
Management of Upper GI Bleeding
Management of Upper GI Bleeding
You might also like
- Concept Map Worksheet Mary Richards Heart Failure Jasgou1752Document3 pagesConcept Map Worksheet Mary Richards Heart Failure Jasgou1752Jasmyn Rose100% (1)
- Pat 2 Medsurg1Document20 pagesPat 2 Medsurg1api-300849832No ratings yet
- CholestyramineDocument1 pageCholestyramineKatie McPeekNo ratings yet
- Final Case StudyDocument18 pagesFinal Case Studyapi-487702467100% (1)
- Hypokalemia PDFDocument1 pageHypokalemia PDFJanedear PasalNo ratings yet
- Medical Case of SurgeryDocument7 pagesMedical Case of SurgerysugisweNo ratings yet
- Dysthymia and CyclothymiaDocument9 pagesDysthymia and CyclothymiaNatnael0% (1)
- Upper Gastrointestinal Bleeding 2007Document43 pagesUpper Gastrointestinal Bleeding 2007Matthew ThompsonNo ratings yet
- NCP GeDocument14 pagesNCP GeSuluhTriUtomoNo ratings yet
- Case Presentation: Presented byDocument34 pagesCase Presentation: Presented byZahid AnwarNo ratings yet
- This Study Resource Was Shared Via: HypoparathyroidismDocument1 pageThis Study Resource Was Shared Via: HypoparathyroidismDeo FactuarNo ratings yet
- Fluid Volume Deficit Nursing ManagementDocument5 pagesFluid Volume Deficit Nursing ManagementA.No ratings yet
- V. Pathophysiology Modifiable: Non - ModifiableDocument2 pagesV. Pathophysiology Modifiable: Non - ModifiableMary Grace BanezNo ratings yet
- Diabetes Mellitus: Rasmussen NPR Concept PlanDocument1 pageDiabetes Mellitus: Rasmussen NPR Concept PlanRoshin TejeroNo ratings yet
- Diagnosis of Gastrointestinal Bleeding in AdultsDocument8 pagesDiagnosis of Gastrointestinal Bleeding in AdultsSaeed Al-YafeiNo ratings yet
- Electrolyte ImbalanceDocument4 pagesElectrolyte ImbalanceDoneva Lyn MedinaNo ratings yet
- Case 2 and 3 Q1Document3 pagesCase 2 and 3 Q1Jeffrey Ramos0% (1)
- Cs HemorrhoidsDocument9 pagesCs HemorrhoidsPearl Joy Diaz AnggotNo ratings yet
- Addison's Disease. FinalDocument10 pagesAddison's Disease. FinalAnn KelseaNo ratings yet
- Schematic Diag DMDocument1 pageSchematic Diag DMReynaKatNo ratings yet
- Cushing's SyndromeDocument5 pagesCushing's SyndromesummerduskNo ratings yet
- HTN EmergencyDocument11 pagesHTN EmergencyKaran ChhabraNo ratings yet
- Concept Map Worksheet Fatime Sanogo Jasgou1752Document1 pageConcept Map Worksheet Fatime Sanogo Jasgou1752Jasmyn RoseNo ratings yet
- Bleeding Peptic Ulcer Disease Case StudyDocument17 pagesBleeding Peptic Ulcer Disease Case StudyChino Dela Cruz100% (2)
- HyperphosphatemiaDocument2 pagesHyperphosphatemiatephNo ratings yet
- Nephrolithiasis Concept MapDocument1 pageNephrolithiasis Concept MapSebastianNo ratings yet
- Assessment and Management of Patients With Biliary DisordersDocument16 pagesAssessment and Management of Patients With Biliary DisordersJills JohnyNo ratings yet
- Pathophysiology of Portal HYPERTENSION PDFDocument11 pagesPathophysiology of Portal HYPERTENSION PDFCamilo VidalNo ratings yet
- Gallbladder HydropsDocument6 pagesGallbladder HydropsSaifulAnamNo ratings yet
- Pneumonperitoneum A Review of Nonsurgical Causes PDFDocument7 pagesPneumonperitoneum A Review of Nonsurgical Causes PDFDellysa Eka Nugraha TNo ratings yet
- CKD + HPN Concept Map DRAFTDocument1 pageCKD + HPN Concept Map DRAFTInah Floresta BesasNo ratings yet
- UGIBDocument5 pagesUGIBdwyane0033100% (1)
