Professional Documents
Culture Documents
Imaging of Chopart (Midtarsal) Joint Complex: Normal Anatomy and Posttraumatic Findings
Imaging of Chopart (Midtarsal) Joint Complex: Normal Anatomy and Posttraumatic Findings
Uploaded by
Edgar Bonifacio Chay ChayOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Imaging of Chopart (Midtarsal) Joint Complex: Normal Anatomy and Posttraumatic Findings
Imaging of Chopart (Midtarsal) Joint Complex: Normal Anatomy and Posttraumatic Findings
Uploaded by
Edgar Bonifacio Chay ChayCopyright:
Available Formats
M u s c u l o s k e l e t a l I m a g i n g • R ev i ew
Walter et al.
Chopart Joint Complex
Musculoskeletal Imaging
Review
Imaging of Chopart (Midtarsal)
Joint Complex: Normal Anatomy
and Posttraumatic Findings
William R. Walter 1 OBJECTIVE. The objective of this article is to review the normal anatomy and posttrau-
Anna Hirschmann2 matic findings of the Chopart joint complex. Key imaging features of the normal ligaments
Monica Tafur 3 and patterns of ligamentous and osseous injuries are discussed.
Zehava S. Rosenberg1 CONCLUSION. Traumatic midtarsal injuries, particularly midtarsal sprain, are often
overlooked clinically and on imaging but are relatively common and typically are associated
Walter WR, Hirschmann A, Tafur M, Rosenberg ZS with inversion ankle injuries. Radiologists should be familiar with Chopart joint anatomy
and the imaging features of midtarsal injuries because early diagnosis may help optimize
clinical management.
idtarsal sprains are defined as a tion, in part because of unfamiliarity with
M
American Journal of Roentgenology
spectrum of soft-tissue and osse- typical imaging findings [9, 10]. Untreated
ous injuries at the Chopart joint midtarsal sprains may cause instability and
complex involving the talocalca- chronic pain; therefore, recognition of mid-
neonavicular and calcaneocuboid joints. tarsal sprains by clinicians and radiologists
Typically, midtarsal sprains result from low- is important [9, 11].
energy, inversion-type ankle trauma. They In this article, we discuss Chopart joint
are distinct from Chopart joint fracture-dis- anatomy, pathomechanisms of midtarsal
locations, which result from high-energy sprains, clinical implications, and radio-
trauma such as motor vehicle crashes. graphic and cross-sectional imaging findings,
Midtarsal sprains may affect the support- with a focus on MRI. Other injuries affecting
ing ligaments along the talocalcaneonavic- the Chopart joint complex, such as fracture-
ular and calcaneocuboid joints. The most dislocation, will be briefly described.
commonly injured ligaments are the dor-
sal calcaneocuboid, bifurcate, and dorsal ta- Normal Anatomy and MRI of the
Keywords: ankle trauma, calcaneocuboid joint, lonavicular ligaments and the spring liga- Chopart Joint Complex
Chopart joint, midtarsal sprain, talonavicular ment complex, with plantar ligament injuries The Chopart joint complex, also known as
thought to be significantly less frequent [1–4]. the midtarsal or transverse tarsal joint, is lo-
doi.org/10.2214/AJR.17.19310
The range of osseous injuries includes contu- cated between the hindfoot and midfoot and
Received November 17, 2017; accepted after revision sions, avulsions, or impaction fractures of the consists of the talocalcaneonavicular and
January 11, 2018. anterior process of the calcaneus, talar head, calcaneocuboid joints. The joint complex is
cuboid bone, and navicular bone [2, 4, 5]. named after François Chopart, born in Par-
The true incidence of midtarsal sprains is in 1743, who is the surgeon credited with
1
Department of Radiology, Musculoskeletal Division,
NYU Langone Orthopedic Hospital, 301 E 17th St, 6th Fl,
New York, NY 10003. Address correspondence to
is uncertain, with disparate values reported describing and pioneering an anatomically
W. R. Walter (William.Walter@nyumc.org). in the literature ranging from 5.5% to 33% and functionally expedient method for treat-
of inversion ankle injuries [1, 6, 7], where- ing gangrene of the foot by disarticulation at
as midfoot fracture-dislocations are consid- the transverse tarsal joint. The first descrip-
2
Clinic of Radiology and Nuclear Medicine, University of
Basel Hospital, Basel, Switzerland.
erably less common, estimated to occur at tion of this operation was published in 1792,
3
Joint Department of Medical Imaging, University of a frequency of 3.6/100,000 per year [8]. In 3 years before his death [12].
Toronto, Toronto, ON, Canada. clinical and radiographic evaluations, mid-
tarsal sprains are frequently underdiagnosed Chopart Joint Function
AJR 2018; 211:1–10 and are missed at initial evaluation in up to The talocalcaneonavicular and calcaneo-
41% of cases, resulting in delayed treatment cuboid joints are regarded as a unit despite
0361–803X/18/2112–1
[1]. Recent estimates indicate that 22–40% the distinct functions provided by each. The
© American Roentgen Ray Society of midtarsal sprains are missed at presenta- talus and navicular form the proximal, flexi-
AJR:211, August 2018 1
Walter et al.
ble part of the medial column of the foot, and The spring ligament complex—The spring quences, and has variable signal intensity on
the calcaneus and cuboid form the proximal, (calcaneonavicular) ligament complex is T2-weighted sequences [20] (Fig. 2A).
more rigid segment of the lateral column. The composed of the superomedial, medioplan- The bifurcate ligament—The bifurcate lig-
Chopart joint complex allows the hindfoot to tar oblique, and inferoplantar longitudinal ament consists of the lateral calcaneonavic-
pivot while the forefoot remains still with in- components (Fig. 1). The superomedial com- ular and medial calcaneocuboid ligaments,
version and eversion. The complex locks on ponent is triangular or hammock-shaped, supporting the talonavicular and calcaneocu-
heel inversion, stabilizing the midfoot during coursing anteromedially from its origin at boid joints (Fig. 1). It is located anterior to the
the push-off phase of gait [13, 14]. the anteromedial aspect of the sustentaculum cervical ligament and the origin of the exten-
tali and attaching at the superomedial navic- sor digitorum brevis muscle. The lateral cal-
The Talocalcaneonavicular Joint ular tuberosity. Its inner surface is fibrocar- caneonavicular ligament extends between the
The talocalcaneonavicular joint, also known tilaginous, resembling an articular surface. intermediary tubercle of the calcaneus and the
as the talonavicular joint, is composed of the Loose connective tissue is interposed be- posterosuperior aspect of the lateral margin of
talar head, the posterior surface of the navic- tween the superomedial component and the the navicular (Figs. 1 and 2B). The medial
ular, and the anterior process of the calcane- posterior tibial tendon, allowing gliding be- calcaneocuboid ligament extends between the
us. Extracapsular ligaments of the sinus tarsi tween the two structures. The medioplantar intermediary tubercle, slightly lateral to the
and tarsal canal guide motion of the calcaneo- oblique component originates from the cor- lateral calcaneonavicular ligament, and the
navicular complex, a functional unit moving onoid fossa of the calcaneus, a notch in the dorsum of the cuboid, inserting approximate-
around the talus. Any motion between the cal- anterior process of the calcaneus. It courses ly 15 mm anterior to the calcaneocuboid joint
caneus and the talus occurs at the anterior and medially and obliquely, attaching at the me- [15] (Figs. 1 and 2C). The lateral calcaneona-
posterior subtalar joints [14, 15]. dioplantar navicular, just below its tuberos- vicular ligament was visualized in all speci-
Ligaments of the talonavicular joint can ity (Fig. 2A). The short and thick inferoplan- mens and imaging planes in a cadaveric study
be divided into ligaments of the acetabu- tar longitudinal component originates in the by Melão and colleagues [19], whereas the
lum pedis (spring ligament and calcaneona- coronoid fossa, anterolateral to the medio- medial calcaneocuboid ligament was less con-
vicular component of bifurcate ligament), ta- plantar oblique component, extends forward, sistently shown, best seen on coronal and sag-
localcaneal ligaments (lateral, medial, and and fans out onto the navicular beak [15, 16] ittal ankle MR images or short-axis and sag-
American Journal of Roentgenology
posterior talocalcaneal, interosseous, and (Fig. 2A). ittal foot MR images in another study [4]. On
cervical ligaments), and dorsal talonavicu- The superomedial component is best non–fat-saturated MRI sequences, the com-
lar ligament (Fig. 1). The talocalcaneal lig- shown on coronal and axial ankle MR im- ponents are thin, low- to intermediate-signal-
aments will not be discussed, because they ages and on short- and long-axis midfoot intensity structures highlighted by adjacent fat
pertain to the subtalar joint. MR images [17–19]. It is an intermedi- [19, 20] (Figs. 2B and 2C).
