Download as pdf or txt
You might also like
- Normal Lab Values PDFDocument2 pagesNormal Lab Values PDFItharshan Indreswaran83% (18)
- Lesson Plan On - Essential-NewbornDocument22 pagesLesson Plan On - Essential-NewbornSwati Sharma100% (2)
- Swing Low, Sweet Chariot (Ma Del Carmen Aguilar)Document2 pagesSwing Low, Sweet Chariot (Ma Del Carmen Aguilar)Alejandro AllegraNo ratings yet
- Activity 2Document5 pagesActivity 2api-492104888100% (1)
- Advice Sheet A12 - Infection Control in Dentistry - Identist - 2 PDFDocument31 pagesAdvice Sheet A12 - Infection Control in Dentistry - Identist - 2 PDFizeldien5870No ratings yet
- 142 Ped Cystic FibrosisDocument9 pages142 Ped Cystic FibrosisritaNo ratings yet
- 143 Ped DehydrationDocument4 pages143 Ped DehydrationritaNo ratings yet
- Block 1Document22 pagesBlock 1ايات عبدالرحمنNo ratings yet
- 144 Ped Foreign Body IngestionDocument3 pages144 Ped Foreign Body IngestionritaNo ratings yet
- 0001 01 PDFDocument10 pages0001 01 PDFAmmar Al-basitiNo ratings yet
- Ith in L Ti I L in I Llitus Is Is Is Ic J in Int L Tid L LlowsDocument6 pagesIth in L Ti I L in I Llitus Is Is Is Ic J in Int L Tid L LlowsAlex ChenNo ratings yet
- MCR3 Funcional PDFDocument4 pagesMCR3 Funcional PDFLucas Mathias Lobos EtcheverriaNo ratings yet
- Item:: E L E EDocument7 pagesItem:: E L E Eshahbaz HazardousNo ratings yet
- Slewing Crane Schematic Diagram PDFDocument3 pagesSlewing Crane Schematic Diagram PDFachmadihinNo ratings yet
- Cortical Mastoidectomy Varsha MamDocument19 pagesCortical Mastoidectomy Varsha Mamrailabhi83No ratings yet
- Rabi3a Old Edittion 1985 Cairo University 2nd Petroleum 16Document319 pagesRabi3a Old Edittion 1985 Cairo University 2nd Petroleum 16Abdelaziz Mohamed Abdelmoaty Arafa100% (1)
- UW 2024 - OphthalmologyDocument204 pagesUW 2024 - Ophthalmology부산No ratings yet
- Img 20221014 0006Document1 pageImg 20221014 0006philipNo ratings yet
- Redistricting PacketDocument20 pagesRedistricting PacketWCTV Digital TeamNo ratings yet
- Ms Lecture 4 PDFDocument11 pagesMs Lecture 4 PDFAkash GolwalkarNo ratings yet
- 08 Dismantling Dim. & Part WeichtsDocument2 pages08 Dismantling Dim. & Part WeichtstruryNo ratings yet
- Scan 27 Oct 2022Document11 pagesScan 27 Oct 2022Noha badrNo ratings yet
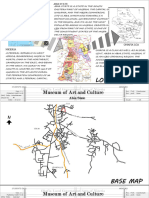
- Museum PrelimsDocument31 pagesMuseum PrelimsKraven KingsNo ratings yet
- Adobe Scan Mar 13, 2023Document9 pagesAdobe Scan Mar 13, 2023aroradoll210No ratings yet
- 158 Sur Rib FractureDocument12 pages158 Sur Rib Fracturerami ibrahiemNo ratings yet
- Why Ops. MatterDocument6 pagesWhy Ops. MatterPulkitNo ratings yet
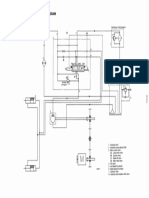
- Esquema zzr1100Document1 pageEsquema zzr1100miozao miozaoNo ratings yet
- KK 016Document1 pageKK 016Choky FhNo ratings yet
- ProjectileDocument46 pagesProjectileSneha KarkeeNo ratings yet
- OpthalmologyDocument45 pagesOpthalmologyWill HNo ratings yet
- Roland R8 Owners Manual (OCR)Document239 pagesRoland R8 Owners Manual (OCR)SteveNo ratings yet