- RBC AliquotsDocument1 pageRBC AliquotsARIF AHAMMEDNo ratings yet
- Acute PyelonephritisDocument9 pagesAcute Pyelonephritistaekado-1No ratings yet
- Betahistine Drug InfoDocument3 pagesBetahistine Drug InfoAshish KarnNo ratings yet
- Chronic PyelonephritisDocument5 pagesChronic PyelonephritisIsak ShatikaNo ratings yet
- A Case of A 61/M Client With Upper Gastrointestinal Bleeding Secondary To Peptic Ulcer DiseaseDocument3 pagesA Case of A 61/M Client With Upper Gastrointestinal Bleeding Secondary To Peptic Ulcer DiseasejohndavennarvaezNo ratings yet
- Chronic GastritisDocument37 pagesChronic GastritisBondu Babu007No ratings yet
- Prepared By: Rashmi Regmi B. SC Nursing Manmohan Memorial Institute of Health SciencesDocument93 pagesPrepared By: Rashmi Regmi B. SC Nursing Manmohan Memorial Institute of Health SciencesNinaNo ratings yet
- The Correlation Between Disease Stage and Pulmonary Edema Assessed With Chest Xray in Chronic Kidney Disease PatientsDocument6 pagesThe Correlation Between Disease Stage and Pulmonary Edema Assessed With Chest Xray in Chronic Kidney Disease PatientsAnnisa RabbaniNo ratings yet
- Malignant Neoplasm (Ovarian Cancer)Document4 pagesMalignant Neoplasm (Ovarian Cancer)nursing concept mapsNo ratings yet
- Liver Cirrhosis Care PlanDocument3 pagesLiver Cirrhosis Care PlanWendy EscalanteNo ratings yet
- Bowel ObstructionDocument6 pagesBowel ObstructionKryza Dale Bunado BaticanNo ratings yet
- NCP PainDocument2 pagesNCP PainApril_Ivy_Raga_3835No ratings yet
- Chronic GastritisDocument7 pagesChronic GastritisDivina AquinoNo ratings yet
- Gastrointestinal BleedingDocument24 pagesGastrointestinal BleedingGunawan Cahyo SNo ratings yet
- Dr. Sunatrio - Management Hypovolemic ShockDocument59 pagesDr. Sunatrio - Management Hypovolemic ShockArga Putra SaboeNo ratings yet
- Chapter54 Management of Patients With Kidney DisordersDocument40 pagesChapter54 Management of Patients With Kidney Disordersjericho dinglasanNo ratings yet
- HemorrhoidectomyDocument5 pagesHemorrhoidectomydrnareshkumar3281100% (1)
- BSN4D-SG2 DM Type2Document201 pagesBSN4D-SG2 DM Type2Charisse CaydanNo ratings yet
- Renal Case Study Final1Document41 pagesRenal Case Study Final1api-202881815100% (1)
- Ascending CholangitisDocument7 pagesAscending CholangitisAmar HasanNo ratings yet
- NCP UgibDocument4 pagesNCP UgibErnest Brian FernandezNo ratings yet
- Management of Patients With Intestinal and Rectal DisordersDocument33 pagesManagement of Patients With Intestinal and Rectal DisordersDoneva Lyn MedinaNo ratings yet
- Schematic DiagramDocument3 pagesSchematic Diagramrn msnNo ratings yet
- Abdominal Distension: Common Causes: - (Five F'S) 1. 2. 3. 4. 5. History of Present Illness 1Document3 pagesAbdominal Distension: Common Causes: - (Five F'S) 1. 2. 3. 4. 5. History of Present Illness 1Maxamed DananNo ratings yet
- Nursing Management Pancreatic CancerDocument2 pagesNursing Management Pancreatic CancerKit NameKo100% (2)
- CPG On AID PPT PresentationDocument83 pagesCPG On AID PPT Presentationsharmaine peroNo ratings yet
- Upper GIT BleedDocument4 pagesUpper GIT BleedRed DevilNo ratings yet
- Acute and Chronic Gastrointestinal BleedingDocument7 pagesAcute and Chronic Gastrointestinal BleedingMarwan M.100% (1)