Ligaments of the acetabulum pedis—The ate- to low-signal-intensity band on T1- and Dorsal talonavicular ligament—The dor-
head of the talus articulates with the acetab- T2-weighted MRI sequences. The medio- sal talonavicular ligament is a capsular thick-
ulum pedis, which is formed by the navicu- plantar oblique component is best seen on ening connecting the dorsal aspect of the
lar anteriorly, the anterior and middle calca- axial ankle or long-axis midfoot planes and talar neck and the dorsal surface of the na-
neal facets and the plantar components of has a striated appearance (Fig. 2A). The me- vicular bone [15] (Fig. 1). It is hypointense
the spring ligament complex inferiorly, the dioplantar oblique component is usually not on T1- and T2-weighted MRI sequences and
superomedial component of the spring lig- seen on a single sagittal image because of is best visualized on sagittal MR images [19,
ament complex medially, and the calcaneo- its oblique course. The inferoplantar longi- 20] (Fig. 2D).
navicular component of the bifurcate liga- tudinal component is best seen on axial and
ment laterally (Fig. 1). The acetabulum pedis coronal ankle MR images and on long- and The Calcaneocuboid Joint
adapts to talar head displacement and rota- short-axis midfoot images, has intermediate The calcaneocuboid joint is formed by
tion [14]. to low signal intensity on T1-weighted se- the quadrilateral facets of the calcaneus and
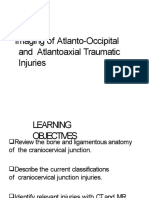
Fig. 1—Anatomy of Chopart joint complex.
A, Schematic drawing of supporting ligaments of Chopart joint
depicts dorsal talonavicular ligament (TN), bifurcate ligament
(calcaneonavicular and calcaneocuboid components), and
dorsal calcaneocuboid ligament (DCC; dorsal and lateral
bundles). Short and long plantar ligaments (not shown) stabilize
plantar aspect of joint.
B, Schematic drawing of spring ligament complex depicts
medioplantar oblique (MPO), inferoplantar longitudinal (IPL),
and superomedial (SM) components. (Reprinted from Magnetic
Resonance Imaging Clinics of North America, Vol. 25/edition
1, Tafur M, Rosenberg ZS, Bencardino JT. MR Imaging of the
Midfoot Including Chopart and Lisfranc Joint Complexes, Pages
95–125, Copyright 2017, with permission from Elsevier) [20].
A B
2 AJR:211, August 2018
Chopart Joint Complex
A B
American Journal of Roentgenology
C D E
Fig. 2—MRI anatomy of Chopart joint ligaments in different patients. Insets show level (lines) of each image.
A, Axial T1-weighted image of 37-year-old man/woman. Lateral band of dorsal calcaneocuboid ligament (arrowhead) is seen adjacent to extensor digitorum brevis muscle
(asterisk). Note also inferoplantar longitudinal (short arrow) and medioplantar oblique (long arrow) components of spring ligament complex.
B and C, T1-weighted images of 26-year-old man/woman show that lateral calcaneonavicular ligament (arrowhead, B) and more laterally located medial calcaneocuboid
ligament (wavy arrow, C) form bifurcate ligament. Long plantar ligament (curved arrow, C) typically has striated appearance.
D, Fat-saturated proton density–weighted image of 51-year-old man/woman. Talonavicular ligament (arrow) reinforces talonavicular joint capsule.
E, T1-weighted image of 44-year-old man/woman. Short plantar ligament (arrow) typically has striated appearance.
cuboid bone. The calcaneus articular sur- the medial calcaneocuboid component of the The plantar calcaneocuboid ligaments—
face is saddle-shaped, forming a groove di- bifurcate ligament, and the dorsal surface of The long and short plantar ligaments form
rected inferomedially. At its posteromedial the cuboid (Fig. 1). However, in a cadaveric the superficial and deep components of the
end is the calcaneal coronoid fossa, which study by Dorn-Lange and colleagues [21], al- inferior calcaneocuboid ligament, respec-
articulates with the beak of the cuboid. The most half of the cases showed morphologic tively. The long plantar ligament originates
posterior surface of the cuboid is also sad- variation including a V-shaped ligament, a from the inferior surface of the calcaneus
dle-shaped, with the cuboid beak lodging in meniscoid band, or two or more separate lig- between the posterior and anterior tubercles
the calcaneal coronoid fossa during forefoot aments (dorsal and lateral calcaneocuboid and divides distally into at least two bands
flexion and adduction [15]. Four ligaments ligaments). The normal dorsal calcaneocu- that attach to the cuboid (lateral band) and
connect the calcaneus and cuboid: the me- boid ligament is often difficult to identify on variably to the metatarsal bases (medial
dial calcaneocuboid ligament (component of sagittal images because of its small size and band). When present, the medial band forms
bifurcate, described in the previous section), volume-averaging effects with the overlying the roof of the peroneus longus tunnel [22].
the dorsal calcaneocuboid ligament, and the extensor digitorum brevis muscle. Melão and On MRI, the long plantar ligament has ho-
plantar calcaneocuboid ligaments (Fig. 1). colleagues [19] found dorsal calcaneocuboid mogeneous to striated low signal intensity
The dorsal calcaneocuboid ligament— ligaments in all specimens and that the dorsal and is well depicted on all ankle and midfoot
The dorsal calcaneocuboid ligament, also calcaneocuboid ligament was better shown planes [19] (Fig. 2C). The short plantar liga-
called the dorsolateral calcaneocuboid lig- on coronal ankle MR images or short-axis ment originates at the plantar surface of the
ament, has been described as a thin, broad midfoot MR images. The dorsal calcaneocu- calcaneus, anterior to the long plantar liga-
band between the superolateral aspect of the boid ligament is also well depicted on axial ment. It extends anteromedially to the plan-
anterior process of the calcaneus, lateral to MR images of the ankle [4, 20] (Fig. 2A). tar surface of the cuboid, proximal to the
AJR:211, August 2018 3
Walter et al.
TABLE 1: Mechanisms of Midtarsal Sprains
Mechanism
Characteristic Ankle Inversion Ankle Eversion
Primary injurious force Varus distraction at the lateral calcaneocuboid joint, impaction Valgus compression at the lateral calcaneocuboid joint,
at talonavicular joint, talonavicular plantar flexion distraction at talonavicular joint
Primary injury Lateral calcaneocuboid ligamentous or bony avulsion, dorsal Lateral calcaneocuboid contusion or impaction fracture (i.e.,
talonavicular ligamentous or bony avulsiona, impaction of nutcracker injuries)
plantar talar head and navicular body
Ligaments involved Dorsal calcaneocuboid and calcaneocuboid components of Short and long plantar ligaments
bifurcate ligament, dorsal talonavicular ligament
Secondary injuries Medial calcaneocuboid joint impaction, plantar ligament Plantar ligament avulsion, navicular tuberosity avulsion, talar
contusion or avulsion, plantar spring ligament avulsion head impaction
aWith superimposed plantar flexion during injury (e.g., wearing high-heeled shoes).
