Download as pdf or txt
You might also like
- ProActive Training Case Study 1Document8 pagesProActive Training Case Study 1danthemanyvrNo ratings yet
- Clinic History and Physical MedicalTemplateDocument3 pagesClinic History and Physical MedicalTemplatee-MedTools95% (44)
- Estoya, Gen Paulo C. - Deep Vein Thrombosis NCP - NCM 112 LecDocument2 pagesEstoya, Gen Paulo C. - Deep Vein Thrombosis NCP - NCM 112 LecGen Paulo EstoyaNo ratings yet
- AIMTED 2017 Practice Exam Questions and Answers: © AIMTED 2017. All Rights Reserved. See Website For Disclaimer. 1Document25 pagesAIMTED 2017 Practice Exam Questions and Answers: © AIMTED 2017. All Rights Reserved. See Website For Disclaimer. 1evatangNo ratings yet
- Pre Op Questionnaire PDFDocument3 pagesPre Op Questionnaire PDFjgilforNo ratings yet
- Ra Case StudyDocument52 pagesRa Case StudyMiracle Guillermo100% (4)
- Waiters Rheumatoid Arthritis PDFDocument1 pageWaiters Rheumatoid Arthritis PDFmp1757100% (1)
- Juvenile Rheumatoid ArthritisDocument30 pagesJuvenile Rheumatoid Arthritispragna VanapalaNo ratings yet
- Rheumatology & Rehabilitation 2018-2019Document57 pagesRheumatology & Rehabilitation 2018-2019Selim TarekNo ratings yet
- Clinical Case 1Document10 pagesClinical Case 1aveekumbharNo ratings yet
- Juvenile Idiopathic Arthritis For The Pediatric Orthopedic SurgeonDocument18 pagesJuvenile Idiopathic Arthritis For The Pediatric Orthopedic SurgeonMayra Alejandra RamírezNo ratings yet
- Childhood ArthritisDocument73 pagesChildhood ArthritisJica GulaNo ratings yet
- Ra SlideshowDocument16 pagesRa Slideshowapi-582804360No ratings yet
- Jurnal Rheumatoid Arthritis - 6 PDFDocument4 pagesJurnal Rheumatoid Arthritis - 6 PDFJeanstepanisaragihNo ratings yet
- Pedia Case 3Document10 pagesPedia Case 3Jona Joyce JunsayNo ratings yet
- Drug StudyDocument9 pagesDrug Studytalia hamedNo ratings yet
- Pain in and Around JointsDocument11 pagesPain in and Around JointsitstwelveNo ratings yet
- Clinico Pathological Correlation: Sarathchandran KDocument26 pagesClinico Pathological Correlation: Sarathchandran Ksarath chandranNo ratings yet
- Childhood Arthritis: RCSI Students 2013Document41 pagesChildhood Arthritis: RCSI Students 2013Mohamed KhatibNo ratings yet
- Case Presentation CardiomyopathyDocument30 pagesCase Presentation CardiomyopathyKshayna 1234No ratings yet
- The Vaccine Adverse Event Reporting SystDocument184 pagesThe Vaccine Adverse Event Reporting SystAlcides Riera MoraNo ratings yet
- Prctmol OkDocument1 pagePrctmol OkSethlyn_Gomez_5337No ratings yet
- Approach To A Patient With PolyarthritisDocument29 pagesApproach To A Patient With PolyarthritisMd ImamuddinNo ratings yet
- RenalDocument11 pagesRenalayunisallehNo ratings yet
- Lupus SeverDocument3 pagesLupus SeverdeliaNo ratings yet
- Arthritis: By: Charmaine BaniquedDocument106 pagesArthritis: By: Charmaine BaniquedGemgem Acosta100% (1)
- Approach To Polyarthritis For The Primary Care Physician: Arielle Freilich, DO, PGY2 & Helaine Larsen, DODocument8 pagesApproach To Polyarthritis For The Primary Care Physician: Arielle Freilich, DO, PGY2 & Helaine Larsen, DOLydia IsaacNo ratings yet
- Pembahasan To Online 3Document201 pagesPembahasan To Online 3Fate DreamworkNo ratings yet
- Mari Zita Spa OnDocument57 pagesMari Zita Spa OnMarty BrownNo ratings yet