- Upper Gastrointestinal Bleeding (Ugib) : Muhammad Izzat Bin FatasDocument47 pagesUpper Gastrointestinal Bleeding (Ugib) : Muhammad Izzat Bin FatascopperNo ratings yet
- Acute Cholecystitis SeminarDocument42 pagesAcute Cholecystitis SeminarNatnaelNo ratings yet
- Acute Cholecystitis SeminarDocument42 pagesAcute Cholecystitis SeminarNatnaelNo ratings yet
- Hypothermia and HyperthermiaDocument17 pagesHypothermia and HyperthermiaNatnaelNo ratings yet
- Cervical Intraepithelial Neoplasia and Cervical CancerDocument28 pagesCervical Intraepithelial Neoplasia and Cervical CancerNatnael100% (1)
- Pediatrics Study ScheduleDocument2 pagesPediatrics Study ScheduleNatnaelNo ratings yet
- Increase: Are Even More ComplicationsDocument5 pagesIncrease: Are Even More ComplicationsNatnaelNo ratings yet
- Ectopic PregnancyDocument24 pagesEctopic PregnancyNatnaelNo ratings yet
- Total PresentationDocument22 pagesTotal PresentationNatnaelNo ratings yet
- Body's Normal Flora:: ScavengersDocument4 pagesBody's Normal Flora:: ScavengersNatnaelNo ratings yet
- Vit A DeficiencyDocument27 pagesVit A DeficiencyNatnaelNo ratings yet
- Anterior Segment ManifestationDocument25 pagesAnterior Segment ManifestationNatnaelNo ratings yet
- The Physiology of Human Sexual Act (Final)Document16 pagesThe Physiology of Human Sexual Act (Final)NatnaelNo ratings yet
- Diencephalon PhysiologyDocument36 pagesDiencephalon PhysiologyNatnael0% (1)
- Syrgery Mock 10Document8 pagesSyrgery Mock 10Sergiu CiobanuNo ratings yet
- Autacoids and Related DrugsDocument17 pagesAutacoids and Related DrugsmidhunNo ratings yet
- Abdominal PainDocument7 pagesAbdominal PainKartikey ChauhanNo ratings yet
- Richard Baron, An Introduction To Medical Phenomenology, Ann Int Med, 1985Document6 pagesRichard Baron, An Introduction To Medical Phenomenology, Ann Int Med, 1985Aymar Hachero JoaquínNo ratings yet
- Abdominal Pain History TakingDocument8 pagesAbdominal Pain History TakingParth PatelNo ratings yet
- Clinical Report AdlucemDocument23 pagesClinical Report AdlucemSilver DrakeNo ratings yet
- Fischer's CramathonDocument3 pagesFischer's CramathonRaymond KwokNo ratings yet
- Taking Medical HistoryDocument2 pagesTaking Medical HistoryDiana KulsumNo ratings yet
- Peptic Ulcer Disease (PUD)Document32 pagesPeptic Ulcer Disease (PUD)Ali AlyahawiNo ratings yet
- Notes Muscle Relaxants Part 3Document62 pagesNotes Muscle Relaxants Part 3Charlotte FabrosNo ratings yet
- Peptic Ulcer Disease 2019Document2 pagesPeptic Ulcer Disease 2019DrhussamNo ratings yet
- List of Common Drugs-UpdatedDocument29 pagesList of Common Drugs-UpdatedPaul Benjomin AgregadoNo ratings yet
- Eng 2005 MedDocument43 pagesEng 2005 MedLucia BogNo ratings yet
- MCQsDocument290 pagesMCQsTaima Fayez100% (4)
- 50 Item Gastrointestinal Health Problems Test Drill KeysDocument14 pages50 Item Gastrointestinal Health Problems Test Drill KeysmervilynNo ratings yet
- PARIET 20mg - Summary of Product Characteristics (SMPC) - Print Friendly - (Emc)Document9 pagesPARIET 20mg - Summary of Product Characteristics (SMPC) - Print Friendly - (Emc)Abdullah Al MamunNo ratings yet
- Tanaman 2Document10 pagesTanaman 2Mohamad YasinNo ratings yet
- Case Study On Acute Gastritis: T Villanueva Avenue, Naga CityDocument26 pagesCase Study On Acute Gastritis: T Villanueva Avenue, Naga CityMark Jefferson LunaNo ratings yet