peroneus longus tunnel. The short plantar torum brevis origin avulsion. Impaction in- Although a less common injury mecha-
ligament appears striated and of intermedi- juries medially may produce contusions nism, ankle eversion can also result in mid-
ate signal intensity in all ankle and midfoot or fractures of the talar head and navicu- tarsal sprains (Fig. 3B). The distinguish-
planes on MRI [19, 20] (Fig. 2E). lar body. Occasionally, because of its com- ing feature of this injury is the compressive
plex saddle shape, the calcaneocuboid joint impaction (instead of distraction) force at the
Midtarsal Injuries: Pathomechanisms may suffer distraction forces laterally and lateral aspect of the calcaneocuboid joint,
Midtarsal sprains reflect a spectrum of in- impaction forces medially. Furthermore, dis- producing impaction fractures of the anteri-
juries resulting from low-energy trauma of traction forces across the Chopart joint com- or process of the calcaneus and posterolater-
the Chopart joint complex and encompass plex may cause avulsions of the plantar com- al cuboid, referred to as “nutcracker” injuries
both soft-tissue capsuloligamentous injuries ponents of the spring ligament. When ankle [23] (Fig. 3B). These impaction fractures are
American Journal of Roentgenology
and bony injuries, including ligament tears inversion is accompanied by plantar flex- often comminuted and depressed. Distrac-
or sprains as well as avulsion or impaction ion (as can occur while wearing high-heeled tion forces medially can cause navicular tu-
fractures, depending on the severity of the shoes), distraction forces propagate dorsally berosity avulsion fractures due to pull by the
trauma and the mechanism-dependent forc- through the talonavicular joint, often caus- posterior tibial tendon.
es involved. Although midtarsal sprains most ing dorsal talonavicular ligament avulsion.
commonly result from ankle inversion, ever- Distraction forces at the medial calcaneocu- High-Energy Midtarsal Injuries
sion injuries are also a possible mechanism. boid joint may also produce joint capsule and Other uncommon mechanisms of injury
Each mechanism results in a distinct inju- short plantar ligament avulsion injuries. known to cause Chopart joint complex inju-
ry pattern at the Chopart joint complex, and ries include direct longitudinal forces propa-
recognition of these patterns is critical for ra- Eversion Midtarsal Sprains gating along the metatarsal axes from a di-
diologists to propose a unified, accurate di-
agnosis of a midtarsal sprain (Table 1).
Inversion Midtarsal Sprains
Most midtarsal sprains are thought to oc-
cur as a result of an inversion injury (Fig.
3A), resulting in distraction forces across the
lateral and dorsolateral aspects of the cal-
caneocuboid joint [1, 2, 6] and, if the mag-
nitude of forces involved are sufficiently se-
vere, impaction along the medial column of
the foot. Distraction injuries often result in
avulsion fractures in combination with a tear
or sprain of the ligament stabilizing the joint.
Impaction injuries frequently cause contusion,
osteochondral injury, or impaction fractures
at the involved bony interfaces; occasionally, A B
ligamentous contusion can also accompany Fig. 3—Schematic drawings show typical inversion and eversion injury mechanisms of Chopart joint complex.
impaction injuries. (Drawings by Tafur M, used with permission)
Common injuries in this setting include A, Inversion, most common mechanism, will cause distraction forces and avulsions of calcaneocuboid
avulsion of the dorsal calcaneocuboid liga- ligaments and concomitant impaction forces at talonavicular joint. Commonly associated plantar flexion can
cause dorsal talonavicular ligament sprain. Arrow shows direction of forces.
ment and calcaneocuboid component of the B, Eversion of foot may lead to impaction injury of calcaneocuboid joint, which is also known as “nutcracker
bifurcate ligament as well as extensor digi- effect.” Arrow shows direction of forces.
4 AJR:211, August 2018
Chopart Joint Complex
panying talus and navicular fractures are of- is further confounded by the fact that most
ten comminuted and impacted and are also midtarsal sprains are accompanied by lateral
frequently underestimated on conventional collateral ligament sprains. Conversely, mid-
radiographs. Avascular necrosis and fracture tarsal sprains also occur in isolation; there-
nonunion are well-documented complica- fore, the diagnosis should not be discounted
tions, especially after delayed treatment. At in the presence of intact lateral collateral lig-
least 60% of the talonavicular articular sur- aments. One study found a negative correla-
face must be intact and congruent to prevent tion between findings associated with midtar-
a high risk of postsurgical instability [30]. sal sprain and syndesmotic ligament injury,
Calcaneocuboid fracture-dislocations are suggesting distinct injury mechanisms [3].
usually accompanied by comminuted calca- Nevertheless, the close proximity of the lat-
neus and cuboid impaction fractures. They eral collateral and midtarsal ligaments and
are commonly associated with medial col- the epidemiologic overlap between midtarsal
umn midfoot injuries, usually requiring sur- and lateral collateral ligament sprains, as well
gical treatment to restore Chopart joint con- as the high incidence of the latter, present a
gruence and correct the lengths of the medial challenge to clinicians evaluating acute inver-
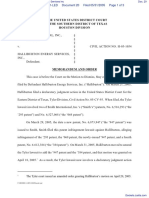
Fig. 4—Chopart fracture-dislocation in 27-year-old and lateral midfoot columns. Cuboid frac- sion-type ankle injuries.
woman after twisting ankle injury. Anteroposterior
radiograph of foot reveals talonavicular and, less tures rarely occur in isolation and are usual- Definitive clinical diagnosis of midtarsal
pronounced, calcaneocuboid malalignment with ly associated with low-energy trauma, rarely sprains often requires a high index of suspi-
small fracture fragment (arrow). requiring surgical intervention [29, 31]. cion [2, 34]. Pain, swelling, and point tender-
MRI is unnecessary and is rarely per- ness over the calcaneocuboid or talonavicu-
rect blow to the forefoot; when this occurs formed after high-energy trauma. Osseous lar joints are suggestive of a Chopart joint
with ankle plantar flexion, compressive forc- injury is more easily diagnosed using radi- injury. Varus stress applied at the lateral cal-
es at the navicular-cuneiform joints can re- ography or CT, and soft-tissue injuries are caneocuboid joint may show joint laxity, for
sult in a crush injury of the midtarsal joint unlikely to be addressed in the acute setting; which objective radiographic criteria have
American Journal of Roentgenology
(usually in high-energy scenarios) or shear- therefore, MRI is rightly deferred until the been developed. Varus stress radiographs of
ing forces, causing sagittally oriented navic- patient is clinically stabilized. the foot resulting in a calcaneocuboid angle
ular fractures [1, 10]. of greater than 10° are considered diagnos-
Subtalar Dislocations tic of a midtarsal sprain with instability [2].
Midtarsal Fracture-Dislocations Chopart joint injuries may also occur in Prolonged lateral foot pain after an acute
Midtarsal fracture-dislocations occur in the setting of subtalar dislocations. The lat- ankle injury, reflecting failure of conserva-
high-energy lower extremity trauma with ter are rare injuries, occurring almost exclu- tive management, may be the first sign of a
an axial loading force and are present in up sively in high-energy trauma related to mo- midtarsal sprain. The exact cause is contro-
to 10% of patients with motor vehicle crash tor vehicle crashes or axial loading caused versial, but Chopart joint instability specif-
polytrauma [24, 25]. This injury, although by falling from a height. Subtalar disloca- ically involving the calcaneocuboid joint is
obvious on imaging, may be initially over- tions universally involve the talocalcaneal thought to be the most likely cause. Cuboid
looked because of life-threatening trauma, joint, but most cases also result in talona- instability, or so-called “cuboid syndrome,”
resulting in a delayed diagnosis [26]. Frac- vicular dislocation, given that the stabilizing is an important cause of chronic lateral foot
ture-dislocations among low-energy traumas ligaments of the talonavicular joint are not pain and is at least in part related to posttrau-
are rare but have been reported in misstep in- as strong as those of the talocalcaneal joint. matic calcaneocuboid instability [11].
