Download as pdf or txt
You might also like
- Full Download Ebook PDF Netters Atlas of Human Embryology Updated Edition PDFDocument41 pagesFull Download Ebook PDF Netters Atlas of Human Embryology Updated Edition PDFkenneth.edwards64498% (41)
- Clinical Epidemiology and Biostatistics A Primer For Clinical Investigators and Decision MakersDocument289 pagesClinical Epidemiology and Biostatistics A Primer For Clinical Investigators and Decision Makerszucca100% (2)
- Extended Heredity: A New Understanding of Inheritance and EvolutionFrom EverandExtended Heredity: A New Understanding of Inheritance and EvolutionNo ratings yet
- Kenneth W. Goodman - Ethics and Evidence-Based Medicine - Fallibility and Responsibility in Clinical Science (2002) PDFDocument181 pagesKenneth W. Goodman - Ethics and Evidence-Based Medicine - Fallibility and Responsibility in Clinical Science (2002) PDFhgfelipe87No ratings yet
- Practical Flow Cytometry, 4th Edition.17Document2 pagesPractical Flow Cytometry, 4th Edition.17Catalina BanuNo ratings yet
- Bui Van Minh - CVDocument2 pagesBui Van Minh - CVVan MinhNo ratings yet
- Social Studies Lesson PlanDocument7 pagesSocial Studies Lesson Planapi-404999113No ratings yet
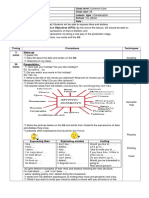
- Unit 4 Expres Likes & Dislikes Conversation C.CDocument2 pagesUnit 4 Expres Likes & Dislikes Conversation C.Chbat said100% (2)
- Textbook On Pediatric Clinical PharmacologyDocument4 pagesTextbook On Pediatric Clinical PharmacologyAhsan KabirNo ratings yet
- 14 FaDocument2 pages14 FaMADHU GIRI 2170094No ratings yet
- Nonsexist Research Methods A Practical GDocument2 pagesNonsexist Research Methods A Practical GCamila SánchezNo ratings yet
- Book Review: American Journal of Medical Genetics 72:250 (1997)Document1 pageBook Review: American Journal of Medical Genetics 72:250 (1997)José Abraham Amaya DuarteNo ratings yet
- Norman2007 PDFDocument3 pagesNorman2007 PDFEMILIANO CAMACHO RAMOSNo ratings yet
- Postmedj00208 0062cDocument2 pagesPostmedj00208 0062cابراهيم العسيريNo ratings yet
- Practical Head and Neck Pathology: Frequently Asked QuestionsFrom EverandPractical Head and Neck Pathology: Frequently Asked QuestionsDanielle Elliott RangeNo ratings yet
- Biochimia CreieruluiDocument2 pagesBiochimia CreieruluiRadu BadoiuNo ratings yet
- 4125 Pediatrics Product SamplerDocument23 pages4125 Pediatrics Product SamplercapttheosNo ratings yet
- 1988 Book ClinicalEpidemiologyAndBiostatDocument290 pages1988 Book ClinicalEpidemiologyAndBiostatJéssica BittencourtNo ratings yet
- Psychopathic and Antisocial Personality Disorders: Treatment and Research IssuesDocument3 pagesPsychopathic and Antisocial Personality Disorders: Treatment and Research IssuesIrisha AnandNo ratings yet
- Fundamentals of Nursing Concepts ProcessDocument1 pageFundamentals of Nursing Concepts Processagathamboe4No ratings yet
- Neuropsychological Evaluation of The ChildDocument51 pagesNeuropsychological Evaluation of The ChildrushnaNo ratings yet
- Essential Endocrinology - A Primer For Nonspecialists (1986, Springer US)Document514 pagesEssential Endocrinology - A Primer For Nonspecialists (1986, Springer US)trần quốc vĩ0% (1)
- Ethical Issues in Death and DyingDocument2 pagesEthical Issues in Death and Dying2022-200395No ratings yet
- Junqueiras Basic Histology 14e 14th Edition Ebook PDFDocument61 pagesJunqueiras Basic Histology 14e 14th Edition Ebook PDFhenrietta.hallquist413100% (44)
- Robbins Review of PathologyDocument2 pagesRobbins Review of PathologyTofik MohammedNo ratings yet
- Introduction To Toxicology: ReviewsDocument2 pagesIntroduction To Toxicology: ReviewsMárcio RodriguesNo ratings yet
- Difference Between Literature Review and EssayDocument5 pagesDifference Between Literature Review and Essayqtbghsbnd100% (1)
