Download as pdf or txt
You might also like
- Chicken-Pox Concept MapDocument4 pagesChicken-Pox Concept MapElle0% (1)
- Tuberculosis 1. Background of The Problem Chickenpox Is A Highly Contagious Disease Caused by Primary Infection With VaricellaDocument6 pagesTuberculosis 1. Background of The Problem Chickenpox Is A Highly Contagious Disease Caused by Primary Infection With VaricellaFkrygeustobat Tikamarimunteupercaya TanyakeunkajalminaNo ratings yet
- Nassef2015 PDFDocument6 pagesNassef2015 PDFBilel DhaouadiNo ratings yet
- Complicated MeaslesDocument13 pagesComplicated MeaslesFarica Armane AquinoNo ratings yet
- Kutis PorcelanaDocument34 pagesKutis Porcelanaapi-3743483No ratings yet
- Journal Reading - Nurul Nadifa Erza - 2010221012 - Insight Into ScabiesDocument24 pagesJournal Reading - Nurul Nadifa Erza - 2010221012 - Insight Into ScabiesNurul Nadifa ErzaNo ratings yet
- Chickenpox Chickenpox Is A Highly Contagious Disease Caused by Primary Infection With Varicella ZosterDocument12 pagesChickenpox Chickenpox Is A Highly Contagious Disease Caused by Primary Infection With Varicella Zostersubbu2raj3372100% (2)
- Meehleib, Rachelle Ayn S. Pepino, Stephanie Kate ADocument16 pagesMeehleib, Rachelle Ayn S. Pepino, Stephanie Kate ARachelle AynNo ratings yet
- Oral Manifestations Ofviral InfectionsDocument5 pagesOral Manifestations Ofviral InfectionsNur Adha AtjoNo ratings yet
- W9 Measles German Measles Influenza Chicken Pox Covid19Document16 pagesW9 Measles German Measles Influenza Chicken Pox Covid19Jamie De LunaNo ratings yet
- Assignment IndividualDocument10 pagesAssignment Individualkartini272597No ratings yet
- Common Child and AdolescentDocument23 pagesCommon Child and AdolescentValeria BeltranNo ratings yet
- SKIN Viral InfectionDocument85 pagesSKIN Viral InfectionNica RTNo ratings yet
- 1) - Oral Exam Revealed A White Strawberry Tongue: Ecker, Habashy, SkopitDocument5 pages1) - Oral Exam Revealed A White Strawberry Tongue: Ecker, Habashy, SkopitAngela DuangchitNo ratings yet
- PAEDS 4 - 18.10.19 Viral InfectionDocument15 pagesPAEDS 4 - 18.10.19 Viral Infectionlotp12No ratings yet
- ImpetigoDocument3 pagesImpetigopcarty98No ratings yet
- Common Diseases in MalaysiaDocument9 pagesCommon Diseases in Malaysiafarishahanis07No ratings yet
- Oral Viral Infections Diagnosis and ManagementDocument13 pagesOral Viral Infections Diagnosis and ManagementhunarsandhuNo ratings yet
- 000 .ZH-CN - enDocument2 pages000 .ZH-CN - enkynaloughlinNo ratings yet
- Pediatrics CR Day 1 and 3Document26 pagesPediatrics CR Day 1 and 3CC Samson, Caesar AnthonyNo ratings yet
- Mayores. Chicken Pox - Concept MapDocument3 pagesMayores. Chicken Pox - Concept MapAlvic Dy KowNo ratings yet
- Clinical Features of Viral Exanthems: Sarajane Ting, Rosemary NixonDocument6 pagesClinical Features of Viral Exanthems: Sarajane Ting, Rosemary NixonJustine Frances CabalayNo ratings yet
- Jurnal AcneDocument10 pagesJurnal Acneasep budiyantoNo ratings yet
- Pcfm-Enterovirus InfectionsDocument7 pagesPcfm-Enterovirus InfectionsZarene AnnNo ratings yet
- Measles: Complications PreventionDocument3 pagesMeasles: Complications PreventionAn NieNo ratings yet
- 1 s2.0 S0365059622000204 MainDocument5 pages1 s2.0 S0365059622000204 MainRizky RahmaNo ratings yet
- Chickenpox: 2008/9 Schools Wikipedia Selection Health and MedicineDocument5 pagesChickenpox: 2008/9 Schools Wikipedia Selection Health and MedicinenvijaykanthNo ratings yet
