Download as pdf or txt
You might also like
- Common JCI CBAHI Survey QuestionsDocument371 pagesCommon JCI CBAHI Survey Questionsshadi alshadafan100% (4)
- Case Preterm Labor Ch.Document29 pagesCase Preterm Labor Ch.Gazala Parveen100% (1)
- Pahtophysiology of EsrdDocument5 pagesPahtophysiology of EsrdCarl JardelezaNo ratings yet
- Placental Growth Factor and Pre-Eclampsia: ReviewDocument5 pagesPlacental Growth Factor and Pre-Eclampsia: ReviewAnnissa SyairaNo ratings yet
- Mechanisms and Potential Therapies For PreeclampsiaDocument8 pagesMechanisms and Potential Therapies For PreeclampsiaAchmad Deza FaristaNo ratings yet
- 17189.1 20150302091114 CoveredDocument11 pages17189.1 20150302091114 CoveredLintang SuroyaNo ratings yet
- Angiogenic Factors in PreeclampsiaDocument9 pagesAngiogenic Factors in PreeclampsiaAudrey Madina DewiNo ratings yet
- P Selectin 2Document7 pagesP Selectin 2DesyHandayaniNo ratings yet
- A Cross Sectional Study To Assess The SFLT - 1:PlGF Ratio in Pregnant Women With and Without PreeclampsiaDocument8 pagesA Cross Sectional Study To Assess The SFLT - 1:PlGF Ratio in Pregnant Women With and Without PreeclampsiaEvita LarasNo ratings yet
- Excess Placental Soluble Fms-Like Tyrosine Kinase 1 (Sflt1) May Contribute To Endothelial Dysfunction, Hypertension, and Proteinuria in PreeclampsiaDocument10 pagesExcess Placental Soluble Fms-Like Tyrosine Kinase 1 (Sflt1) May Contribute To Endothelial Dysfunction, Hypertension, and Proteinuria in PreeclampsiaEnrique RosasNo ratings yet
- Bimarker Aswin BoyDocument10 pagesBimarker Aswin BoyAswin BoyNo ratings yet
- Filosofia Del Cuerpo HumaniDocument14 pagesFilosofia Del Cuerpo HumaniCristina Galvez PerezNo ratings yet
- Preeclampsia: Maternal Systemic Vascular Disorder Caused by Generalized Endothelial Dysfunction Due To Placental Antiangiogenic FactorsDocument18 pagesPreeclampsia: Maternal Systemic Vascular Disorder Caused by Generalized Endothelial Dysfunction Due To Placental Antiangiogenic FactorsSherilinne Quiles LópezNo ratings yet
- SFLT 1Document10 pagesSFLT 1William Camilo Camargo MartinezNo ratings yet
- PLGF, sFlt-1 and sFlt-1/PlGF Ratio: Promising Markers For Predicting Pre-EclampsiaDocument6 pagesPLGF, sFlt-1 and sFlt-1/PlGF Ratio: Promising Markers For Predicting Pre-EclampsiaPeertechz Publications Inc.No ratings yet
- Chronic Kidney Disease May Be Differentially Diagnosed From Preeclampsia by Serum BiomarkersDocument5 pagesChronic Kidney Disease May Be Differentially Diagnosed From Preeclampsia by Serum BiomarkersmeliabudiNo ratings yet
- Mini-Review: Elizabeth Phipps, Devika Prasanna, Wunnie Brima, and Belinda JimDocument10 pagesMini-Review: Elizabeth Phipps, Devika Prasanna, Wunnie Brima, and Belinda JimemilyNo ratings yet
- Maternal Levels of Growth Differentiation Factor-15 in Patients With PreeclampsiaDocument6 pagesMaternal Levels of Growth Differentiation Factor-15 in Patients With PreeclampsiaqvldNo ratings yet
- Ihc 2Document5 pagesIhc 2DesyHandayaniNo ratings yet
- Investigational Approaches Biomarkers Angiogenic ModulatorsDocument2 pagesInvestigational Approaches Biomarkers Angiogenic ModulatorsKatherine GuijarroNo ratings yet
- Hemostatic Changes in Normal PregnancyDocument3 pagesHemostatic Changes in Normal PregnancyArfi FachrulNo ratings yet
- Hypertension 2011 Woods 94 102 3Document18 pagesHypertension 2011 Woods 94 102 3Nimas Luthfiana HapsariNo ratings yet
- Increased Sflt1/Plgf Ratio in Covid-19: A Novel Link To Angiotensin Ii-Mediated Endothelial DysfunctionDocument10 pagesIncreased Sflt1/Plgf Ratio in Covid-19: A Novel Link To Angiotensin Ii-Mediated Endothelial DysfunctioncirererereNo ratings yet