- Medicine Seminar: Sakshi Malik 379 Shalini Singh 384 Sunanda Verma 394Document53 pagesMedicine Seminar: Sakshi Malik 379 Shalini Singh 384 Sunanda Verma 394966342No ratings yet
- DD ArthritisDocument6 pagesDD ArthritiskabhusNo ratings yet
- PulmonaryDocument12 pagesPulmonaryayunisallehNo ratings yet
- Dengue FeverDocument5 pagesDengue FeverRayana UbasNo ratings yet
- Case StudypcolDocument5 pagesCase StudypcolJoshua AysonNo ratings yet
- Case Presentation - GBSDocument28 pagesCase Presentation - GBSJan Marvin Lichauco MendozaNo ratings yet
- Joint Pain Case StudiesDocument51 pagesJoint Pain Case StudiesNaziBrola TsivadzeNo ratings yet
- Hari-3 - 02 - Dr. Alindina - Demam TifoidDocument33 pagesHari-3 - 02 - Dr. Alindina - Demam TifoidmodrsbmNo ratings yet
- ORAL KetamineDocument5 pagesORAL Ketaminerobo100% (1)
- Approach To Joint Pain (October 2022)Document56 pagesApproach To Joint Pain (October 2022)imranmohammad968No ratings yet
- OsteoarthritisDocument29 pagesOsteoarthritisfizhazhiNo ratings yet
- Ra Concept Map CompletionDocument18 pagesRa Concept Map Completionapi-308471999No ratings yet
- Spond Ylo ArthritisDocument58 pagesSpond Ylo ArthritisirsyadilfikriNo ratings yet
- Final PBLDocument11 pagesFinal PBLjanhvichougule3006No ratings yet
- Approach To Case of ArthritisDocument53 pagesApproach To Case of ArthritisdrsarathmenonNo ratings yet
- Introduction To Clinical Medicine (ICM) Diseases of The Musculoskeletal System and JointsDocument144 pagesIntroduction To Clinical Medicine (ICM) Diseases of The Musculoskeletal System and JointsomarNo ratings yet
- 103-Article Text-477-2-10-20201107Document14 pages103-Article Text-477-2-10-20201107Belinda SuhuyanlyNo ratings yet
- The Steroid Withdrawal Syndrome: A Review of The Implications, Etiology, and TreatmentsDocument5 pagesThe Steroid Withdrawal Syndrome: A Review of The Implications, Etiology, and TreatmentsChristopher Surya SuwitaNo ratings yet
- Case Presentation On Chronic Osteomyelitis: Prepared By: Sital Gautam MN1 Year, 2012Document55 pagesCase Presentation On Chronic Osteomyelitis: Prepared By: Sital Gautam MN1 Year, 2012Rabina RajbanshiNo ratings yet
- Drug Name Drug Class Mechanism of Action Indications Contraindications Side Effects/ Adverse Effects Nursing ConsiderationDocument3 pagesDrug Name Drug Class Mechanism of Action Indications Contraindications Side Effects/ Adverse Effects Nursing ConsiderationKim SunooNo ratings yet
- Primary Care 6531Document28 pagesPrimary Care 6531Zaha CalatravaNo ratings yet
- Case Report Rheumatoid ArthritisDocument29 pagesCase Report Rheumatoid ArthritisEmmy Safitri Abbas0% (1)
- SIGNS AND SYMPTOMS, SKIN LESIONS, EtcDocument7 pagesSIGNS AND SYMPTOMS, SKIN LESIONS, EtcMukesh KhatiNo ratings yet
- Ankylosing Spondylitis: An Update: RheumatologyDocument5 pagesAnkylosing Spondylitis: An Update: RheumatologyNazmul IslamNo ratings yet
- Herpes Z Oster Clinical PresentationDocument50 pagesHerpes Z Oster Clinical PresentationS KkNo ratings yet
- MY-MIM-048 2017 Emergency Med Sulivan Gastroentritis CMDocument5 pagesMY-MIM-048 2017 Emergency Med Sulivan Gastroentritis CMwazerbeqNo ratings yet
- A Patient With Joint PainDocument18 pagesA Patient With Joint PainAnuradha NanayakkaraNo ratings yet
- Par Diagnostic Si TratamentDocument8 pagesPar Diagnostic Si TratamentValeria BostanNo ratings yet
