Download as pdf or txt
You might also like
- Biocidal Activity Report NadccDocument32 pagesBiocidal Activity Report NadccFabiola OlivaresNo ratings yet
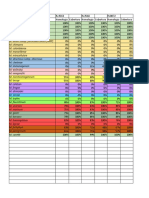
- Organism Indcidence in Blood 2022Document2 pagesOrganism Indcidence in Blood 2022anisNo ratings yet
- Enter Antimicrobial Agent NameDocument17 pagesEnter Antimicrobial Agent NameUlin Nuha JazminNo ratings yet
- Pemeriksaan JamurDocument10 pagesPemeriksaan JamurkiflyNo ratings yet
- 216 2011 4877 Moesm1 EsmDocument4 pages216 2011 4877 Moesm1 EsmEllaNo ratings yet
- Amkamxamcampsamazmatmbpc Cfzfep CFM: Sensitivitas Antibiotik Di Rsud Dr. Harjono S PonorogoDocument3 pagesAmkamxamcampsamazmatmbpc Cfzfep CFM: Sensitivitas Antibiotik Di Rsud Dr. Harjono S Ponorogotresna anggaNo ratings yet
- Type Strain Genome ServerDocument37 pagesType Strain Genome ServerTeresita CamachoNo ratings yet
- Foodborne Illnesses in Developing CountriesDocument18 pagesFoodborne Illnesses in Developing CountriesKhalifa Sifaw GhengheshNo ratings yet
- Conservação Micobactérias FinalDocument4 pagesConservação Micobactérias FinalAhlex Van der AllNo ratings yet
- Peta Kuman 2022Document3 pagesPeta Kuman 2022Musyafa'atun AnitaNo ratings yet
- Sensitivitas KumanDocument16 pagesSensitivitas KumanduckshaNo ratings yet
- Kepekaan Antibiotik Pada Darah 2022Document20 pagesKepekaan Antibiotik Pada Darah 2022anisNo ratings yet
- Amina Bukar Grema Slid UpdatedDocument14 pagesAmina Bukar Grema Slid UpdatedMusa AbubakarNo ratings yet
- IndentifikasiDocument10 pagesIndentifikasiNur AeniNo ratings yet
- M031 PDFDocument3 pagesM031 PDFandualemNo ratings yet
- The Evaluation of The in Vitro AntiDocument6 pagesThe Evaluation of The in Vitro Antiscolasticakunambi18No ratings yet
- Investigation On Streptomycin Inhibitors With The Aid of A Streptomycin-Dependent Vibrio CommuDocument8 pagesInvestigation On Streptomycin Inhibitors With The Aid of A Streptomycin-Dependent Vibrio CommuSwati HegdeNo ratings yet
- SMH118CDocument4 pagesSMH118CNanthicha KrajangpawNo ratings yet
- Principles in Antimicrobial Therapy: The Abcs: Benjamin G. Co, MD, FPPS, FpsecpDocument46 pagesPrinciples in Antimicrobial Therapy: The Abcs: Benjamin G. Co, MD, FPPS, FpsecpAayushi AggarwalNo ratings yet
- Xylose-Lysine Deoxycholate Agar (XLD Agar) : Intended UseDocument5 pagesXylose-Lysine Deoxycholate Agar (XLD Agar) : Intended UseAmbika ShindeNo ratings yet
- Bioteknologi Mikroorganisme LautDocument10 pagesBioteknologi Mikroorganisme LautEM Read-One LessyNo ratings yet
- Uji Spss Bawang Dayak BuliaDocument5 pagesUji Spss Bawang Dayak BuliahairunnisaaaNo ratings yet
- Readycult Coliforms 100: Ordering Number: 1.01298.0001Document4 pagesReadycult Coliforms 100: Ordering Number: 1.01298.0001Maria Alejandra VillalbaNo ratings yet
- POLA KUMAN OKTOBER 2023 11 OkDocument100 pagesPOLA KUMAN OKTOBER 2023 11 Okmaspul lamuruprintNo ratings yet
- Streptococcus Thermophilus: Revival of The Species Oria-Jensen, 1919) Nom. RevDocument3 pagesStreptococcus Thermophilus: Revival of The Species Oria-Jensen, 1919) Nom. RevТаро и Астрология с Anatoly KartNo ratings yet