juries [27]. These injuries are usually clinically obvi- Most lateral ankle sprains are managed
Although Chopart joint dislocations are ous and are often accompanied by open frac- conservatively with a controlled–ankle mo-
commonly associated with fractures, isolat- tures. Concomitant fractures of the anterior tion walking boot or aircast splint, whereas
ed dislocations were found in 25% of cas- calcaneus and talus are common in these in- treatment of midtarsal sprains varies widely
es in one series [28]. Concomitant Lisfranc juries, and talar head avascular necrosis is a and remains controversial. Often, midtarsal
joint injuries occur in 20% of patients with common posttraumatic sequela [32, 33]. sprains are treated identically to lateral an-
Chopart fracture-dislocations; this combi- kle sprains; however, a recent report recom-
nation portends poorer outcomes compared Midtarsal Injuries mends more aggressive immobilization us-
with the outcomes of other Chopart fracture- Clinical Considerations ing a below-the-knee rigid cast for 6–8 weeks
dislocations [25, 28]. Because midtarsal sprains most common- followed by return to weight-bearing with a
Medial and dorsal direction of dislocation ly occur with inversion-type injuries, the pre- soft brace for 6 weeks [10]. The consequences
of the midfoot relative to the hindfoot is most sumptive clinical diagnosis often mistakenly of immobilization as a treatment of midtarsal
common (Fig. 4). Talonavicular dislocations favors the more common ankle sprain, in- sprains have not been systematically studied,
may be associated with subtalar or tibiotalar volving the lateral collateral ligaments—in but it is recognized that a subset of patients
dislocations. Fractures along the talonavic- particular, the talofibular and calcaneofibular will not improve with conservative manage-
ular joint shorten the medial column of the ligaments. Therefore, definitive diagnosis of ment [9, 36] and may require surgical inter-
midfoot, causing adduction malalignment midtarsal sprain is often delayed or is over- vention. Traditionally, midtarsal arthrode-
that requires surgical reduction [29]. Accom- looked entirely [34, 35]. Diagnostic accuracy sis is performed for chronic instability, pain,
AJR:211, August 2018 5
Walter et al.
and secondary Chopart osteoarthrosis [1, 10, based on radiographic evaluation has been is not usually indicated and is reserved only
26]. New operative techniques have been de- suggested in which the presence of a small for patients who, with or without known an-
veloped to address soft-tissue injuries with calcaneal or cuboid cortical avulsion fracture kle sprain, experience persistent severe pain
or without significant osseous injuries. Spe- fragment may be treated with casting for 6 or chronic ankle instability (symptoms of an-
cifically, primary reconstruction of the dorsal weeks but a large fracture fragment with a kle sprain typically resolve within 4 weeks)
calcaneocuboid ligament has been performed widened calcaneocuboid joint angle (> 10°) [39]. More extensive injuries, such as dis-
in patients, usually young athletes, with mid- requires open plate and screw fixation [2]. ruption of the tibiofibular syndesmosis, frac-
tarsal instability and refractory lateral foot tures, or osteochondral injuries, may be pres-
pain. Surgical techniques include perioste- Imaging Features With a Focus on MRI ent [40]. These patients are also the ones for
al flap, extensor digitorum brevis tendon, or Most acute ankle inversion injuries are whom radiologists should make an extra ef-
peroneal tendon graft reconstructions of the clinically diagnosed through a physical ex- fort to search for occult Chopart joint injury.
dorsolateral ligamentous complex of the cal- amination and careful history; occasionally, Radiography should be the initial imag-
caneocuboid joint [36–38]. radiographic evaluation is required to exclude ing modality for making the diagnosis of a
Nonreducible dislocations or displaced fractures or assess syndesmotic integrity. Chopart joint injury. Radiographic (or CT)
fractures are indications for operative man- Cross-sectional imaging, such as MRI or CT, evaluation is especially useful for detecting
agement [1, 9, 10]. A treatment algorithm for initial diagnosis or therapeutic decisions fractures about the Chopart joint that are fre-
American Journal of Roentgenology
A B C
Fig. 5—Inversion-related advanced Chopart joint complex injury with concomitant calcaneocuboid and talonavicular involvement in 55-year-old woman after twisting
right ankle injury.
A–C, Avulsion fractures of anterior calcaneal process at insertion of dorsal calcaneocuboid ligament (arrowheads, A and B) and of dorsum of talar head at insertion of
dorsal talonavicular ligament (arrow, C) can be seen on anteroposterior ankle (A), anteroposterior foot (B), and lateral ankle (C) radiographs. Note typical subfibular soft-
tissue swelling (asterisk, A) as secondary sign of calcaneocuboid joint injury.
A B C
Fig. 6—55-year-old woman who presented for follow-up imaging 3 weeks after falling.
A and B, Sagittal fat-saturated proton density–weighted MR images show dorsal talonavicular ligament avulsion (arrow, A) and nondisplaced fracture of anterior process
of calcaneus due to bifurcate ligament avulsion (arrow, B). Additional marrow edema may be related to capsular avulsion or plantar calcaneal contusion (arrowhead, B).
C, Axial fat-saturated proton density–weighted MR image shows mild edema at calcaneal and cuboid attachments of dorsal calcaneocuboid ligament (arrowheads).
Note edema of extensor digitorum brevis muscle (asterisk), common finding in Chopart joint complex injury.
6 AJR:211, August 2018
Chopart Joint Complex
quently associated with midtarsal sprains.
In the setting of ankle inversion, distraction
forces produce avulsion fractures along the
calcaneocuboid joint and impaction frac-
tures along the talonavicular joint (Fig. 5).
Concomitant plantar flexion may cause avul-
sion at the dorsal talonavicular joint (Fig.
5C). The reverse pattern will be seen in the
less-common ankle eversion injuries.
Radiographic evaluation for the detection
of subtle avulsion fractures requires scru-
tiny of each view depending on the frac-
ture location. Radiographic examinations of
both the ankle and foot will yield a higher
likelihood of fracture detection than either
examination separately. The lateral ankle or
foot views are optimal for detecting a dor-
sal talonavicular ligament avulsion fracture A
(Fig. 5). Because osteophytes are common
at this location, osseous irregularity may of-
ten be present; overlying soft-tissue swell-
ing is a helpful confirmatory sign of frac-
ture. An oblique view of the foot is optimal B
for visualizing the anterior process of the
calcaneus, although a displaced fracture of
American Journal of Roentgenology
the anterior process of the calcaneus may
also be detected on lateral views. Occasion-
ally, dorsolateral calcaneocuboid avulsion
fractures are seen on only the anteroposte-
rior radiograph of the ankle and are not vis-
ible on foot radiographs.
Avulsion fractures at ligamentous or cap-
sular attachments, in the setting of an inver-
sion injury, include dorsal calcaneocuboid
and bifurcate ligament avulsion fractures
from the anterior process of the calcaneus or
the dorsolateral cuboid [5, 41] and dorsal ta-
lonavicular ligament avulsion from either the
dorsal talar head or navicular (Figs. 5 and 6).
Another common avulsion fracture from the
dorsolateral anterior calcaneus occurs at the C D
origin of the extensor digitorum brevis mus-
Fig. 7—Inversion-related advanced Chopart joint complex injury with involvement of both talonavicular and
cle [42]. Occasionally, calcaneocuboid cap- calcaneocuboid joints in 77-year-old woman.
sular avulsion fractures occur at the lateral A, Fat-saturated proton density–weighted MR image reveals tear of talonavicular ligament (open arrow) and
or lateral-plantar calcaneus or cuboid (Fig. avulsion fracture at navicular attachment of inferoplantar longitudinal component of spring ligament (solid
5B). Avulsions of the plantar ligaments can arrow).
B–D, Fat-saturated proton density–weighted MR images show plantar talar head contusion (arrowhead, B)
occur medially. The least common avulsion and navicular tuberosity fracture (arrow, C). Laterally, there are avulsions at calcaneal attachment of dorsal
fractures are seen at the plantar navicular— calcaneocuboid ligament (arrowhead, C) and at cuboid attachment of calcaneocuboid part of bifurcate ligament
that is, at the attachment of the plantar com- (arrowhead, D).
ponents of the spring ligament (Fig. 7A). Fi-
nally, medial impaction fractures may occur es of the calcaneus and cuboid, and avulsion prompt a thorough search for others. For ex-
along the talonavicular joint, usually involv- fractures of the navicular tuberosity, due to ample, the presence of an avulsion fracture
ing the plantar aspect of the talar head and distraction forces and pull by the posterior of the anterior process of the calcaneus war-
sagittal plane navicular body fractures (Fig. tibial tendon, are associated with eversion in- rants careful inspection for the presence of
7). Osteochondral injuries at the talonavicu- juries (Fig. 8). the often subtle and overlooked dorsal talo-
lar articulation may also occur. Common fractures at the Chopart joint navicular fracture [5, 41, 43].