- Case Presentation Peptic Ulcer: Ma. Christina T. Alvarez Wup - Bs Nursing Iii-2Document18 pagesCase Presentation Peptic Ulcer: Ma. Christina T. Alvarez Wup - Bs Nursing Iii-2Shane Aileen AngelesNo ratings yet
- Practice Questions GastroDocument31 pagesPractice Questions GastroGEN COLLANTESNo ratings yet
- Instruct To Avoid Drinking Alcohol While Taking This MedicationDocument6 pagesInstruct To Avoid Drinking Alcohol While Taking This MedicationMonica BorjaNo ratings yet
- Instant Download PDF Linear Algebra A Modern Introduction 4th Edition David Poole Solutions Manual Full ChapterDocument24 pagesInstant Download PDF Linear Algebra A Modern Introduction 4th Edition David Poole Solutions Manual Full Chaptersaaverfgiiu1100% (5)
- Prevalence of Helicobacter Pylori Infection AmongDocument77 pagesPrevalence of Helicobacter Pylori Infection AmongAbigailNo ratings yet
- Amoxil 3Document9 pagesAmoxil 3sisnaingaungNo ratings yet
- Teaching Regarding Measures To Improve Sleep?Document37 pagesTeaching Regarding Measures To Improve Sleep?Martin HusseinNo ratings yet
- Drugs For Digestive Disorders PDFDocument41 pagesDrugs For Digestive Disorders PDFNoreak SokNo ratings yet
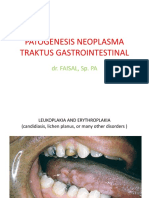
- Patogenesis Neoplasma Traktus Gastrointestinal: Dr. FAISAL, Sp. PADocument42 pagesPatogenesis Neoplasma Traktus Gastrointestinal: Dr. FAISAL, Sp. PAmitasushNo ratings yet
- $RUEZRZJDocument10 pages$RUEZRZJJc GaldosNo ratings yet
- 5149 4 Helicobacter PyloriDocument3 pages5149 4 Helicobacter PyloriMachira MuturiNo ratings yet
- Chronic GastroduodenitisDocument6 pagesChronic GastroduodenitisIvanNo ratings yet





































































































Download as pdf or txt
You might also like
- Concept Map Worksheet Mary Richards Heart Failure Jasgou1752Document3 pagesConcept Map Worksheet Mary Richards Heart Failure Jasgou1752Jasmyn Rose100% (1)
- Pat 2 Medsurg1Document20 pagesPat 2 Medsurg1api-300849832No ratings yet
- CholestyramineDocument1 pageCholestyramineKatie McPeekNo ratings yet
- Final Case StudyDocument18 pagesFinal Case Studyapi-487702467100% (1)
- Hypokalemia PDFDocument1 pageHypokalemia PDFJanedear PasalNo ratings yet
- Medical Case of SurgeryDocument7 pagesMedical Case of SurgerysugisweNo ratings yet
- Dysthymia and CyclothymiaDocument9 pagesDysthymia and CyclothymiaNatnael0% (1)
- Upper Gastrointestinal Bleeding 2007Document43 pagesUpper Gastrointestinal Bleeding 2007Matthew ThompsonNo ratings yet
- NCP GeDocument14 pagesNCP GeSuluhTriUtomoNo ratings yet
- Case Presentation: Presented byDocument34 pagesCase Presentation: Presented byZahid AnwarNo ratings yet
- This Study Resource Was Shared Via: HypoparathyroidismDocument1 pageThis Study Resource Was Shared Via: HypoparathyroidismDeo FactuarNo ratings yet
- Fluid Volume Deficit Nursing ManagementDocument5 pagesFluid Volume Deficit Nursing ManagementA.No ratings yet
- V. Pathophysiology Modifiable: Non - ModifiableDocument2 pagesV. Pathophysiology Modifiable: Non - ModifiableMary Grace BanezNo ratings yet
- Diabetes Mellitus: Rasmussen NPR Concept PlanDocument1 pageDiabetes Mellitus: Rasmussen NPR Concept PlanRoshin TejeroNo ratings yet
- Diagnosis of Gastrointestinal Bleeding in AdultsDocument8 pagesDiagnosis of Gastrointestinal Bleeding in AdultsSaeed Al-YafeiNo ratings yet