- UVC Dose Table For Viruses Bacteria Moulds EtcDocument7 pagesUVC Dose Table For Viruses Bacteria Moulds EtcBosco WoodsNo ratings yet
- Working For A Healthier World: Dr. Nang Ying Nom Kham PSR IiDocument33 pagesWorking For A Healthier World: Dr. Nang Ying Nom Kham PSR IiMyoNo ratings yet
- Bioactivities of Sesbania Sesban ExtractivesDocument3 pagesBioactivities of Sesbania Sesban Extractiveshilma adilaNo ratings yet
- Epo No5 Oct2010Document4 pagesEpo No5 Oct2010Markus Deni KuncoroNo ratings yet
- FluomizinDocument4 pagesFluomizinAyu Rahmawati HidayatNo ratings yet
- Tabla Enterobacteriaceae PDFDocument3 pagesTabla Enterobacteriaceae PDFRené LoZanoNo ratings yet
- Daily Plankton Agrabinta CianjurDocument141 pagesDaily Plankton Agrabinta CianjurPutra Cahya GemilangNo ratings yet
- Page 005Document1 pagePage 005Alejandra LópezNo ratings yet
- CMB Lab Written Report Ex 4Document5 pagesCMB Lab Written Report Ex 4Fiona SimeonNo ratings yet
- Ba0001 TM1 PDFDocument4 pagesBa0001 TM1 PDFLiz W. Villarreal WaiwaNo ratings yet
- Observations & ResultsDocument6 pagesObservations & ResultsavnishNo ratings yet
- Rappaport Vassiliadis Medium: Ordering Number: 1.46181.0020 / 1.46181.0100Document3 pagesRappaport Vassiliadis Medium: Ordering Number: 1.46181.0020 / 1.46181.0100Dice TwelveNo ratings yet
- Technical Data Sheet: Readycult® Coliforms 100Document4 pagesTechnical Data Sheet: Readycult® Coliforms 100AnnisaNo ratings yet
- New Genus Of: Levinea, EnterobacteriaceaeDocument6 pagesNew Genus Of: Levinea, EnterobacteriaceaeJuan Carlos Colina VenegasNo ratings yet
- Amr Ppra Bethesda 2017 (DR Hari)Document29 pagesAmr Ppra Bethesda 2017 (DR Hari)Maya DamanikNo ratings yet
- Program Pengendalian Resistensi Antimikroba: (PPRA) Di Rumah SakitDocument34 pagesProgram Pengendalian Resistensi Antimikroba: (PPRA) Di Rumah Sakitevy sari sutrisnaningsih100% (1)
- SOP Aerobic Gram Negative Bacilli SalmonellaDocument8 pagesSOP Aerobic Gram Negative Bacilli SalmonellaBabelNo ratings yet
- Program Pengendalian Resistensi Antimikroba Di Rumah SakitDocument23 pagesProgram Pengendalian Resistensi Antimikroba Di Rumah SakitYulia Wati Safitri SanjayaNo ratings yet
- Atlas of Medical BacteriologyDocument103 pagesAtlas of Medical BacteriologyNilesh MaitiNo ratings yet
- Bayer 3rd Proc'99 - HARRISDocument6 pagesBayer 3rd Proc'99 - HARRISsergioNo ratings yet
- Staphylococcus Factsheet FINALDocument5 pagesStaphylococcus Factsheet FINALAhmed TharwatNo ratings yet
- Formal Lab 4 Report B00505932Document5 pagesFormal Lab 4 Report B00505932kirsti_jangaardNo ratings yet
- Curva Do Coletor - 20052024Document2 pagesCurva Do Coletor - 20052024Maria IzabelNo ratings yet
- 966.24 NMPDocument2 pages966.24 NMPAlvaro NAVARRONo ratings yet
- Principle General Information Mode of Action Experimental Procedure and EvaluationDocument2 pagesPrinciple General Information Mode of Action Experimental Procedure and EvaluationmohammedNo ratings yet
- Mikrobiologi Industri: Taksonomi MikroorganismeDocument51 pagesMikrobiologi Industri: Taksonomi MikroorganismeEunike RhizaNo ratings yet