- Shubh 0001Document6 pagesShubh 0001er.shubh0001No ratings yet
- .Fu-205 Vi-204Document115 pages.Fu-205 Vi-204Ismael A. BautistaNo ratings yet
- Digital Capacitance Meter: Electronic Instrumentati NDocument8 pagesDigital Capacitance Meter: Electronic Instrumentati NRama ChandraNo ratings yet
- SCHNEIDERS (00012) Periodic Billing Statement Period Ending 12.15.2015 - RedactedDocument1 pageSCHNEIDERS (00012) Periodic Billing Statement Period Ending 12.15.2015 - Redactedlarry-612445No ratings yet
- Laser Cutter Manual UeleleleDocument23 pagesLaser Cutter Manual UeleleleJ YapNo ratings yet
- Smart Lock ManualDocument4 pagesSmart Lock ManuallubisNo ratings yet
- Exercise 2 (2) - CoedDocument3 pagesExercise 2 (2) - CoedTIDEYNo ratings yet
- Btruool Assocurrs Lp: ltti郡Document3 pagesBtruool Assocurrs Lp: ltti郡Simon YiuNo ratings yet
- Shop Manual D 85SSDocument1 pageShop Manual D 85SSsigit prihantoNo ratings yet
- Juki LBH-781Document25 pagesJuki LBH-781Jei CabzNo ratings yet
- JUN 2 7 1990 Operating I Service Manual: Quick StartDocument6 pagesJUN 2 7 1990 Operating I Service Manual: Quick StartFouquetNo ratings yet
- Chapter 2Document18 pagesChapter 2Hadi SleemNo ratings yet
- Single Plate Framing Connection Design PDFDocument83 pagesSingle Plate Framing Connection Design PDFlaiju p b100% (1)
- Hmokpat:A A Ⅲ Ⅲ Ⅲ 田 01: EaahnikhDocument1 pageHmokpat:A A Ⅲ Ⅲ Ⅲ 田 01: EaahnikhPanos Hey Translations OfficialNo ratings yet
- Gama ING 6Document1 pageGama ING 6mbidNo ratings yet
- Clean Steam Generator-2Document71 pagesClean Steam Generator-2EwdinNo ratings yet
- Aln 1 Work at HieghtDocument1 pageAln 1 Work at HieghtStructural EngineerNo ratings yet
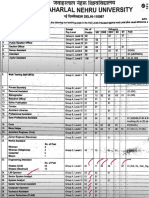
- JNU Non Teaching Recruitment 2023 Short NoticeDocument4 pagesJNU Non Teaching Recruitment 2023 Short NoticeVipin RoyalNo ratings yet
- Anritsu MF160xADocument3 pagesAnritsu MF160xAJosue PazNo ratings yet
- Calibración Termohigrometro 2019Document1 pageCalibración Termohigrometro 2019Chirley Jazmin Bayona BautistaNo ratings yet
- LD: 2658 Lab: 0. Previous Next Values Notes Calculator Reverse Color Text ZoomDocument5 pagesLD: 2658 Lab: 0. Previous Next Values Notes Calculator Reverse Color Text ZoomAlex ChenNo ratings yet
- Narsaraopeta FeederDocument1 pageNarsaraopeta FeederADE MRTNo ratings yet
- AppleliciousDocument6 pagesAppleliciousapi-117237667No ratings yet
- Modul Tutor THT 2018 PDFDocument1 pageModul Tutor THT 2018 PDFYelsintha SaalinoNo ratings yet
- Adobe Scan 22 Apr 2024Document1 pageAdobe Scan 22 Apr 2024anastarcontracting9No ratings yet
- Pages From Dorman Longs - Handbook For Constructional Engineers - 1895-64Document1 pagePages From Dorman Longs - Handbook For Constructional Engineers - 1895-64Fornvald TamasNo ratings yet
- Scan0023 Fig 1-121a To 121d PDFDocument1 pageScan0023 Fig 1-121a To 121d PDFJayson Jonson AraojoNo ratings yet
- Applelicious 1Document6 pagesApplelicious 1api-117237667No ratings yet