- Electrolyte ImbalanceDocument4 pagesElectrolyte ImbalanceDoneva Lyn MedinaNo ratings yet
- Case 2 and 3 Q1Document3 pagesCase 2 and 3 Q1Jeffrey Ramos0% (1)
- Cs HemorrhoidsDocument9 pagesCs HemorrhoidsPearl Joy Diaz AnggotNo ratings yet
- Addison's Disease. FinalDocument10 pagesAddison's Disease. FinalAnn KelseaNo ratings yet
- Schematic Diag DMDocument1 pageSchematic Diag DMReynaKatNo ratings yet
- Cushing's SyndromeDocument5 pagesCushing's SyndromesummerduskNo ratings yet
- HTN EmergencyDocument11 pagesHTN EmergencyKaran ChhabraNo ratings yet
- Concept Map Worksheet Fatime Sanogo Jasgou1752Document1 pageConcept Map Worksheet Fatime Sanogo Jasgou1752Jasmyn RoseNo ratings yet
- Bleeding Peptic Ulcer Disease Case StudyDocument17 pagesBleeding Peptic Ulcer Disease Case StudyChino Dela Cruz100% (2)
- HyperphosphatemiaDocument2 pagesHyperphosphatemiatephNo ratings yet
- Nephrolithiasis Concept MapDocument1 pageNephrolithiasis Concept MapSebastianNo ratings yet
- Assessment and Management of Patients With Biliary DisordersDocument16 pagesAssessment and Management of Patients With Biliary DisordersJills JohnyNo ratings yet
- Pathophysiology of Portal HYPERTENSION PDFDocument11 pagesPathophysiology of Portal HYPERTENSION PDFCamilo VidalNo ratings yet
- Gallbladder HydropsDocument6 pagesGallbladder HydropsSaifulAnamNo ratings yet
- Pneumonperitoneum A Review of Nonsurgical Causes PDFDocument7 pagesPneumonperitoneum A Review of Nonsurgical Causes PDFDellysa Eka Nugraha TNo ratings yet
- CKD + HPN Concept Map DRAFTDocument1 pageCKD + HPN Concept Map DRAFTInah Floresta BesasNo ratings yet
- UGIBDocument5 pagesUGIBdwyane0033100% (1)
- RBC AliquotsDocument1 pageRBC AliquotsARIF AHAMMEDNo ratings yet
- Acute PyelonephritisDocument9 pagesAcute Pyelonephritistaekado-1No ratings yet
- Betahistine Drug InfoDocument3 pagesBetahistine Drug InfoAshish KarnNo ratings yet
- Chronic PyelonephritisDocument5 pagesChronic PyelonephritisIsak ShatikaNo ratings yet
- A Case of A 61/M Client With Upper Gastrointestinal Bleeding Secondary To Peptic Ulcer DiseaseDocument3 pagesA Case of A 61/M Client With Upper Gastrointestinal Bleeding Secondary To Peptic Ulcer DiseasejohndavennarvaezNo ratings yet
- Chronic GastritisDocument37 pagesChronic GastritisBondu Babu007No ratings yet
- Prepared By: Rashmi Regmi B. SC Nursing Manmohan Memorial Institute of Health SciencesDocument93 pagesPrepared By: Rashmi Regmi B. SC Nursing Manmohan Memorial Institute of Health SciencesNinaNo ratings yet
- The Correlation Between Disease Stage and Pulmonary Edema Assessed With Chest Xray in Chronic Kidney Disease PatientsDocument6 pagesThe Correlation Between Disease Stage and Pulmonary Edema Assessed With Chest Xray in Chronic Kidney Disease PatientsAnnisa RabbaniNo ratings yet
- Malignant Neoplasm (Ovarian Cancer)Document4 pagesMalignant Neoplasm (Ovarian Cancer)nursing concept mapsNo ratings yet
- Liver Cirrhosis Care PlanDocument3 pagesLiver Cirrhosis Care PlanWendy EscalanteNo ratings yet
- Bowel ObstructionDocument6 pagesBowel ObstructionKryza Dale Bunado BaticanNo ratings yet
- NCP PainDocument2 pagesNCP PainApril_Ivy_Raga_3835No ratings yet
- Chronic GastritisDocument7 pagesChronic GastritisDivina AquinoNo ratings yet