- Chinese Medicine Research PaperDocument8 pagesChinese Medicine Research Papermoykicvnd100% (1)
- Book Reviews: Mayo Clinic Gastrointestinal Surgery Physiologic Basis of Surgery. 3rd EdDocument2 pagesBook Reviews: Mayo Clinic Gastrointestinal Surgery Physiologic Basis of Surgery. 3rd EdIhsan DisiniNo ratings yet
- Histology and Cell Biology An Introduction To Pathology 5Th Edition Abraham L Kierszenbaum Full ChapterDocument67 pagesHistology and Cell Biology An Introduction To Pathology 5Th Edition Abraham L Kierszenbaum Full Chapterdennis.roberson462100% (21)
- R D Ttrct&I: Books ReviewedDocument1 pageR D Ttrct&I: Books ReviewedPeterNo ratings yet
- The Yale Journal of Biology and Medicine June 2015Document3 pagesThe Yale Journal of Biology and Medicine June 2015Osama AtifNo ratings yet
- McCleodreview1 2011submittedDocument4 pagesMcCleodreview1 2011submittedahlem bhmNo ratings yet
- Lippincott Williams & Wilkins The American Journal of NursingDocument2 pagesLippincott Williams & Wilkins The American Journal of NursingRjsjcjNo ratings yet
- Postmedj00189 0078aDocument1 pagePostmedj00189 0078aikebuakupearlNo ratings yet
- The Biology of CancerDocument3 pagesThe Biology of CancerPianista10% (1)
- C.coek - Info Comprehensive Gynecology Review 4th EditionDocument1 pageC.coek - Info Comprehensive Gynecology Review 4th EditionCylyn Ann CabatinganNo ratings yet
- Histology and Cell Biology An Introduction To Pathology 5Th Edition Abraham L Kierszenbaum M D PH D Full ChapterDocument67 pagesHistology and Cell Biology An Introduction To Pathology 5Th Edition Abraham L Kierszenbaum M D PH D Full Chapterdennis.roberson462100% (17)
- FULL Download Ebook PDF Junqueiras Basic Histology Text and Atlas 15th Edition PDF EbookDocument41 pagesFULL Download Ebook PDF Junqueiras Basic Histology Text and Atlas 15th Edition PDF Ebookcandace.binegar878100% (38)
- Frameworks For Practice in The Systemic Field: Part 1Document16 pagesFrameworks For Practice in The Systemic Field: Part 1JujuNo ratings yet
- First Principles of Gastroenterology and HepatologyDocument826 pagesFirst Principles of Gastroenterology and HepatologyDiana Iordache100% (1)
- Schwartz & Dell, 2010Document19 pagesSchwartz & Dell, 2010FanyestNo ratings yet
- Sociology of Health and Illness: Fergusos@grinnell - EduDocument18 pagesSociology of Health and Illness: Fergusos@grinnell - EduRanchuJoseNo ratings yet
- Medical NeurobiologyDocument682 pagesMedical NeurobiologyMaría CristinaNo ratings yet
- The Vulva & Vagina Manual YmjdDocument2 pagesThe Vulva & Vagina Manual Ymjd5jnpzgz4cqNo ratings yet
- Principles of Medical GeneticsDocument3 pagesPrinciples of Medical GeneticsJORGE ALEJANDRO MOLINA PARRANo ratings yet
- Cecil - Pediatric PsychopharmacologyDocument837 pagesCecil - Pediatric Psychopharmacologypinkykuku12No ratings yet
- Antisocial Personality Disorder An EpidemiologicalDocument2 pagesAntisocial Personality Disorder An EpidemiologicalFarina FatimaNo ratings yet
- What Is A Case Study in The ScienceDocument39 pagesWhat Is A Case Study in The ScienceJA GANo ratings yet
- Effective Speech Language PathologyDocument173 pagesEffective Speech Language PathologyLucas Gandy100% (1)
- ROZUL, Patricia Dianne MDocument27 pagesROZUL, Patricia Dianne MDianne RozulNo ratings yet
- Term Paper On Stem Cell ResearchDocument5 pagesTerm Paper On Stem Cell Researchafdtorpqk100% (1)
- Nejmx 080030Document1 pageNejmx 080030fahad alkatheryNo ratings yet
- Practical Statistics For Medical ResearchDocument2 pagesPractical Statistics For Medical ResearchShanmuga Sundaram0% (1)
- Book Review: American Journal of Medical Genetics 77:338-339 (1998)Document2 pagesBook Review: American Journal of Medical Genetics 77:338-339 (1998)pajtgocjNo ratings yet