The typical nutcracker-type impaction often occur simultaneously; therefore, vi- CT is a sensitive, confirmatory examina-
fractures, occurring at the opposing surfac- sualization of any of these fractures should tion and may reveal fractures not otherwise
AJR:211, August 2018 7
Walter et al.
Because midtarsal sprains are predom-
inantly ligamentous injuries, the superior
soft-tissue contrast of MRI is optimal for es-
tablishing a comprehensive, accurate diagno-
sis of Chopart joint injury. Based on MRI,
most cases of midtarsal sprains involve mul-
tiple ligaments—most commonly, the dor-
sal calcaneocuboid and bifurcate ligaments
(Figs. 6 and 7). Similar to the MRI appear-
ance of ankle ligament sprains, the MRI ap-
pearance of acute or subacute injuries will
be ligamentous edema, discontinuity, irregu-
larity, waviness, and laxity [47]. Focal mar-
row edema at the osseous attachments of the
ligaments typically indicates underlying lig-
A B amentous injury. The evolution of midtarsal
Fig. 8—Eversion-related nutcracker-type fracture pattern in 51-year-old woman. ligamentous sprain is thought to resemble
A, Anteroposterior radiograph of foot reveals impaction fracture of anterior calcaneal process (arrow) and ligaments in other locations with eventual
nondisplaced avulsion fracture of navicular tuberosity (arrowhead).
B, Fat-saturated proton density–weighted MR image shows impaction fracture of proximal cuboid (wavy black scar-remodeling causing low-signal-intensity
arrow) in addition to calcaneal fracture (straight black arrow) and extensive bone marrow edema of distal thickening. Old injury is a common cause of
calcaneus (white arrow). increased ligament conspicuity (Fig. 10).
Careful inspection of the lesser-known
detected on radiography, so the Chopart joint medial calcaneocuboid joint, and dorsolater- ligaments stabilizing the Chopart joint (such
should again be scrutinized (Fig. 9). Over- al calcaneus and cuboid (Figs. 6 and 7). Nut- as the dorsal calcaneocuboid ligament) is
all, radiographic detection of midtarsal inju- cracker injuries associated with ankle ever- particularly important when seeking mid-
American Journal of Roentgenology
ries is thought to be insensitive, missing up sion may be radiographically subtle but are tarsal sprains. Because the normal dorsal
to 33% of cases with fractures [44]. Again, readily seen on MRI with bone marrow ede- calcaneocuboid and calcaneocuboid com-
when a single midtarsal avulsion fracture is ma in the anterior process of the calcaneus ponents of the bifurcate ligament may be
identified, others should be carefully sought and throughout the cuboid (Fig. 8). In contra- difficult to detect on MRI, failure to visual-
and the potential diagnosis of midtarsal distinction to impaction fractures that cause ize them should not automatically be con-
sprain should be invoked. Even in the ab- obvious bone marrow edema, the marrow sidered pathologic; secondary signs of liga-
sence of additional fractures, associated liga- edema caused by ligamentous avulsion with mentous injury should be sought to support
mentous injuries indicating midtarsal sprain or without a fracture fragment is surprisingly the diagnosis of a sprain. For example, mar-
are common and MRI is a useful modality minimal and, therefore, small foci of marrow row edema within the anterior process of the
for their detection [5]. edema on MRI should be carefully assessed calcaneus or dorsolateral cuboid or periliga-
MRI is superior to conventional radiog- in correlation with radiographs or CT images mentous fat edema should heighten suspicion
raphy in the detection of soft-tissue inju- for a potential avulsion injury [45, 46]. of acute injury. Ligament discontinuity or ir-
ries and, sometimes, osseous injuries at the
Chopart joint. In one recent study, calcaneo-
cuboid avulsion fractures were evident in
48% of radiographs and 100% of MR imag-
es [5]. Similarly, talonavicular joint injuries
were evident in 38% of radiographs and 76%
of MR images [5]. Furthermore, simultane-
ous involvement of both the calcaneocuboid
and talonavicular joints, based on the pres-
ence of marrow edema, fractures, or liga-
mentous injury, was noted in 76% of MRI
examinations compared with 14% of radio-
graphs [5] (Figs. 6 and 7).
The Chopart joint complex is readily eval-
uated on ankle MRI; thus, a dedicated mid-
tarsal protocol is not mandatory. MRI is
sensitive for detecting typical contusions or
nondisplaced impaction fractures. Common A B
and consistent patterns of marrow edema in
Fig. 9—CT images depict inversion-related Chopart joint complex injury in 39-year-old woman.
midtarsal sprains include the dorsal or plan- A and B, Sagittal reformatted images show talonavicular avulsion fractures at dorsum of talar head (open
tar talar head, anterior calcaneal process, arrow, A) and navicular (solid arrow, A) and avulsion fracture of anterior calcaneal process (arrow, B).
8 AJR:211, August 2018
Chopart Joint Complex
porting ligaments on sagittal fluid-sensitive (Chopart) sprain in the setting of acute ankle in-
images may create the false impression of jury. AJR 2018; 210:386–395
ligament signal hyperintensity and be easi- 5. Hirschmann A, Walter WR, Alaia EF, Garwood
ly mistaken for a sprain. Additionally, a spu- ER, Rosenberg ZS. Acute fracture of the anterior
rious appearance of “ligament thickening” process of calcaneus: does it herald a more ad-
may be seen on MR images obtained with fat vanced injury to Chopart joint? AJR 2018;
saturation because of volume averaging be- 210:1123–1130
tween the ligament and saturated signal from 6. Søndergaard L, Konradsen L, Hølmer P, Jørgensen
adjacent fat. Correlation with T1-weighted LN, Nielsen PT. Acute midtarsal sprains: frequen-
sagittal images clarifies these issues. cy and course of recovery. Foot Ankle Int 1996;
Ultrasound evaluation of the midtar- 17:195–199
sal ligaments is of great utility in experi- 7. Broström L. Sprained ankles. Part 3. Clinical ob-
enced hands. Sonographic evaluation of the servations in recent ligament ruptures. Acta Chir
Chopart joint allows dynamic assessment of Scand 1965; 130:560–569
joint stability and is particularly suited for 8. Court-Brown CM, Caesar B. Epidemiology of
evaluating the superficial dorsal and later- adult fractures: a review. Injury 2006; 37:691–697
Fig. 10—Old Chopart joint injury with osteoarthritis al soft tissues about the joint, including the 9. van Dorp KB, de Vries MR, van der Elst M,
of calcaneocuboid joint in 67-year-old woman.
Deformity and nonunion of avulsion fracture dorsal calcaneocuboid, dorsal talonavicular, Schepers T. Chopart joint injury: a study of out-
of anterior calcaneal process (arrowhead) and and calcaneocuboid joint capsules [49]. It come and morbidity. J Foot Ankle Surg 2010;
subchondral degenerative changes at opposing has also been shown to depict some avulsion 49:541–545
cuboid (arrow) are seen on this sagittal fat-saturated
T2-weighted MR image.
fractures associated with midtarsal sprains 10. Kutaish H, Stern R, Drittenbass L, Assal M. Inju-
[34, 50]. Although MRI evaluation is re- ries to the Chopart joint complex: a current review.