- Gastrointestinal BleedingDocument24 pagesGastrointestinal BleedingGunawan Cahyo SNo ratings yet
- Dr. Sunatrio - Management Hypovolemic ShockDocument59 pagesDr. Sunatrio - Management Hypovolemic ShockArga Putra SaboeNo ratings yet
- Chapter54 Management of Patients With Kidney DisordersDocument40 pagesChapter54 Management of Patients With Kidney Disordersjericho dinglasanNo ratings yet
- HemorrhoidectomyDocument5 pagesHemorrhoidectomydrnareshkumar3281100% (1)
- BSN4D-SG2 DM Type2Document201 pagesBSN4D-SG2 DM Type2Charisse CaydanNo ratings yet
- Renal Case Study Final1Document41 pagesRenal Case Study Final1api-202881815100% (1)
- Ascending CholangitisDocument7 pagesAscending CholangitisAmar HasanNo ratings yet
- NCP UgibDocument4 pagesNCP UgibErnest Brian FernandezNo ratings yet
- Management of Patients With Intestinal and Rectal DisordersDocument33 pagesManagement of Patients With Intestinal and Rectal DisordersDoneva Lyn MedinaNo ratings yet
- Schematic DiagramDocument3 pagesSchematic Diagramrn msnNo ratings yet
- Abdominal Distension: Common Causes: - (Five F'S) 1. 2. 3. 4. 5. History of Present Illness 1Document3 pagesAbdominal Distension: Common Causes: - (Five F'S) 1. 2. 3. 4. 5. History of Present Illness 1Maxamed DananNo ratings yet
- Nursing Management Pancreatic CancerDocument2 pagesNursing Management Pancreatic CancerKit NameKo100% (2)
- CPG On AID PPT PresentationDocument83 pagesCPG On AID PPT Presentationsharmaine peroNo ratings yet
- Upper GIT BleedDocument4 pagesUpper GIT BleedRed DevilNo ratings yet
- Acute and Chronic Gastrointestinal BleedingDocument7 pagesAcute and Chronic Gastrointestinal BleedingMarwan M.100% (1)
- Upper Gastrointestinal Bleeding (Ugib) : Muhammad Izzat Bin FatasDocument47 pagesUpper Gastrointestinal Bleeding (Ugib) : Muhammad Izzat Bin FatascopperNo ratings yet
- Acute Cholecystitis SeminarDocument42 pagesAcute Cholecystitis SeminarNatnaelNo ratings yet
- Acute Cholecystitis SeminarDocument42 pagesAcute Cholecystitis SeminarNatnaelNo ratings yet
- Hypothermia and HyperthermiaDocument17 pagesHypothermia and HyperthermiaNatnaelNo ratings yet
- Cervical Intraepithelial Neoplasia and Cervical CancerDocument28 pagesCervical Intraepithelial Neoplasia and Cervical CancerNatnael100% (1)
- Pediatrics Study ScheduleDocument2 pagesPediatrics Study ScheduleNatnaelNo ratings yet
- Increase: Are Even More ComplicationsDocument5 pagesIncrease: Are Even More ComplicationsNatnaelNo ratings yet
- Ectopic PregnancyDocument24 pagesEctopic PregnancyNatnaelNo ratings yet
- Total PresentationDocument22 pagesTotal PresentationNatnaelNo ratings yet
- Body's Normal Flora:: ScavengersDocument4 pagesBody's Normal Flora:: ScavengersNatnaelNo ratings yet
- Vit A DeficiencyDocument27 pagesVit A DeficiencyNatnaelNo ratings yet
- Anterior Segment ManifestationDocument25 pagesAnterior Segment ManifestationNatnaelNo ratings yet
- The Physiology of Human Sexual Act (Final)Document16 pagesThe Physiology of Human Sexual Act (Final)NatnaelNo ratings yet
- Diencephalon PhysiologyDocument36 pagesDiencephalon PhysiologyNatnael0% (1)
- Syrgery Mock 10Document8 pagesSyrgery Mock 10Sergiu CiobanuNo ratings yet
- Autacoids and Related DrugsDocument17 pagesAutacoids and Related DrugsmidhunNo ratings yet
- Abdominal PainDocument7 pagesAbdominal PainKartikey ChauhanNo ratings yet