- Professional Parking Management CorporationDocument1 pageProfessional Parking Management CorporationJe RoNo ratings yet
- Ati RN Proctored Maternal Newborn Form C 2016Document2 pagesAti RN Proctored Maternal Newborn Form C 2016Stevania96% (27)
- Safety Devices Manual 7300 KOBELCO Crawler CraneDocument71 pagesSafety Devices Manual 7300 KOBELCO Crawler CraneWilliam ColinsNo ratings yet
- Su ND: Ly (/ /min, /minDocument3 pagesSu ND: Ly (/ /min, /minAlex ChenNo ratings yet
- E e - . Ea: ItemDocument5 pagesE e - . Ea: ItemAlex ChenNo ratings yet
- Item:: LD: 4239 Prevoous Next Lab Values Notes Calculator Reverse Color Text ZoomDocument5 pagesItem:: LD: 4239 Prevoous Next Lab Values Notes Calculator Reverse Color Text ZoomAlex ChenNo ratings yet
- Biochem Self-AssessmentDocument44 pagesBiochem Self-AssessmentAlex ChenNo ratings yet
- Item ,: Irt I I I I I I L in Ntil Vit L I Hy Ic L in V Ic Li Ill N Im I V L L Lvic I - in I Li LyDocument5 pagesItem ,: Irt I I I I I I L in Ntil Vit L I Hy Ic L in V Ic Li Ill N Im I V L L Lvic I - in I Li LyAlex ChenNo ratings yet
- E - . - E - Ess., .: 0. LD: 2728 Previous Next Lab Values Notes Calculator Reverse Color Text ZoomDocument5 pagesE - . - E - Ess., .: 0. LD: 2728 Previous Next Lab Values Notes Calculator Reverse Color Text ZoomAlex ChenNo ratings yet
- Absite - Chapter 3 PresentationDocument12 pagesAbsite - Chapter 3 PresentationAlex ChenNo ratings yet
- Su ND: o o o o o oDocument5 pagesSu ND: o o o o o oAlex ChenNo ratings yet
- Absite - Chapter 2 PresentationDocument6 pagesAbsite - Chapter 2 PresentationAlex ChenNo ratings yet
- Measures of DispersionDocument10 pagesMeasures of DispersionAlex ChenNo ratings yet
- Made by SS (A.Aladawy)Document8 pagesMade by SS (A.Aladawy)Alex ChenNo ratings yet
- 0: 2717 Previou Next Lab Values Notes Calculator Reverse Color Text ZoomDocument3 pages0: 2717 Previou Next Lab Values Notes Calculator Reverse Color Text ZoomAlex ChenNo ratings yet
- Absite - Chapter 1 Presentation With RevisionsDocument8 pagesAbsite - Chapter 1 Presentation With RevisionsAlex ChenNo ratings yet
- Su ND: o o o o oDocument3 pagesSu ND: o o o o oAlex ChenNo ratings yet
- Ith in L Ti I L in I Llitus Is Is Is Ic J in Int L Tid L LlowsDocument6 pagesIth in L Ti I L in I Llitus Is Is Is Ic J in Int L Tid L LlowsAlex ChenNo ratings yet
- Su ND: Eft e E. FDocument3 pagesSu ND: Eft e E. FAlex ChenNo ratings yet
- Su ND: ItemDocument4 pagesSu ND: ItemAlex ChenNo ratings yet
- Es - E E Ess. - Cat - E - E Es.: 0.: 4395 Previous Next Lab Values Notes Calculator Reverse Color Text ZoomDocument6 pagesEs - E E Ess. - Cat - E - E Es.: 0.: 4395 Previous Next Lab Values Notes Calculator Reverse Color Text ZoomAlex ChenNo ratings yet
- 0201 01Document3 pages0201 01Alex ChenNo ratings yet
- Q and AnswerDocument1 pageQ and AnswerAlex ChenNo ratings yet
- Case Report Glenohumeral Dysplasia, A Complication of Obstetrics Brachial Plexus PalsyDocument5 pagesCase Report Glenohumeral Dysplasia, A Complication of Obstetrics Brachial Plexus PalsyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Xtracorporeal 38 Weeks Diagnose andDocument18 pagesXtracorporeal 38 Weeks Diagnose andSiti RahayuNo ratings yet