- Approach To The Patient With ArthritisDocument10 pagesApproach To The Patient With ArthritisshosmedNo ratings yet
- Arthritis and Related Disorders Types and TreatmentDocument8 pagesArthritis and Related Disorders Types and Treatmentmf6pjpswswNo ratings yet
- FUO-6th Year MedicineDocument25 pagesFUO-6th Year MedicineananNo ratings yet
- ParacetamolDocument1 pageParacetamoljennelyn losantaNo ratings yet
- Nursing Care Plan LeptospirosisDocument2 pagesNursing Care Plan Leptospirosisderic86% (21)
- Chronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicFrom EverandChronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicRating: 5 out of 5 stars5/5 (1)
- Profile of Waling On Reconstruction and RetrofittingDocument2 pagesProfile of Waling On Reconstruction and RetrofittingDIMariaAUnitedNo ratings yet
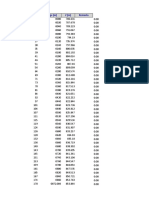
- S.N. Chainage (M) Z (M) RemarksDocument169 pagesS.N. Chainage (M) Z (M) RemarksDIMariaAUnitedNo ratings yet
- Dismantling HillyDocument26 pagesDismantling HillyDIMariaAUnitedNo ratings yet
- Chainage (M) Length (M) Diameter (M) Pipe Count Clear Cover Depth (M) Slope (1V:mH)Document4 pagesChainage (M) Length (M) Diameter (M) Pipe Count Clear Cover Depth (M) Slope (1V:mH)DIMariaAUnitedNo ratings yet
- Soil Classification - Hill SideDocument30 pagesSoil Classification - Hill SideDIMariaAUnitedNo ratings yet
- EW Data-Terai SectionDocument354 pagesEW Data-Terai SectionDIMariaAUnitedNo ratings yet
- Subject: Subject: Draft Report Submission: Regd. No.: 48396-063/64 PAN: 302707869Document3 pagesSubject: Subject: Draft Report Submission: Regd. No.: 48396-063/64 PAN: 302707869DIMariaAUnitedNo ratings yet
- Terms of Reference: 1.1 Location of Proposed Tropical HouseDocument5 pagesTerms of Reference: 1.1 Location of Proposed Tropical HouseDIMariaAUnitedNo ratings yet
- Ladhari L-Profile and X-SecDocument2 pagesLadhari L-Profile and X-SecDIMariaAUnitedNo ratings yet
- Chainage (M) Span (M) Thickness (M) Depth (M) Remarks Work CodeDocument2 pagesChainage (M) Span (M) Thickness (M) Depth (M) Remarks Work CodeDIMariaAUnitedNo ratings yet
- DESIGN PROFILE - 30kmhrDocument14 pagesDESIGN PROFILE - 30kmhrDIMariaAUnitedNo ratings yet
- Test Report: Dynamic Cone Penetration Test (DCPT)Document4 pagesTest Report: Dynamic Cone Penetration Test (DCPT)DIMariaAUnitedNo ratings yet
- 022 Iee 27Document105 pages022 Iee 27DIMariaAUnitedNo ratings yet
- Pedestrian and Bicycle Planning: A Guide To Best PracticesDocument89 pagesPedestrian and Bicycle Planning: A Guide To Best PracticesDIMariaAUnitedNo ratings yet
- PDF Created With Pdffactory Pro Trial VersionDocument21 pagesPDF Created With Pdffactory Pro Trial VersionDIMariaAUnitedNo ratings yet
- 4.d Manning Schedule-1Document1 page4.d Manning Schedule-1DIMariaAUnitedNo ratings yet
- Client Ministry of Federal Affairs and Local Development Gipayal Silgadi Municipality DotiDocument2 pagesClient Ministry of Federal Affairs and Local Development Gipayal Silgadi Municipality DotiDIMariaAUnitedNo ratings yet
- DVC AuditRepirt 2020Document9 pagesDVC AuditRepirt 2020DIMariaAUnitedNo ratings yet
- Test Report: Project: Date: Location: Weather: Tested By: Chainage: 0+000Document45 pagesTest Report: Project: Date: Location: Weather: Tested By: Chainage: 0+000DIMariaAUnitedNo ratings yet