- Richard Baron, An Introduction To Medical Phenomenology, Ann Int Med, 1985Document6 pagesRichard Baron, An Introduction To Medical Phenomenology, Ann Int Med, 1985Aymar Hachero JoaquínNo ratings yet
- Abdominal Pain History TakingDocument8 pagesAbdominal Pain History TakingParth PatelNo ratings yet
- Clinical Report AdlucemDocument23 pagesClinical Report AdlucemSilver DrakeNo ratings yet
- Fischer's CramathonDocument3 pagesFischer's CramathonRaymond KwokNo ratings yet
- Taking Medical HistoryDocument2 pagesTaking Medical HistoryDiana KulsumNo ratings yet
- Peptic Ulcer Disease (PUD)Document32 pagesPeptic Ulcer Disease (PUD)Ali AlyahawiNo ratings yet
- Notes Muscle Relaxants Part 3Document62 pagesNotes Muscle Relaxants Part 3Charlotte FabrosNo ratings yet
- Peptic Ulcer Disease 2019Document2 pagesPeptic Ulcer Disease 2019DrhussamNo ratings yet
- List of Common Drugs-UpdatedDocument29 pagesList of Common Drugs-UpdatedPaul Benjomin AgregadoNo ratings yet
- Eng 2005 MedDocument43 pagesEng 2005 MedLucia BogNo ratings yet
- MCQsDocument290 pagesMCQsTaima Fayez100% (4)
- 50 Item Gastrointestinal Health Problems Test Drill KeysDocument14 pages50 Item Gastrointestinal Health Problems Test Drill KeysmervilynNo ratings yet
- PARIET 20mg - Summary of Product Characteristics (SMPC) - Print Friendly - (Emc)Document9 pagesPARIET 20mg - Summary of Product Characteristics (SMPC) - Print Friendly - (Emc)Abdullah Al MamunNo ratings yet
- Tanaman 2Document10 pagesTanaman 2Mohamad YasinNo ratings yet
- Case Study On Acute Gastritis: T Villanueva Avenue, Naga CityDocument26 pagesCase Study On Acute Gastritis: T Villanueva Avenue, Naga CityMark Jefferson LunaNo ratings yet
- Case Presentation Peptic Ulcer: Ma. Christina T. Alvarez Wup - Bs Nursing Iii-2Document18 pagesCase Presentation Peptic Ulcer: Ma. Christina T. Alvarez Wup - Bs Nursing Iii-2Shane Aileen AngelesNo ratings yet
- Practice Questions GastroDocument31 pagesPractice Questions GastroGEN COLLANTESNo ratings yet
- Instruct To Avoid Drinking Alcohol While Taking This MedicationDocument6 pagesInstruct To Avoid Drinking Alcohol While Taking This MedicationMonica BorjaNo ratings yet
- Instant Download PDF Linear Algebra A Modern Introduction 4th Edition David Poole Solutions Manual Full ChapterDocument24 pagesInstant Download PDF Linear Algebra A Modern Introduction 4th Edition David Poole Solutions Manual Full Chaptersaaverfgiiu1100% (5)
- Prevalence of Helicobacter Pylori Infection AmongDocument77 pagesPrevalence of Helicobacter Pylori Infection AmongAbigailNo ratings yet
- Amoxil 3Document9 pagesAmoxil 3sisnaingaungNo ratings yet
- Teaching Regarding Measures To Improve Sleep?Document37 pagesTeaching Regarding Measures To Improve Sleep?Martin HusseinNo ratings yet
- Drugs For Digestive Disorders PDFDocument41 pagesDrugs For Digestive Disorders PDFNoreak SokNo ratings yet
- Patogenesis Neoplasma Traktus Gastrointestinal: Dr. FAISAL, Sp. PADocument42 pagesPatogenesis Neoplasma Traktus Gastrointestinal: Dr. FAISAL, Sp. PAmitasushNo ratings yet
- $RUEZRZJDocument10 pages$RUEZRZJJc GaldosNo ratings yet
- 5149 4 Helicobacter PyloriDocument3 pages5149 4 Helicobacter PyloriMachira MuturiNo ratings yet
- Chronic GastroduodenitisDocument6 pagesChronic GastroduodenitisIvanNo ratings yet