- Taenia Solium Cysticercosis: Immunity in Pigs Induced by Primary InfectionDocument7 pagesTaenia Solium Cysticercosis: Immunity in Pigs Induced by Primary InfectionAna VargasNo ratings yet
- MLE-T Eng 20140723Document17 pagesMLE-T Eng 20140723Putri Gyar PertiwiNo ratings yet
- Determination of M.O in Herbal ProductsDocument11 pagesDetermination of M.O in Herbal Productsreda_bassuonyNo ratings yet
- Surveylans Terpadu Penyakit Berbasis Puskesmas Kasus Baru September 2019 Golongan Umur TotalDocument3 pagesSurveylans Terpadu Penyakit Berbasis Puskesmas Kasus Baru September 2019 Golongan Umur TotalPuskesmas BatusepuluhNo ratings yet
- Microbial Organisms Causing Specific Types of Urinary Tract InfectionsDocument1 pageMicrobial Organisms Causing Specific Types of Urinary Tract InfectionsVeruna AveriNo ratings yet
- Tn1363en MKDocument3 pagesTn1363en MKFlorencia PieragostiniNo ratings yet
- Abstrak Efek Inhibisi Ekstrak Etanol Batang Kayu Manis (Cinnamomum Burmanni) TERHADAP PERTUMBUHAN BAKTERIDocument6 pagesAbstrak Efek Inhibisi Ekstrak Etanol Batang Kayu Manis (Cinnamomum Burmanni) TERHADAP PERTUMBUHAN BAKTERIFrengkyNo ratings yet
- Gynae History TakingDocument23 pagesGynae History TakingAlmira PutriNo ratings yet
- Ujian Journal Reading PPT Laringofaringeal RefluxDocument25 pagesUjian Journal Reading PPT Laringofaringeal RefluxAlmira PutriNo ratings yet
- Dyspepsia - DR NataDocument23 pagesDyspepsia - DR NataAlmira PutriNo ratings yet
- Term Example Discoloration Flat,: Patch ( 1cm) Papule ( 1cm)Document4 pagesTerm Example Discoloration Flat,: Patch ( 1cm) Papule ( 1cm)Almira PutriNo ratings yet
- Journal of Sleep Disorders & Therapy Snoring: Recommended JournalsDocument4 pagesJournal of Sleep Disorders & Therapy Snoring: Recommended JournalsAlmira PutriNo ratings yet
- Dyspnea: Dr. Siddharth - Med PGDocument37 pagesDyspnea: Dr. Siddharth - Med PGAlmira PutriNo ratings yet
- Upper Airway Obstruction: Many Causes, 3 OutcomesDocument29 pagesUpper Airway Obstruction: Many Causes, 3 OutcomesAlmira PutriNo ratings yet
- Physical Exam in Kidney DiseasenDocument26 pagesPhysical Exam in Kidney DiseasenAlmira PutriNo ratings yet
- Soal HO Rev 1nnnDocument21 pagesSoal HO Rev 1nnnAlmira PutriNo ratings yet
- Soal First Aid Quiz MentorDocument9 pagesSoal First Aid Quiz MentorAlmira PutriNo ratings yet
- Osteogenesis Imperfecta: TypesDocument9 pagesOsteogenesis Imperfecta: TypesAlmira PutriNo ratings yet
- Arteries of The Upper Limb: Artery Origin Branches VaskulaisasiDocument15 pagesArteries of The Upper Limb: Artery Origin Branches VaskulaisasiAlmira PutriNo ratings yet
- Clinical SkilllllllllllllllDocument12 pagesClinical SkilllllllllllllllAlmira Putri100% (1)
- Particularities of Family Planning in Women With Mental DisordersDocument6 pagesParticularities of Family Planning in Women With Mental DisordersAlmira PutriNo ratings yet
- Endometrial ThicknessDocument7 pagesEndometrial ThicknessAlmira PutriNo ratings yet
- ĐÁP ÁN TIẾNG ANH CHUYÊN NGÀNHDocument12 pagesĐÁP ÁN TIẾNG ANH CHUYÊN NGÀNHLinh PhạmNo ratings yet
- Enteric FeverDocument51 pagesEnteric FeverBinayaNo ratings yet