- Thrombin 10 PDFDocument5 pagesThrombin 10 PDFSaddam FuadNo ratings yet
- Diagnostic Accuracy of SFlt1PlGF Ratio As A MarkerDocument7 pagesDiagnostic Accuracy of SFlt1PlGF Ratio As A MarkerWahyudi WirawanNo ratings yet
- Prostasin, Proteases, and Preeclampsia.7Document3 pagesProstasin, Proteases, and Preeclampsia.7rachel0301No ratings yet
- Ajpheart 00045 2018Document15 pagesAjpheart 00045 2018kamkamNo ratings yet
- Decreased STAT3 in Human Idiopathic Fetal Growth Restriction Contributes To Trophoblast DysfunctionDocument10 pagesDecreased STAT3 in Human Idiopathic Fetal Growth Restriction Contributes To Trophoblast DysfunctionYosef Dwi Cahyadi SalanNo ratings yet
- 21, Hypoxia-Inducible Factor-1 Mediates The Biological Effects of Oxygen On Human Trophoblast Differentiation Through TGFbeta (3) .Document11 pages21, Hypoxia-Inducible Factor-1 Mediates The Biological Effects of Oxygen On Human Trophoblast Differentiation Through TGFbeta (3) .ari chandra ervinaNo ratings yet
- Kim 2009Document7 pagesKim 2009edelinNo ratings yet
- Angiogenic Factors in The Pathogenesis and Pathophysiology of Preeclampsia A Mini ReviewDocument7 pagesAngiogenic Factors in The Pathogenesis and Pathophysiology of Preeclampsia A Mini ReviewedelinNo ratings yet
- Thomas 2007Document11 pagesThomas 2007edelinNo ratings yet
- JurnalDocument2 pagesJurnalidhaNo ratings yet
- Fleming 2010Document4 pagesFleming 2010Ahmed GhanimNo ratings yet
- Pre-Eclampsia Prediction Panel - Anatomy, Etymology and AnalysisDocument1 pagePre-Eclampsia Prediction Panel - Anatomy, Etymology and AnalysisSalome Adame GuisadoNo ratings yet
- Journal 2Document14 pagesJournal 2Dio PattersonNo ratings yet
- Diagnostic Accuracy of SFlt1 - PLGF Ratio As A Marker For PreeclampsiaDocument6 pagesDiagnostic Accuracy of SFlt1 - PLGF Ratio As A Marker For PreeclampsiaWahyudi WirawanNo ratings yet
- Roberts CT, 2008Document6 pagesRoberts CT, 2008Anibal LeNo ratings yet
- Functions of p21 in Cell Cycle, Apoptosis and Transcriptional Regulation After DNA Damage-1Document33 pagesFunctions of p21 in Cell Cycle, Apoptosis and Transcriptional Regulation After DNA Damage-1rayanahfedanNo ratings yet
- Review Article: The Role of Estrogen in The Pathophysiology of Tubal Ectopic PregnancyDocument10 pagesReview Article: The Role of Estrogen in The Pathophysiology of Tubal Ectopic PregnancySri AgustinaNo ratings yet
- Pathophysiology of PreeclampsiaDocument4 pagesPathophysiology of PreeclampsiaRyan AndrianNo ratings yet
- Khalil2008 PDFDocument8 pagesKhalil2008 PDFArina RNo ratings yet
- Ovário 2Document9 pagesOvário 2Sandro PinhoNo ratings yet
- Birdir - J Matern Fetal Neonatal Med - 2017Document7 pagesBirdir - J Matern Fetal Neonatal Med - 2017Sayedur RahmanNo ratings yet
- New Developments in The Pathogenesis of Preeclampsia: Mihran V. NaljayanDocument12 pagesNew Developments in The Pathogenesis of Preeclampsia: Mihran V. NaljayanRaymond FrazierNo ratings yet
- 1 s2.0 S0898656822002972 MainDocument10 pages1 s2.0 S0898656822002972 Maindr. Nur'aini HasanNo ratings yet
- Antiphospholipid Antibody Syndrome Learnsimply Volume 11Document3 pagesAntiphospholipid Antibody Syndrome Learnsimply Volume 11Ashita DubeyNo ratings yet
- Preeclampsia and Glomerulonephritis: A Bidirectional AssociationDocument7 pagesPreeclampsia and Glomerulonephritis: A Bidirectional AssociationJesi Anggraini Ekaputri LubisNo ratings yet
- PI3K/AKT/mTOR Pathway in Angiogenesis: Molecular NeuroscienceDocument8 pagesPI3K/AKT/mTOR Pathway in Angiogenesis: Molecular NeuroscienceAbu KhairNo ratings yet
- P45NF-E2 Represses Gcm1 in Trophoblast Cells To ReDocument13 pagesP45NF-E2 Represses Gcm1 in Trophoblast Cells To ReM KashifNo ratings yet
