Download as docx, pdf, or txt
You might also like
- Gynecology PDFDocument18 pagesGynecology PDFKatheryn100% (2)
- Suture Practice Kit Ebook PDFDocument18 pagesSuture Practice Kit Ebook PDFKarla Aguilar GuerreroNo ratings yet
- TeratologyDocument34 pagesTeratologyธิติวุฒิ แสงคล้อย100% (1)
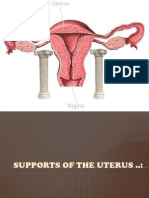
- Supports of The UterusDocument20 pagesSupports of The UterusAshwin Prem Solomon100% (1)
- Office Gynecology: Princess Cony CayabaDocument60 pagesOffice Gynecology: Princess Cony CayabaCarla Dela CruzNo ratings yet
- Pelvic Examiantion: BY: Charisse Ann G. GasatayaDocument27 pagesPelvic Examiantion: BY: Charisse Ann G. GasatayaCharisse Ann GasatayaNo ratings yet
- InfertilityDocument14 pagesInfertilityDrChauhanNo ratings yet
- Obstetrics PDFDocument14 pagesObstetrics PDFKatheryn100% (1)
- Physiology of LaborDocument49 pagesPhysiology of LaborGunung MahameruNo ratings yet
- 1-Obs&Gynae - Anatomy and Embryology of The Female Reproductive SystemDocument52 pages1-Obs&Gynae - Anatomy and Embryology of The Female Reproductive Systemfadiawwad100% (4)
- Physiological Changes of PregnancyDocument40 pagesPhysiological Changes of PregnancyAita AladianseNo ratings yet
- AmenorrheaDocument23 pagesAmenorrheaKarmmanya Razahani PurnamaNo ratings yet
- ObGyn Board Review PDFDocument85 pagesObGyn Board Review PDFCoolrobertizNo ratings yet
- Benign Gynecologic Lesions FinalDocument11 pagesBenign Gynecologic Lesions Final2012100% (4)
- 62 Lecture Menstrual Cycle Abnormalities, Infertility, MenopauseDocument69 pages62 Lecture Menstrual Cycle Abnormalities, Infertility, MenopauseTarek TarekNo ratings yet
- Blood Supply Pelvic OrgansDocument39 pagesBlood Supply Pelvic OrgansoliviaNo ratings yet
- Benign & Precancerous Tumors of Female Genital Organs: by Assist. O.V.BakunDocument83 pagesBenign & Precancerous Tumors of Female Genital Organs: by Assist. O.V.BakunDian Permata PutraNo ratings yet
- Benign Disease of The UterusDocument27 pagesBenign Disease of The UterusnyangaraNo ratings yet
- Early Pregnancy Complications: Ectopic Pregnancy Gestational Trophoblastic Disease Ji Aggasid, JanniecelDocument60 pagesEarly Pregnancy Complications: Ectopic Pregnancy Gestational Trophoblastic Disease Ji Aggasid, JanniecelmedicoNo ratings yet
- Total Abdominal Hysterectomy and Bilateral Salpingo-OophorectomyDocument12 pagesTotal Abdominal Hysterectomy and Bilateral Salpingo-OophorectomyBadri KobalavaNo ratings yet
- Diagnosis and Management of Pelvic Organ ProlapseDocument47 pagesDiagnosis and Management of Pelvic Organ ProlapseWindy Puspa Kusumah100% (1)
- MHN TerminologyDocument27 pagesMHN Terminologydonb27529No ratings yet
- Stroke & Hemiplegia LocalizationDocument54 pagesStroke & Hemiplegia LocalizationVasu PottabatthiniNo ratings yet
- OBGYN Clinical RotationDocument5 pagesOBGYN Clinical Rotationriczen mae vilaNo ratings yet
- Aquifer Case - Summary - FamilyMedicine17 - 55-YDocument9 pagesAquifer Case - Summary - FamilyMedicine17 - 55-YHyunsoo EllisNo ratings yet
- Management of Labor and DeliveryFrom EverandManagement of Labor and DeliveryGeorge A. MaconesNo ratings yet
- Prenatal Assessments by TrimesterDocument6 pagesPrenatal Assessments by TrimesterMauZungNo ratings yet
- Pediatric HistoryDocument96 pagesPediatric Historyapi-3712326100% (2)
- Neurofibromatosis in PregnancyDocument2 pagesNeurofibromatosis in PregnancyDwi Wahyu AprianiNo ratings yet
- Obs History Taking FormatDocument24 pagesObs History Taking FormatBibek PandeyNo ratings yet