- Why Did I Choose Pathology As A Career?: The ExperienceDocument2 pagesWhy Did I Choose Pathology As A Career?: The ExperienceGupita WidyadhariNo ratings yet
- Science and Morality in Medicine: A Survey of Medical EducatorsFrom EverandScience and Morality in Medicine: A Survey of Medical EducatorsNo ratings yet
- Skull Base Surgery: Facial SurgeryDocument2 pagesSkull Base Surgery: Facial SurgeryVerica JankelićNo ratings yet
- Ten Common Questions (And Their Answers) On Medical FutilityDocument17 pagesTen Common Questions (And Their Answers) On Medical FutilitycindyNo ratings yet
- Vestibular DisorderDocument417 pagesVestibular DisorderDEEKSHA ABROLNo ratings yet
- Book Review: American Journal of Medical Genetics 73:236 (1997)Document1 pageBook Review: American Journal of Medical Genetics 73:236 (1997)Maxime PorcoNo ratings yet
- Course Outline TEP 072015Document7 pagesCourse Outline TEP 072015dautaychua2008No ratings yet
- Worksheet On SnapshotDocument7 pagesWorksheet On SnapshotaNo ratings yet
- Banasthali Request LetterDocument7 pagesBanasthali Request LetterShreya DeyNo ratings yet
- The Marginal Man Hans Morgenthau PDFDocument286 pagesThe Marginal Man Hans Morgenthau PDFlilianaNo ratings yet
- Book Lovers ClubDocument3 pagesBook Lovers ClubMN FerueloNo ratings yet
- Internship Log Book CopierDocument20 pagesInternship Log Book CopierCollenNo ratings yet
- Soal Sinonim Dan AntonimDocument14 pagesSoal Sinonim Dan Antonimilham sukriNo ratings yet
- Zannemily - Resume2021Document1 pageZannemily - Resume2021api-546387929No ratings yet
- Practical Research 1 Kenneth G. Bacala 11 1: Himamaylan National High School Senior High School (SHS)Document5 pagesPractical Research 1 Kenneth G. Bacala 11 1: Himamaylan National High School Senior High School (SHS)Rodito Jr VillanuevaNo ratings yet
- Musical Knowledge For Drum Kit PDFDocument1 pageMusical Knowledge For Drum Kit PDFLeny Almario RonquilloNo ratings yet
- Individual Reading StatusDocument5 pagesIndividual Reading StatusAleli LandoyNo ratings yet
- 02 WholeDocument308 pages02 WholeEdu CordonNo ratings yet
- Collegeboard-Approved Ap Calculus BC Syllabus-2Document6 pagesCollegeboard-Approved Ap Calculus BC Syllabus-2api-292365857No ratings yet
- Syllabus HRM, Jan-May 2012Document12 pagesSyllabus HRM, Jan-May 2012alejandro_garcia_240No ratings yet
- Annnual SpeechDocument8 pagesAnnnual SpeechVaishali ShuklaNo ratings yet
- Educational Philosophies and Their ProponentsDocument2 pagesEducational Philosophies and Their ProponentsEvaNo ratings yet
- Cambridge O Level: Second Language Urdu 3248/01Document8 pagesCambridge O Level: Second Language Urdu 3248/01Muhammad HarisNo ratings yet
- Fame Master CV TemplateDocument2 pagesFame Master CV TemplateRaviRoshanKeshariNo ratings yet
- 10th Maths FinalDocument344 pages10th Maths FinalRahul NarasimmanNo ratings yet
- Reach and ICAS Comparison TableDocument1 pageReach and ICAS Comparison Tablekltch2No ratings yet
- Recipe For TPRDocument13 pagesRecipe For TPRestefania hernandezNo ratings yet
- Metzger y Otros A Comparative PerspectiveDocument9 pagesMetzger y Otros A Comparative PerspectiveEl CuervoNo ratings yet
- Introduction Broken HomesDocument2 pagesIntroduction Broken HomesNslaimoa Ajh100% (6)
- Ode To A Grecian Urn - Discussion - Questions - ECDocument2 pagesOde To A Grecian Urn - Discussion - Questions - ECSudeshna bharNo ratings yet
- Human Population and EnvironmentDocument5 pagesHuman Population and EnvironmentRahul0% (1)
- How Does Society Influence Our Development As PersonsDocument22 pagesHow Does Society Influence Our Development As PersonsKirl GilNo ratings yet
- Abebaw BelachewDocument129 pagesAbebaw BelachewMohamed BioNo ratings yet