- E2 Out Going LattersDocument3 pagesE2 Out Going LattersDIMariaAUnitedNo ratings yet
- Road EstimateDocument244 pagesRoad EstimateDIMariaAUnitedNo ratings yet
- Probablity and Random VariablesDocument113 pagesProbablity and Random VariablesDIMariaAUnitedNo ratings yet
- 4.c Work SCH KathmanduDocument2 pages4.c Work SCH KathmanduDIMariaAUnitedNo ratings yet
- Epicor Prevents and Reduces Inflammation in Two Separate Experimental Immune Animal ModelsDocument8 pagesEpicor Prevents and Reduces Inflammation in Two Separate Experimental Immune Animal ModelssteeljackNo ratings yet
- STUDY GUIDE 2 (Operaña, Ellayza)Document4 pagesSTUDY GUIDE 2 (Operaña, Ellayza)OPERAñA ELLAYZA RB DECANONo ratings yet
- RemoveWatermark Module+2+Adaptive+Easy 240121 103210Document10 pagesRemoveWatermark Module+2+Adaptive+Easy 240121 103210Ahmed tahaNo ratings yet
- BursitisDocument23 pagesBursitisAngie Paola RodriguezNo ratings yet
- Rain Soul Testimonials 2 7 17Document17 pagesRain Soul Testimonials 2 7 17api-244808410No ratings yet
- Rheumatoid Arthritis Thesis StatementDocument5 pagesRheumatoid Arthritis Thesis Statementafjryccau100% (1)
- Thomas McPherson Brown MD Treatment of Rheumatoid DiseaseDocument29 pagesThomas McPherson Brown MD Treatment of Rheumatoid DiseaseLidia Lidia100% (1)
- DVDGGDocument10 pagesDVDGGSilviNo ratings yet
- Functional and Work Outcomes Improve in Patients With Rheumatoid Arthritis Who Receive Targeted, Comprehensive Occupational TherapyDocument9 pagesFunctional and Work Outcomes Improve in Patients With Rheumatoid Arthritis Who Receive Targeted, Comprehensive Occupational TherapyispasNo ratings yet
- Pedro 1Document34 pagesPedro 1Samantha Agustin100% (1)
- COP Module 3 Endterm Health Problems 1Document110 pagesCOP Module 3 Endterm Health Problems 1Leonifel BersaminaNo ratings yet
- Locomotor - Hand Clinical Mark SheetDocument7 pagesLocomotor - Hand Clinical Mark SheetDrShamshad KhanNo ratings yet
- 5 Bullets MS 3Document21 pages5 Bullets MS 3rihamNo ratings yet
- BFO-Review of Pathology AFODocument32 pagesBFO-Review of Pathology AFOnovitaNo ratings yet
- Autacoids For Med.Document140 pagesAutacoids For Med.Feysal AhmedNo ratings yet
- 5.children With Physical ImpairmentDocument8 pages5.children With Physical ImpairmentJunadrian GenitoNo ratings yet
- Reiter S SyndromeDocument4 pagesReiter S SyndromeInternational Medical PublisherNo ratings yet
- General Principles of Management of Rheumatoid Arthritis in Adults - UpToDateDocument26 pagesGeneral Principles of Management of Rheumatoid Arthritis in Adults - UpToDateSalo MarianoNo ratings yet
- Transmarine Carriers V BernardoDocument2 pagesTransmarine Carriers V BernardoDerick TorresNo ratings yet
- PnleDocument118 pagesPnleZanie CruzNo ratings yet
- 6 NDJ - Limfadenopati LimfadenitisDocument45 pages6 NDJ - Limfadenopati LimfadenitisYUFFANo ratings yet
- Task 1. Active Learning Template: Assessment Teamwork and CollaborationDocument2 pagesTask 1. Active Learning Template: Assessment Teamwork and CollaborationAce FabrigasNo ratings yet
- BFKT Test 1Document1 pageBFKT Test 1Laurus AdiaNo ratings yet
- Moving Away From Knee Osteoarthritis - Harvard HealthDocument1 pageMoving Away From Knee Osteoarthritis - Harvard HealthOctavio LópezNo ratings yet
- Ra and Osteoarthritis R IfDocument43 pagesRa and Osteoarthritis R IfsnfhanNo ratings yet