- Understanding Basic Obstetrics and GynaecologyDocument60 pagesUnderstanding Basic Obstetrics and GynaecologyleaslimNo ratings yet
- Intraepithelial Neoplasia of The Lower Genital TractDocument54 pagesIntraepithelial Neoplasia of The Lower Genital TractDee Sarajan100% (1)
- Cesarean Section: Associate Professor Ph.D. E.A. EinyshDocument33 pagesCesarean Section: Associate Professor Ph.D. E.A. EinyshPrerit Aggarwal100% (1)
- Gynecology Abnormal Bleeding 2014aDocument8 pagesGynecology Abnormal Bleeding 2014aBhi-An BatobalonosNo ratings yet
- Obgyn Osce - Ob HistoryDocument3 pagesObgyn Osce - Ob HistoryErika Leah ManaloNo ratings yet
- Pulmonary Disorders in PregnancyDocument49 pagesPulmonary Disorders in PregnancyMara Medina - BorleoNo ratings yet
- Genital ProlapseDocument13 pagesGenital ProlapsesmbawasainiNo ratings yet
- Vaginal Bleeding in Pregnancy - 5-Minute Emergency ConsultDocument6 pagesVaginal Bleeding in Pregnancy - 5-Minute Emergency ConsultLaoMed plusNo ratings yet
- History TakingDocument26 pagesHistory TakingShauie CayabyabNo ratings yet
- (New) Early Pregnancy Complications RDocument51 pages(New) Early Pregnancy Complications RMesk Banat100% (2)
- Menopause NotesDocument5 pagesMenopause NotesJU WSD100% (1)
- Endometriosis GuidelineDocument44 pagesEndometriosis GuidelineHen DriNo ratings yet
- Reproductive Endocrinology FinalDocument98 pagesReproductive Endocrinology FinalChino Paolo SamsonNo ratings yet
- Examination of The Sensory SystemDocument17 pagesExamination of The Sensory SystemPaulo Henrique Neto Pais100% (1)
- Gynecology: 3.09 - AmenorrheaDocument13 pagesGynecology: 3.09 - AmenorrheaAnna Mae MarantanNo ratings yet
- Congenital Malformations of The Female Genital TractDocument7 pagesCongenital Malformations of The Female Genital TractDo le QuangNo ratings yet
- Leah M. Schenk, MD Infertility Reproductive EndocrinologyDocument2 pagesLeah M. Schenk, MD Infertility Reproductive EndocrinologyLeah M. Schenk MD100% (2)
- Management Normal Labor 2021 SBOGDocument118 pagesManagement Normal Labor 2021 SBOGAHMED .KNo ratings yet
- Amenorrhea - Algorithm & DifferentialsDocument9 pagesAmenorrhea - Algorithm & DifferentialsItharshan IndreswaranNo ratings yet
- Disorders of the Patellofemoral Joint: Diagnosis and ManagementFrom EverandDisorders of the Patellofemoral Joint: Diagnosis and ManagementNo ratings yet
- Obgyn Osce - Breast ExaminationDocument2 pagesObgyn Osce - Breast ExaminationErika Leah ManaloNo ratings yet
- Nursing Abdominal AssessmentDocument5 pagesNursing Abdominal AssessmentPatricia G ChiuNo ratings yet
- Pelvic ExaminationDocument24 pagesPelvic ExaminationVictor SantawiNo ratings yet
- Skills Demo Guide For ClerksDocument11 pagesSkills Demo Guide For ClerksMariana B.No ratings yet
- Pelvic Examination: W - Newton LongDocument3 pagesPelvic Examination: W - Newton LongyuexinchongNo ratings yet
- Per Vaginal ExaminationDocument25 pagesPer Vaginal Examinationazulqaidah95No ratings yet
- 2021.2 - GYNE Written-AnswersDocument113 pages2021.2 - GYNE Written-AnswersLucas Victor AlmeidaNo ratings yet
- National College of Nursing: Procedure ONDocument6 pagesNational College of Nursing: Procedure ONSumit Yadav100% (1)
- Pulmonary DisorderDocument10 pagesPulmonary DisorderIke RilleraNo ratings yet
- Abnormal Labor, Dystocia IIDocument9 pagesAbnormal Labor, Dystocia IIIke RilleraNo ratings yet
- JaundiceDocument25 pagesJaundiceIke RilleraNo ratings yet
- Systemic Lupus ErythematosusDocument89 pagesSystemic Lupus ErythematosusIke RilleraNo ratings yet