- Nasrudin, Hadi U, Vitanata, Erwin AT, Bramantono, Suharto, Dkk. Penyakit Infeksi Di Indonesia. Surabaya: Airlangga University Press, 2007Document4 pagesNasrudin, Hadi U, Vitanata, Erwin AT, Bramantono, Suharto, Dkk. Penyakit Infeksi Di Indonesia. Surabaya: Airlangga University Press, 2007Dwi SriNo ratings yet
- Enteric FeverDocument9 pagesEnteric FeverChetan NaikNo ratings yet
- Final PDFDocument31 pagesFinal PDFHimanshu BishtNo ratings yet
- WidalDocument31 pagesWidalghana faheemNo ratings yet
- Typhoid FeverDocument4 pagesTyphoid FeverBernice GyapongNo ratings yet
- Micro Lec Ars Sessions 17 23Document9 pagesMicro Lec Ars Sessions 17 23rica sebabillonesNo ratings yet
- Typhoid FeverDocument8 pagesTyphoid FeverMARIANTO PUTRA SUHARDINo ratings yet
- INFECTIOUSDocument36 pagesINFECTIOUSNathalie DeebNo ratings yet
- Debre Berhan University: College of Medicine and Health Science Department of Public Health EpidemiologyDocument41 pagesDebre Berhan University: College of Medicine and Health Science Department of Public Health EpidemiologyAgizew Endale100% (1)
- Medically Important Bacteria Memorisation SheetDocument7 pagesMedically Important Bacteria Memorisation SheetOlivia LimNo ratings yet
- Typhidot AssayDocument16 pagesTyphidot Assaychocoholic potchiNo ratings yet
- Ms NP 3 Set ADocument15 pagesMs NP 3 Set AEnna EstrellaNo ratings yet
- Hospital Association MeetDocument34 pagesHospital Association MeetYagesh SharmaNo ratings yet
- Typhoid FeverDocument30 pagesTyphoid FeversakuarNo ratings yet
- Typhoid Disease: Group 4Document57 pagesTyphoid Disease: Group 4ajeng astiaNo ratings yet
- Typhoid FeverDocument2 pagesTyphoid FeverSarah BenjaminNo ratings yet
- NCM 112 Rle: A Case Study On: Typhoid FeverDocument17 pagesNCM 112 Rle: A Case Study On: Typhoid FeverMadelyn Serneo100% (1)
- The Nursing Assessment of Thypoid FeverDocument8 pagesThe Nursing Assessment of Thypoid FeverNilaiNo ratings yet
- Medical Laboratory SIWES Report For NigeDocument44 pagesMedical Laboratory SIWES Report For NigeODEYEMI STEPHEN0% (1)
- MT2 Group-3Document14 pagesMT2 Group-3Berdel PascoNo ratings yet
- General Awareness of Pathology With Special Reference To Typhoid DiseaseDocument41 pagesGeneral Awareness of Pathology With Special Reference To Typhoid DiseaseNiveditaPandeyNo ratings yet
- Solid Waste ManagementDocument40 pagesSolid Waste ManagementMark Jacartny TuyongNo ratings yet
- 7.systemic BacteriologyDocument88 pages7.systemic BacteriologyShimelis Teshome AyalnehNo ratings yet
- Phenotypic and Molecular Characterizations OF: Salmonella Species in EthiopiaDocument194 pagesPhenotypic and Molecular Characterizations OF: Salmonella Species in EthiopiaAmid CapmariNo ratings yet
- Salmonella ThesisDocument6 pagesSalmonella Thesisangieleeportland100% (2)
- Microbiological Food PoisoningDocument72 pagesMicrobiological Food PoisoningFadel Rajab Nugraha100% (1)
- NCMB 312 Lect Final NotesDocument16 pagesNCMB 312 Lect Final NotesAngie BaylonNo ratings yet
- Effectiveness of Tepid Sponge Compresses and Plaster Compresses On Children'S Fever Temperature TyphoidDocument11 pagesEffectiveness of Tepid Sponge Compresses and Plaster Compresses On Children'S Fever Temperature TyphoidAyasNo ratings yet