quired to exclude midtarsal sprain in the set- Eur J Orthop Surg Traumatol 2017; 27:425–431
regularity and overlying edema are concrete ting of normal or equivocal ultrasound find- 11. Durall CJ. Examination and treatment of cuboid
signs of ligamentous injury [4]. ings and is more sensitive for nondisplaced syndrome: a literature review. Sports Health 2011;
American Journal of Roentgenology
The dorsal talonavicular ligament, a cap- fractures, ultrasound offers an attractive mo- 3:514–519
sular thickening, traverses the talonavicu- dality for point-of-care evaluation. 12. Wolf JH. François Chopart (1743–1795): inventor
lar joint dorsally but also extends quite far of the partial foot amputation at the tarsometatar-
medially and laterally [19]. Therefore, par- Conclusion sal articulation. Operat Orthop Traumatol 2003;
tial tears may occur. In our experience, ede- Chopart joint complex injuries—specifi- 4:314–317
ma associated with dorsal talonavicular lig- cally, midtarsal sprains—are relatively com- 13. Benirschke SK, Meinberg E, Anderson SA, Jones
amentous avulsion is most commonly seen mon in the setting of inversion-type ankle CB, Cole PA. Fractures and dislocations of the
in the dorsal talar head (Fig. 6A) and is less injuries and typically present as avulsion in- midfoot: Lisfranc and Chopart injuries. J Bone
commonly seen in the dorsal navicular. juries across the calcaneocuboid joint and Joint Surg Am 2012; 4:1325–1337
Several pitfalls should be considered when impaction injuries at the talonavicular joint. 14. Sarrafian SK. Biomechanics of the subtalar joint
evaluating the ligaments at the Chopart joint. Conversely, an eversion mechanism will complex. Clin Orthop Relat Res 1993; 290:17–26
The aforementioned anatomic variations cause impaction injuries at the calcaneo- 15. Kelikian AS, ed. Sarrafian’s anatomy of the foot
(predominantly involving the dorsal calca- cuboid joint and medial avulsion fractures, and ankle: descriptive, topographic, functional,
neocuboid ligament) may produce distinct typically at the navicular tuberosity. Under- 3rd ed. Philadelphia, PA: Lippincott Williams &
MRI appearances. For example, a thick lat- standing midtarsal joint anatomy, the mech- Wilkins, 2011
eral band of the dorsal calcaneocuboid lig- anisms of injury, and the implications for 16. Taniguchi A, Tanaka Y, Takakura Y, Kadono K,
ament will be conspicuous on axial images. management is important for radiologists so Maeda M, Yamamoto H. Anatomy of the spring
Alternatively, the meniscoid variant pro- that they are able to provide a timely diagno- ligament. J Bone Joint Surg Am 2003; 85:2174–2178
trudes into the calcaneocuboid joint [21, 48]. sis and help optimize management of these 17. Mengiardi B, Zanetti M, Schottle PB, et al. Spring
The dorsal talonavicular ligament is well frequently overlooked injuries. ligament complex: MR imaging-anatomic corre-
evaluated on sagittal images but may appear lation and findings in asymptomatic subjects.
thickened relative to the other midtarsal liga- References Radiology 2005; 237:242–249
ments; care should be taken, particularly in 1. Main BJ, Jowett RL. Injuries of the midtarsal 18. Yao L, Gentili A, Cracchiolo A. MR imaging find-
the absence of associated soft-tissue or mar- joint. J Bone Joint Surg Br 1975; 57:89–97 ings in spring ligament insufficiency. Skeletal
row edema, to avoid overdiagnosing thicken- 2. Andermahr J, Helling HJ, Maintz D, Monig S, Radiol 1999; 28:245–250
ing as evidence of an old midtarsal sprain. Koebke J, Rehm KE. The injury of the calcaneocu- 19. Melão L, Canella C, Weber M, Negrão P, Trudell
The talonavicular joint is highly mobile and boid ligaments. Foot Ankle Int 2000; 21:379–384 D, Resnick D. Ligaments of the transverse tarsal
therefore is susceptible to increased stress 3. Gorbachova T, Wang PS, Hu B, Horrow JC. Plantar joint complex: MRI-anatomic correlation in ca-
and motion during daily activities, likely ac- talar head contusions and osteochondral fractures: as- davers. AJR 2009; 193:662–671
counting for traction-related scarring. sociated findings on ankle MRI and proposed mecha- 20. Tafur M, Rosenberg ZS, Bencardino JT. MR im-
Another potential pitfall occurs in the nism of injury. Skeletal Radiol 2016; 45:795–803 aging of the midfoot including Chopart and
presence of a midtarsal joint effusion. Vol- 4. Walter WR, Hirschmann A, Alaia EF, Garwood Lisfranc joint complexes. Magn Reson Imaging
ume averaging of joint fluid with the sup- ER, Rosenberg ZS. MRI evaluation of midtarsal Clin N Am 2017; 25:95–125
AJR:211, August 2018 9
Walter et al.
21. Dorn-Lange NV, Nauck T, Lohrer H, Arentz S, of the os calcis. South Med J 1958; 51:1161–1164 2007; 36:627–632
Konerding MA. Morphology of the dorsal and lat- 32. Saltzman C, Marsh JL. Hindfoot dislocations: 42. Norfray JF, Rogers LF, Adamo GP, Groves HC,
eral calcaneocuboid ligaments. Foot Ankle Int when are they not benign? J Am Acad Orthop Heiser WJ. Common calcaneal avulsion fracture.
2008; 29:942–949 Surg 1997; 5:192–198 AJR 1980; 134:119–123
22. Ward KA, Soames RW. Morphology of the plan- 33. Veltman ES, Steller EJ, Wittich P, Keizer J. Lat- 43. Schmitt JW, Werner CM, Ossendorf C, Wanner
tar calcaneocuboid ligaments. Foot Ankle Int eral subtalar dislocation: case report and review of GA, Simmen HP. Avulsion fracture of the dorsal
1997; 18:649–653 the literature. World J Orthop 2016; 7:623–627 talonavicular ligament: a subtle radiographic sign
23. Hermel MB, Gershon-Cohen J. The nutcracker 34. Lee SW, Kim DD, Buskanets A, Oh-Park M. Mid- of possible Chopart joint dislocation. Foot Ankle
fracture of the cuboid by indirect violence. tarsal sprain misdiagnosed as ankle sprain: role of Int 2011; 32:722–726
Radiology 1953; 60:850–854 ultrasonography in diagnosis. Am J Phys Med 44. Haapamaki VV, Kiuru MJ, Koskinen SK. Ankle
24. Wilson LS Jr, Mizel MS, Michelson JD. Foot and Rehabil 2016; 95:e44–e45 and foot injuries: analysis of MDCT findings. AJR
ankle injuries in motor vehicle accidents. Foot 35. Zwipp H, Rammelt S, Grass R. Ligamentous inju- 2004; 183:615–622
Ankle Int 2001; 22:649–652 ries about the ankle and subtalar joints. Clin 45. Weishaupt D, Schweitzer ME. MR imaging of the
25. Richter M, Wippermann B, Krettek C, Schratt HE, Podiatr Med Surg 2002; 19:195–229 foot and ankle: patterns of bone marrow signal
Hufner T, Therman H. Fractures and fracture dislo- 36. Lohrer H, Nauck T. Augmented periosteal flap re- abnormalities. Eur Radiol 2002; 12:416–426
cations of the midfoot: occurrence, causes and long- pair of the chronically unstable calcaneocuboid 46. Rios AM, Rosenberg ZS, Bencardino JT, Rodrigo
term results. Foot Ankle Int 2001; 22:392–398 joint: a series of six cases. J Bone Joint Surg Am SP, Theran SG. Bone marrow edema patterns in
26. Rammelt S, Schepers T. Chopart injuries: when to 2006; 88:1596–1601 the ankle and hindfoot: distinguishing MRI fea-
fix and when to fuse? Foot Ankle Clin 2017; 37. Lohrer H, Nauck T, Arentz S, Vogl TJ. Dorsal cal- tures. AJR 2011; 197:[web]W720–W729
22:163–180 caneocuboid ligament versus lateral ankle liga- 47. Rosenberg ZS, Beltran J, Bencardino JT. From the
27. Harris AP, Johnson J, Waryasz GR. Isolated dor- ment repair: a case-control study. Br J Sports Med RSNA refresher courses, Radiological Society of
sal dislocations of the talonavicular and calcaneo- 2006; 40:839–843 North America: MR imaging of the ankle and foot.