- Phylum Aschelminthes - FormattedDocument30 pagesPhylum Aschelminthes - FormattedkingNo ratings yet
- ArrhythmiasDocument55 pagesArrhythmiasAzmi Ikhsan AzharyNo ratings yet
- Pediatrics Report Group 2 Feeding and NutritionDocument23 pagesPediatrics Report Group 2 Feeding and NutritionEd Daniel DavisNo ratings yet
- Management of Bleeding Disorders in Children - MannoDocument7 pagesManagement of Bleeding Disorders in Children - MannoRhiannon Bam OoiNo ratings yet
- Field Guide To Antibiotic StewardshipDocument30 pagesField Guide To Antibiotic StewardshipHosam GomaaNo ratings yet
- Avian EndosDocument15 pagesAvian EndosJosé Moreira Lima NetoNo ratings yet
- DocxDocument53 pagesDocxkuro hanabusaNo ratings yet
- Identification of Hemoglobin Varients Through HPLCDocument42 pagesIdentification of Hemoglobin Varients Through HPLCJohnNo ratings yet
- FNA CCX Ovojnice, CSF, KŽ Za Miru 2020 - gs15FDocument194 pagesFNA CCX Ovojnice, CSF, KŽ Za Miru 2020 - gs15FGoran SimicNo ratings yet
- Hand Hygiene Research PaperDocument3 pagesHand Hygiene Research PaperEd SllenNo ratings yet
- JoDD 17-1 26-37 Schroeder Et AlDocument12 pagesJoDD 17-1 26-37 Schroeder Et AlEspíritu Ciudadano100% (1)
- Mental Health Testu3Document5 pagesMental Health Testu3clarheenaNo ratings yet
- Folinic AcidDocument1 pageFolinic AcidMuhammad ArsalanNo ratings yet
- Lumbar Assessment Form FILLABLE Jun 2020Document2 pagesLumbar Assessment Form FILLABLE Jun 2020FejesNo ratings yet
- Test Drill OBDocument8 pagesTest Drill OBViviane Ńíáshéè Basod100% (1)
- Of Client Having A Nephrectomy: Nursing CareDocument1 pageOf Client Having A Nephrectomy: Nursing CareJayshree ParmarNo ratings yet
- Pneumonia: Meningococcal Pneumonia: A ReviewDocument13 pagesPneumonia: Meningococcal Pneumonia: A ReviewRizki Handayani SiregarNo ratings yet
- Graphic Organiser FactorDocument2 pagesGraphic Organiser FactorRogini SindhuNo ratings yet
- Practical Manual 171Document85 pagesPractical Manual 171Souvik Roy Chowdhury100% (1)
- Biodiversity and Ecosystem ServicesDocument30 pagesBiodiversity and Ecosystem ServicesNick NgNo ratings yet
- Icd 11 Introduction ClinicalDocument50 pagesIcd 11 Introduction ClinicalMuhammad Farooq Ul HassanNo ratings yet
- Vaginal Fungal InfectionsDocument15 pagesVaginal Fungal InfectionsBalsc Bals BalscNo ratings yet
- Toxicology Case Studies Carbon MonoxideDocument5 pagesToxicology Case Studies Carbon MonoxideMark Jayson T. AsinoNo ratings yet
- Biological Classification Class 11Document13 pagesBiological Classification Class 11abhhngouravNo ratings yet
- Diseases: Prevention of Progression in Myopia: A Systematic ReviewDocument25 pagesDiseases: Prevention of Progression in Myopia: A Systematic ReviewFauziah Dwi AprianiNo ratings yet
- Definitions and Reporting Framework For Tuberculosis - 2013 RevisionDocument47 pagesDefinitions and Reporting Framework For Tuberculosis - 2013 RevisionDavien UtoyoNo ratings yet
- Poster Session v3Document11 pagesPoster Session v3Fiola FinandakasihNo ratings yet
- Body World's 1 Running Head: BODY WORLDS EXHIBITDocument5 pagesBody World's 1 Running Head: BODY WORLDS EXHIBITiamruthannNo ratings yet
- Remedi KA6 Slides - Client PPT - Remedi IndiaDocument34 pagesRemedi KA6 Slides - Client PPT - Remedi IndiaSupport InvimedsNo ratings yet
- A Whole-Of-Nation Approach To COVID-19 Taiwan's National Epidemic Prevention TeamDocument16 pagesA Whole-Of-Nation Approach To COVID-19 Taiwan's National Epidemic Prevention Teamgrahma96No ratings yet