Cat C12 ACERT™ Marine Propulsion EnginericardoNo ratings yet
- Lecture 11 Energy Transport With Energy DissipationDocument16 pagesLecture 11 Energy Transport With Energy DissipationFarahin Burhan100% (1)
- Published Article 2Document17 pagesPublished Article 2Bharathi RajaNo ratings yet
- Types of PelvisDocument23 pagesTypes of PelvisChinju Jose SajithNo ratings yet
- Systems of Alternate Current Motors and Transformers / TeslaDocument20 pagesSystems of Alternate Current Motors and Transformers / Teslaalexis.testrfNo ratings yet
- Automotive Rubber Spare Parts and Rubber-to-Metal Bonded PartsDocument14 pagesAutomotive Rubber Spare Parts and Rubber-to-Metal Bonded PartsПавел СкорецNo ratings yet
- T.E. (2019 Pattern) Insem Exam. Timetable For March-April-2024Document13 pagesT.E. (2019 Pattern) Insem Exam. Timetable For March-April-2024rauthrishikesh009No ratings yet
- LX - Advance Diploma in Medical Laboratory TechnologyDocument62 pagesLX - Advance Diploma in Medical Laboratory TechnologyGopal Ghuge RawsahebNo ratings yet
- Modeling and Simulation of A Distillation Column Using MatlabDocument15 pagesModeling and Simulation of A Distillation Column Using Matlabrajtharun48No ratings yet
- Package FaultsDocument6 pagesPackage FaultsArunraj Arumugam100% (1)
- 2022 Damat (Co Author) Kajian Aktivitas Antioksidan Mi BasahDocument15 pages2022 Damat (Co Author) Kajian Aktivitas Antioksidan Mi BasahDamatNo ratings yet