cuboid articulations (Chopart joints) from a low- 38. Hirschmann MT, Friederich NF, Muller C. Ana- RadioGraphics 2000; 20(20 spec no.):S153–S179
energy mechanism. Am J Emerg Med 2016; tomic reconstruction of a chronically unstable 48. Hollander JD, Lidtke RH, Lai JY. The labrum of
34:1733.e1–1733.e4 calcaneocuboid joint with augmented extensor the calcaneocuboid joint. J Foot Ankle Surg 1998;
American Journal of Roentgenology
28. Richter M, Thermann H, Huefner T, Schmidt U, digitorum brevis muscle flap: a new method. Foot 37:308–312
Goesling T, Krettek C. Chopart joint fracture- Ankle Int 2008; 29:1258–1261 49. Sconfienza LM, Orlandi D, Lacelli F, Serafini G,
dislocation: initial open reduction provides better 39. Renstrom PA. Persistently painful sprained an- Silvestri E. Dynamic high-resolution US of ankle
outcome than closed reduction. Foot Ankle Int kle. J Am Acad Orthop Surg 1994; 2:270–280 and midfoot ligaments: normal anatomic struc-
2004; 25:340–348 40. Polzer H, Kanz KG, Prall WC, et al. Diagnosis and ture and imaging technique. RadioGraphics 2015;
29. Swords MP, Schramski M, Switzer K, Nemec S. treatment of acute ankle injuries: development of 35:164–178
Chopart fractures and dislocations. Foot Ankle an evidence-based algorithm. Orthop Rev (Pavia) 50. Thiounn A, Szymanski C, Lalanne C, Soudy K,
Clin 2008; 13:679–693 2012; 4:e5 Demondion X, Maynou C. Prospective observa-
30. Pinney SJ, Sangeorzan BJ. Fractures of the tarsal 41. Petrover D, Schweitzer ME, Laredo JD. Anterior tional study of midtarsal joint sprain: epidemio-
bones. Orthop Clin North Am 2001; 32:21–33 process calcaneal fractures: a systematic evalua- logical and ultrasonographic analysis. Orthop
31. Dell JM Jr. Fractures of the anterior superior process tion of associated conditions. Skeletal Radiol Traumatol Surg Res 2016; 102:657–661
10 AJR:211, August 2018
You might also like
- The Third RomeDocument52 pagesThe Third Romejoedoedoedoe100% (1)
- Boost Your Brain PowerDocument2 pagesBoost Your Brain PowerStrafalogea SerbanNo ratings yet
- SaaS - Primer (VF) PDFDocument20 pagesSaaS - Primer (VF) PDFfiend114100% (2)
- Domain 1 Teacher Self-ReflectionDocument3 pagesDomain 1 Teacher Self-ReflectionleezenarosaNo ratings yet
- Anterior Decompression Techniques For Thoracic and Lumbar FracturesDocument10 pagesAnterior Decompression Techniques For Thoracic and Lumbar Fracturesmetasoniko81No ratings yet
- The Knee - Breaking The MR ReflexDocument20 pagesThe Knee - Breaking The MR ReflexManiDeep ReddyNo ratings yet
- TraumaDocument51 pagesTraumaKumail KhandwalaNo ratings yet
- Surgery Management of Fractures, Dislocations, and Traumatic Instability of The ElbowDocument17 pagesSurgery Management of Fractures, Dislocations, and Traumatic Instability of The ElbowErvaldi IlhamNo ratings yet
- Scapular Fractures: What Radiologists Need To Know: Alan M. Ropp Derik L. DavisDocument11 pagesScapular Fractures: What Radiologists Need To Know: Alan M. Ropp Derik L. DavisMuhammad AliNo ratings yet
- Temporal Bone TraumaDocument16 pagesTemporal Bone Traumadafita4661No ratings yet
- Embryologi CraniocervicalDocument19 pagesEmbryologi CraniocervicalelizabethmargarethNo ratings yet
- Management of Fractures of The Proximal UlnaDocument12 pagesManagement of Fractures of The Proximal UlnaDiana Marcela Benítez HernándezNo ratings yet
- Simon Hill 1989 Rotator Cuff Injuries An UpdateDocument5 pagesSimon Hill 1989 Rotator Cuff Injuries An Updatearaujoaoh07No ratings yet
- Comminuted Patella FracturesDocument8 pagesComminuted Patella FracturesKirana lupitaNo ratings yet
- Fracturas PatologicasDocument20 pagesFracturas PatologicasSamantha AriasNo ratings yet
- Missed Monteggia FXDocument16 pagesMissed Monteggia FXEric RothNo ratings yet
- RG 2020190085Document18 pagesRG 2020190085zoom radiologiNo ratings yet
- 2015 Article 75Document9 pages2015 Article 75Finna Tryasti Fidianti1BNo ratings yet
- Triangular Fibrocartilage Complex Lesions - A Classification (Palmer Classification)Document13 pagesTriangular Fibrocartilage Complex Lesions - A Classification (Palmer Classification)alobrienNo ratings yet
- Tratamiento Quirurgico de Triada Terrible de CodoDocument9 pagesTratamiento Quirurgico de Triada Terrible de Codotraumatologia ortopediaNo ratings yet
- Hombro Inlges PDFDocument6 pagesHombro Inlges PDFOscar Segun DoNo ratings yet
- Fractura Cadera 1Document22 pagesFractura Cadera 1Júlia LedesmaNo ratings yet
- Mri Snowboarding InjuryDocument6 pagesMri Snowboarding InjuryJaume SanahujaNo ratings yet
- Management of Thumb Metacarpophalangeal Hyperextension in The Setting of Thumb Basal Joint ArthritisDocument8 pagesManagement of Thumb Metacarpophalangeal Hyperextension in The Setting of Thumb Basal Joint ArthritiscesarmgaytanmedinaNo ratings yet
- Spinal Cord InjuryDocument4 pagesSpinal Cord Injuryvandrade_635870No ratings yet
- 10.1097@00124635 200007000 00007Document10 pages10.1097@00124635 200007000 00007HOSPITAL COMUNEROS ORTOPEDIANo ratings yet
- Mid Shaft Femur FXDocument10 pagesMid Shaft Femur FXDoctor's BettaNo ratings yet
- J Langford. Pelvic Fractures Part 1, Evaluation, Calssification and Resucitation. 2013Document10 pagesJ Langford. Pelvic Fractures Part 1, Evaluation, Calssification and Resucitation. 2013Bruno HazlebyNo ratings yet
- Imaging of Blunt Thoracic TraumaDocument24 pagesImaging of Blunt Thoracic TraumaZai RojasNo ratings yet
- Kuliah Dr. MLDocument206 pagesKuliah Dr. MLBakingpancakesNo ratings yet
- Wrist Anatomy and Biomechanics: American Society For Surgery of The Hand.)Document9 pagesWrist Anatomy and Biomechanics: American Society For Surgery of The Hand.)Roberto Alonso Lopez SantanaNo ratings yet
- Current Concepts Tibial Plateau FXDocument14 pagesCurrent Concepts Tibial Plateau FXOrtho 20172100% (1)
- Imaging of Atlanto-Occipital and Atlantoaxial Traumatic InjuriesDocument43 pagesImaging of Atlanto-Occipital and Atlantoaxial Traumatic InjuriesMaroofAliNo ratings yet
- Anatomico-Surgical Review of Krikatika Marma Surgical Review of Krikatika MarmaDocument6 pagesAnatomico-Surgical Review of Krikatika Marma Surgical Review of Krikatika MarmaJoseph L. WalkerNo ratings yet
- Current Concepts in Elbow Fracture Dislocation: Adam C Watts, Jagwant Singh, Michael Elvey and Zaid HamoodiDocument8 pagesCurrent Concepts in Elbow Fracture Dislocation: Adam C Watts, Jagwant Singh, Michael Elvey and Zaid HamoodiJoão Artur BonadimanNo ratings yet
- Exogenous Spinal Trauma-Surgical Therapy and AftercareDocument8 pagesExogenous Spinal Trauma-Surgical Therapy and Aftercaretaner_soysurenNo ratings yet
- Exposure Coronoid FXDocument9 pagesExposure Coronoid FXGiulio PriftiNo ratings yet