- 1 s2.0 S0093691X1500182X MainDocument10 pages1 s2.0 S0093691X1500182X MainPâmela FreitasNo ratings yet
- Placental Lactogen As A Marker of Maternal Obesity, Diabetes, and Fetal Growth Abnormalities: Current Knowledge and Clinical PerspectivesDocument19 pagesPlacental Lactogen As A Marker of Maternal Obesity, Diabetes, and Fetal Growth Abnormalities: Current Knowledge and Clinical PerspectivesLigia AbdalaNo ratings yet
- What Causes NVPDocument14 pagesWhat Causes NVPFortuneNo ratings yet
- Altered Angiogenesis As A Common Mechanism Underlying Preterm Birth, Small For Gestational Age, and Stillbirth in Women Living With HIVDocument17 pagesAltered Angiogenesis As A Common Mechanism Underlying Preterm Birth, Small For Gestational Age, and Stillbirth in Women Living With HIVMuhammad Pebri Nilhakim ZavbmNo ratings yet
- Pathogenesis of Retinopathy of Prematurity: Lois E.H. SmithDocument5 pagesPathogenesis of Retinopathy of Prematurity: Lois E.H. SmithretajatiNo ratings yet
- Alt Coagulacion 08Document12 pagesAlt Coagulacion 08Brenda CaraveoNo ratings yet
- Mini-Review: Elizabeth Phipps, Devika Prasanna, Wunnie Brima, and Belinda JimDocument9 pagesMini-Review: Elizabeth Phipps, Devika Prasanna, Wunnie Brima, and Belinda JimemilyNo ratings yet
- Corto CTCF VegfDocument6 pagesCorto CTCF Vegfunknowncountdown167No ratings yet
- AJOG Publication, 2015 On GlyFNDocument9 pagesAJOG Publication, 2015 On GlyFNRaghavanNo ratings yet
- Prediction Using Serum Glycosylated Fibronectin of Imminent Pre Eclampsia in Women With New Onset HypertensionDocument7 pagesPrediction Using Serum Glycosylated Fibronectin of Imminent Pre Eclampsia in Women With New Onset HypertensionWahyudi WirawanNo ratings yet
- Combining Metformin and Esomep PDFDocument15 pagesCombining Metformin and Esomep PDFDirtie Imas HNo ratings yet
- A Novel Human-Specific Soluble Vascular Endothelial Growth Factor Receptor 1Document21 pagesA Novel Human-Specific Soluble Vascular Endothelial Growth Factor Receptor 1edelinNo ratings yet
- Comparative Study of Genexpert With ZN Stain and Culture in Samples of Suspected Pulmonary TuberculosisDocument9 pagesComparative Study of Genexpert With ZN Stain and Culture in Samples of Suspected Pulmonary TuberculosisEgi NabilaNo ratings yet
- LBP and RadiculopathyDocument4 pagesLBP and RadiculopathyEgi NabilaNo ratings yet
- REBA Employee Assessment Worksheet: A. Neck, Trunk and Leg AnalysisDocument1 pageREBA Employee Assessment Worksheet: A. Neck, Trunk and Leg AnalysisEgi NabilaNo ratings yet
- A Vital Direction For Health and Health Care: Addressing Social Determinants of Health and Health DisparitiesDocument16 pagesA Vital Direction For Health and Health Care: Addressing Social Determinants of Health and Health DisparitiesEgi NabilaNo ratings yet
- A Vital Direction For Health and Health Care: Addressing Social Determinants of Health and Health DisparitiesDocument16 pagesA Vital Direction For Health and Health Care: Addressing Social Determinants of Health and Health DisparitiesEgi NabilaNo ratings yet
- Universal Health Coverage in Latin America 3: SeriesDocument9 pagesUniversal Health Coverage in Latin America 3: SeriesEgi NabilaNo ratings yet
- Pregnancy HypertensionDocument7 pagesPregnancy HypertensionEgi NabilaNo ratings yet
- Social Determinants of Health: Best AdviceDocument21 pagesSocial Determinants of Health: Best AdviceEgi NabilaNo ratings yet
- An Interdisciplinary Community Diagnosis Experience in An Undergraduate Medical Curriculum: Development at Ghent UniversityDocument9 pagesAn Interdisciplinary Community Diagnosis Experience in An Undergraduate Medical Curriculum: Development at Ghent UniversityEgi NabilaNo ratings yet