- Performing Intermittent Straight CatheterizationDocument4 pagesPerforming Intermittent Straight CatheterizationMarcia AlmeidaNo ratings yet
- 2 51 1656420123 1ijmpsdec20221Document4 pages2 51 1656420123 1ijmpsdec20221TJPRC PublicationsNo ratings yet
- Published Shally IJARDocument8 pagesPublished Shally IJARJOSLINNo ratings yet
- Kon Et Al-1969-Journal of PeriodontologyDocument16 pagesKon Et Al-1969-Journal of Periodontologyshir keshalesNo ratings yet
- CAGE Test Alcool, CAGE Test Droguri, Test AUDIT Pentru Alcoolism. Ce Este Adictia. Coping Si TratamentDocument35 pagesCAGE Test Alcool, CAGE Test Droguri, Test AUDIT Pentru Alcoolism. Ce Este Adictia. Coping Si TratamentAnonymous KgUtPlkjNo ratings yet
- Survival Guide 2014 2015Document107 pagesSurvival Guide 2014 2015Manpreet BajwaNo ratings yet
- Avascular Necrosis - Causes, Symptoms, Prevention & TreatmentDocument26 pagesAvascular Necrosis - Causes, Symptoms, Prevention & TreatmentSatrio Bangun NegoroNo ratings yet
- 2016 Psychaitric Nursing Problem StatementsDocument10 pages2016 Psychaitric Nursing Problem StatementsMAHESH KOUJALAGI100% (1)
- Overview of CMAMDocument33 pagesOverview of CMAMMd Faruque Ahmad100% (1)
- Deaf CommunityDocument11 pagesDeaf Communityapi-272869175No ratings yet
- Bulacan State University College of Nursing City of Malolos, BulacanDocument2 pagesBulacan State University College of Nursing City of Malolos, BulacanMia PascualNo ratings yet
- Mapeh 10Document2 pagesMapeh 10Joan VecillaNo ratings yet
- 01 STR 29 1 251Document6 pages01 STR 29 1 251RAFAEL BRITONo ratings yet
- Legal Steroids PDF (V2) PDFDocument22 pagesLegal Steroids PDF (V2) PDFAakshi JairathNo ratings yet
- Strokeaha 120 033033Document7 pagesStrokeaha 120 033033AudryaNo ratings yet
- Posterior Circulation StrokeDocument11 pagesPosterior Circulation Strokenitish kumar100% (1)
- Chapter 3 Neuroimmune Aspects of Sleep and Wakefulness: August 2016Document20 pagesChapter 3 Neuroimmune Aspects of Sleep and Wakefulness: August 2016Ganjar AdityoNo ratings yet
- PLASMAPHERESISDocument18 pagesPLASMAPHERESISmuhammad24fayazNo ratings yet
- SHIROVASTIDocument3 pagesSHIROVASTINatseenNo ratings yet
- Spelling Mistakes Corrections of Jahangir's Pool of FCPS Part 1 DentistryDocument16 pagesSpelling Mistakes Corrections of Jahangir's Pool of FCPS Part 1 DentistryAisha BanoNo ratings yet
- Heartbeat HomeostasisDocument1 pageHeartbeat Homeostasisapi-296692561No ratings yet
- Pharmacology CardiovascularDocument86 pagesPharmacology Cardiovascularamasoud96 amasoud96No ratings yet
- Reynaud's DseDocument6 pagesReynaud's DseKengkai MiiNo ratings yet
- 483-Article Text-1867-1-10-20201110Document5 pages483-Article Text-1867-1-10-20201110IT AAMC CellNo ratings yet
- 2023 EDITED EP-Lian-C3-Socio-Part-3Document35 pages2023 EDITED EP-Lian-C3-Socio-Part-3Mark Andrei GubacNo ratings yet