- Imaging of Spine Trauma: Neuroradiology Review Series Neuroradiology Review SeriesDocument17 pagesImaging of Spine Trauma: Neuroradiology Review Series Neuroradiology Review SeriesSalman Alfarisy GaulNo ratings yet
- A Clinical Approach To Diagnosing Wrist Pain: Los Angeles, CaliforniaDocument6 pagesA Clinical Approach To Diagnosing Wrist Pain: Los Angeles, CaliforniaOtnil DNo ratings yet
- A Functional Approach To The Treatment of TFCC Problems KroonDocument16 pagesA Functional Approach To The Treatment of TFCC Problems KroonLaineyNo ratings yet
- 2709 1 23473 1 10 20211231 - Compressed - CompressedDocument13 pages2709 1 23473 1 10 20211231 - Compressed - CompressedmedicNo ratings yet
- Clinical Approaches For Shoulder Injuries in SportsDocument5 pagesClinical Approaches For Shoulder Injuries in SportsanasbugaenkoNo ratings yet
- Complex Elbow InstabilityDocument9 pagesComplex Elbow InstabilityAristoteles Plato SocratesNo ratings yet
- Acute Capsulolig Sports Injuries - AnkleDocument19 pagesAcute Capsulolig Sports Injuries - AnkleIgor Bruno BritoNo ratings yet
- Chopart RSNADocument35 pagesChopart RSNASalvatore CappelliNo ratings yet
- Musculo TemporalDocument6 pagesMusculo TemporalNaim CalilNo ratings yet
- 2012 Fai Sub Talar InstabilityDocument10 pages2012 Fai Sub Talar Instabilityvijaypatel4282No ratings yet
- Initial Management of Acute Spinal Cord Injury: Stephen Bonner MRCP FRCA FFICM Caroline Smith FRCADocument8 pagesInitial Management of Acute Spinal Cord Injury: Stephen Bonner MRCP FRCA FFICM Caroline Smith FRCAMinaz PatelNo ratings yet
- Kassarjian 2012Document9 pagesKassarjian 2012micamart.94No ratings yet
- Spine Trauma and Management - Rocker and DoucetteDocument63 pagesSpine Trauma and Management - Rocker and DoucetteAlex EniuNo ratings yet
- Fractures of Distal Radius: An Overview: Family PracticeDocument8 pagesFractures of Distal Radius: An Overview: Family Practicesuci triana putriNo ratings yet
- Subtrochanteric Femur Fractures: Current Review of ManagementDocument7 pagesSubtrochanteric Femur Fractures: Current Review of ManagementErmiNo ratings yet
- Kramer 2014 TODocument7 pagesKramer 2014 TOjuanNo ratings yet
- Tibial Plateau Fractures: A Review: P Fenton and K PorterDocument7 pagesTibial Plateau Fractures: A Review: P Fenton and K PorterDot DitNo ratings yet
- 2016 Article 9341 PDFDocument8 pages2016 Article 9341 PDFJulenda CintarinovaNo ratings yet
- FractureDocument16 pagesFractureGenevieve LawrenceNo ratings yet
- Tomsan Et Al 2023 Knee Mri Meniscus Roots Ramps Repairs and RepercussionsDocument17 pagesTomsan Et Al 2023 Knee Mri Meniscus Roots Ramps Repairs and RepercussionsgvstbndyhkNo ratings yet
- Clasificacion FX AtlasDocument8 pagesClasificacion FX AtlastedejoNo ratings yet
- Imágenes de RM de Trauma MuscularDocument23 pagesImágenes de RM de Trauma Muscularmicamart.94No ratings yet
- Lumbar Spinal StenosisDocument13 pagesLumbar Spinal Stenosis7w7dzjhgbqNo ratings yet
- Background International Classification of Function (ICF)Document1 pageBackground International Classification of Function (ICF)api-544990754No ratings yet
- Covey JBJS PCL InjuriesDocument11 pagesCovey JBJS PCL InjuriesGirish HNo ratings yet
- Athletic Injuries of The ThoracicDocument20 pagesAthletic Injuries of The ThoracicGrado CristianNo ratings yet
- The Sutures of the Skull: Anatomy, Embryology, Imaging, and SurgeryFrom EverandThe Sutures of the Skull: Anatomy, Embryology, Imaging, and SurgeryNo ratings yet
- Product Life Cycle ManagementDocument57 pagesProduct Life Cycle ManagementSudarshan MankadNo ratings yet
- Relics of Pagan Antiquity in Mediæval SettingsDocument22 pagesRelics of Pagan Antiquity in Mediæval SettingsZhennya SlootskinNo ratings yet
- 3.6.b Relational Databases and NormalisationDocument10 pages3.6.b Relational Databases and Normalisationne002No ratings yet
- Heart Copy of Demonstration-Teaching-Rating-Sheet-ICTDocument3 pagesHeart Copy of Demonstration-Teaching-Rating-Sheet-ICTLouann Heart Lupo100% (1)
- Ahavas TorahDocument24 pagesAhavas TorahJose MartinezNo ratings yet
- Referat Mata KeratititsDocument28 pagesReferat Mata Keratititswidya melianitaNo ratings yet
- Grade 9: Research Quiz: Citation FormatsDocument20 pagesGrade 9: Research Quiz: Citation Formatsvia macario100% (1)
- OralComm Q2 W6 GLAKDocument20 pagesOralComm Q2 W6 GLAKCherryl GallegoNo ratings yet
- 191HS42 - Probability & Statistics - Question Bank PDFDocument7 pages191HS42 - Probability & Statistics - Question Bank PDFKaleesNo ratings yet
- Revision Units 4-6 Going For GoldDocument2 pagesRevision Units 4-6 Going For GoldZsuzsa StuparNo ratings yet
- Lesson PlanDocument3 pagesLesson Planapi-530241350No ratings yet
- Particle Physics (Physics Factsheet)Document27 pagesParticle Physics (Physics Factsheet)Utsav Dhakal83% (6)
- PerDev Learning ActivityDocument4 pagesPerDev Learning ActivitydwacindyfjNo ratings yet
- Chapter Quiz 1. MCNDocument4 pagesChapter Quiz 1. MCNAngie SaquingNo ratings yet
- Error Code Analysis Flow (Mechanism) : 10300 IP Sensor Logical InconsistencyDocument1 pageError Code Analysis Flow (Mechanism) : 10300 IP Sensor Logical InconsistencyElvira RodNo ratings yet
- Secrets. - in Addition To The Proper Administrative Action, TheDocument10 pagesSecrets. - in Addition To The Proper Administrative Action, TheDino AbieraNo ratings yet
- Conjunctions: Coordinating Conjunctions Subordinating ConjunctionsDocument4 pagesConjunctions: Coordinating Conjunctions Subordinating ConjunctionsRokiah ShukerNo ratings yet
- Thesis On Impact of Job Stress On Employee PerformanceDocument7 pagesThesis On Impact of Job Stress On Employee PerformancecoawokuggNo ratings yet
- Chapter 12 - Perfect CompetitionDocument12 pagesChapter 12 - Perfect CompetitionMmxSellerNo ratings yet
- Q2 - Lesson 1 - Worksheet 3 - Card CatalogDocument3 pagesQ2 - Lesson 1 - Worksheet 3 - Card CatalogTine DayotNo ratings yet
- EDU Development of Malaysian EducationDocument47 pagesEDU Development of Malaysian EducationNabilFikriChumiNo ratings yet
- Periodic Safety Update Reports: Adel Alrwisan B.SC, M.SC, PPCDocument16 pagesPeriodic Safety Update Reports: Adel Alrwisan B.SC, M.SC, PPCHala MohamedNo ratings yet
- Smith International Inc v. Halliburton Energy Services Inc - Document No. 20Document3 pagesSmith International Inc v. Halliburton Energy Services Inc - Document No. 20Justia.comNo ratings yet
- Define Applied EconomicsDocument18 pagesDefine Applied EconomicsThalia Rhine AberteNo ratings yet
- Process Control, Network Systems, and SCADADocument13 pagesProcess Control, Network Systems, and SCADASTNo ratings yet
- Absolute Advantage TheoryDocument13 pagesAbsolute Advantage TheoryrajkumarkvNo ratings yet