- Articles: BackgroundDocument10 pagesArticles: BackgroundEgi NabilaNo ratings yet
- Horner Syndrome: Kelly A. Walton and Lawrence M. BuonoDocument7 pagesHorner Syndrome: Kelly A. Walton and Lawrence M. BuonoEgi NabilaNo ratings yet
- Epidemiology of Hay Fever: Towards A Community Diagnosis: ReviewDocument9 pagesEpidemiology of Hay Fever: Towards A Community Diagnosis: ReviewEgi NabilaNo ratings yet
- Glucose Intolerance and Insulin Resistance: Relevance in PreeclampsiaDocument14 pagesGlucose Intolerance and Insulin Resistance: Relevance in PreeclampsiaEgi NabilaNo ratings yet
- Finals Scope - Genetic.childbirthDocument4 pagesFinals Scope - Genetic.childbirthSharmaine MadlaNo ratings yet
- Adult CPR ProcedureDocument3 pagesAdult CPR ProcedureDaniica MacaranasNo ratings yet
- Informatika Farmasi - PBLDocument64 pagesInformatika Farmasi - PBLanisa rachmitaNo ratings yet
- Neuropsychology QuestionnaireDocument5 pagesNeuropsychology Questionnaireeva.mmNo ratings yet
- Great Medical Doctor CV ExampleDocument1 pageGreat Medical Doctor CV ExampleEkvan DanangNo ratings yet
- TERLIPRESSINDocument6 pagesTERLIPRESSINAnil Kumar SNo ratings yet
- Good Thesis Statement For Down SyndromeDocument5 pagesGood Thesis Statement For Down Syndromejamiemillerpeoria100% (2)
- Specific Criteria Nabl-112 (2012)Document53 pagesSpecific Criteria Nabl-112 (2012)kinnusaraiNo ratings yet
- 18 Main CH21.docx 1Document46 pages18 Main CH21.docx 1Emily AnnNo ratings yet
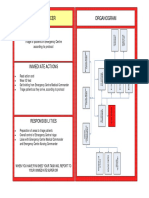
- Triage Officer Organogram: MissionDocument14 pagesTriage Officer Organogram: Missionsnow fazliNo ratings yet
- AFES FINAL Announcement As of 14 SepDocument16 pagesAFES FINAL Announcement As of 14 Sepvanhau24No ratings yet
- Joint Pain Leaflet PDFDocument12 pagesJoint Pain Leaflet PDFSuaeni Kurnia Wirda100% (1)
- Clorazepate Dipotassium (Drug Study)Document2 pagesClorazepate Dipotassium (Drug Study)Franz.thenurse6888No ratings yet
- Physical Assessment Kelompok 9Document13 pagesPhysical Assessment Kelompok 9Putri KinantiNo ratings yet
- Alexander: The Great Addiction: Waleed SamiDocument10 pagesAlexander: The Great Addiction: Waleed Samiapi-341492986No ratings yet
- Pet Healthcare SystemDocument14 pagesPet Healthcare SystemRixel Penoria BalacuitNo ratings yet
- 10 1001@jama 2019 0554 PDFDocument15 pages10 1001@jama 2019 0554 PDFFaisal Reza AdiebNo ratings yet
- Pe and Health Module - Mapeh 4 2nd SemDocument17 pagesPe and Health Module - Mapeh 4 2nd SemCleofe Sobiaco0% (1)
- Sept 4, 2015Document8 pagesSept 4, 2015Deity CelleNo ratings yet
- American Trypanosomiasis: Causative Agent: TrypanosomaDocument32 pagesAmerican Trypanosomiasis: Causative Agent: TrypanosomaMasali MacdonaNo ratings yet
- Concept of Health & DiseaseDocument46 pagesConcept of Health & DiseaseAnonymous rNu1uWjweNo ratings yet
- DR Dina - TB & CovidDocument10 pagesDR Dina - TB & CovidDina FaizahNo ratings yet
- Curious Case of Retrolental Mass: An Unusual Tele-Screening ArtifactDocument2 pagesCurious Case of Retrolental Mass: An Unusual Tele-Screening ArtifactRatneshNo ratings yet
- Conversion DisorderDocument49 pagesConversion DisorderSonali SawaleNo ratings yet
- Roy, Michael J - Biotechnology Operations - Principles and Practices-CRC Press (2011)Document412 pagesRoy, Michael J - Biotechnology Operations - Principles and Practices-CRC Press (2011)AllalannNo ratings yet
- HypertensionSeoul2020 AbstractDocument164 pagesHypertensionSeoul2020 AbstractRimaNo ratings yet
- Caap 19 - AeromedicalDocument139 pagesCaap 19 - AeromedicalShadabNo ratings yet