- Accepted Manuscript: Clinics in DermatologyDocument43 pagesAccepted Manuscript: Clinics in DermatologyanandaacpNo ratings yet
- HFMDDocument49 pagesHFMDDr.snehal patilNo ratings yet
- REFERAT - Meassles - FirdaDocument19 pagesREFERAT - Meassles - FirdaEriza LuthfansyahNo ratings yet
- Communicable Diseases: Rubella, Rubeola, Roseola, Fifth's Disease, Chicken Pox, Scarlet Fever, MononucleosisDocument16 pagesCommunicable Diseases: Rubella, Rubeola, Roseola, Fifth's Disease, Chicken Pox, Scarlet Fever, MononucleosisdrnasrallahNo ratings yet
- Dermatologic Manifestations of Rubella: FrequencyDocument10 pagesDermatologic Manifestations of Rubella: FrequencyImad MakkiNo ratings yet
- Streptococcal Pharyngitis: Clinical PracticeDocument8 pagesStreptococcal Pharyngitis: Clinical PracticeMilagros DiazNo ratings yet
- Impetigo SurveilensDocument10 pagesImpetigo SurveilensSitipradyta KasimNo ratings yet
- Hand Foot and Mouth Disease by RajDocument10 pagesHand Foot and Mouth Disease by RajedsymbiosisNo ratings yet
- Hand-Foot-And - Mouth DiseaseDocument27 pagesHand-Foot-And - Mouth DiseaseNur IzzahNo ratings yet
- Bullous Impetigo Case Series: An Updated Review: Mariam Hasan Rizvi, Sina AzizDocument5 pagesBullous Impetigo Case Series: An Updated Review: Mariam Hasan Rizvi, Sina AzizsayasajaNo ratings yet
- Virus Paramyxovirus: MorbillivirusDocument9 pagesVirus Paramyxovirus: MorbillivirusRhoda Mae Dano JandayanNo ratings yet
- Varicella/Herpes Zoster: Communicable Disease Management ProtocolDocument5 pagesVaricella/Herpes Zoster: Communicable Disease Management Protocolyuliyanto.efendiNo ratings yet
- CHN - Communicable DiseaseDocument117 pagesCHN - Communicable DiseaseGetom NgukirNo ratings yet
- Meningococcemia: N F S LDocument45 pagesMeningococcemia: N F S LMarky Roque100% (1)
- Nursing Therapeutics Specifically For Children and Adolescents With Infectious DiseasesDocument86 pagesNursing Therapeutics Specifically For Children and Adolescents With Infectious Diseasesgladz25No ratings yet
- 308-Article Text-623-1-10-20161213Document3 pages308-Article Text-623-1-10-20161213fadiah maharaniNo ratings yet
- Verruca Vulgaris in A Non-Immunocompromised Patient: Case ReportDocument4 pagesVerruca Vulgaris in A Non-Immunocompromised Patient: Case ReportBryan Eliezer SitumorangNo ratings yet
- Diagnosis and Treatment of Otitis MediaDocument9 pagesDiagnosis and Treatment of Otitis Mediaburbu1490No ratings yet
- Patho Unit 5Document37 pagesPatho Unit 5Shafiya ShaikNo ratings yet
- Appendix 8 Sample Notification Letters To ParentsDocument12 pagesAppendix 8 Sample Notification Letters To ParentsEdward AkumNo ratings yet
- Celulitis Odontogenica en Niños Caso Clinico 2Document6 pagesCelulitis Odontogenica en Niños Caso Clinico 2ana mariaNo ratings yet
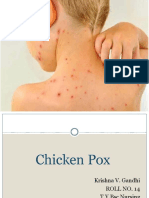
- Chicken PoxDocument26 pagesChicken PoxKrishna GandhiNo ratings yet
- M13 - Dermatology - Chapter 6Document9 pagesM13 - Dermatology - Chapter 6Idham BaharudinNo ratings yet
- Coxsackie Virus: The Hand, Foot, Mouth Disease (HFMD) : Review ArticleDocument5 pagesCoxsackie Virus: The Hand, Foot, Mouth Disease (HFMD) : Review ArticleDevyta Christia HeldisaniNo ratings yet
- Insect BitesDocument26 pagesInsect BiteszeniafadilaNo ratings yet
- Insight Into ScabiesDocument3 pagesInsight Into ScabiesVicky Pérez KlalaNo ratings yet
- Viral InfectionsDocument34 pagesViral InfectionsAlaa MadmoujNo ratings yet
- HFMDDocument9 pagesHFMDAnindita PramadyasiwiNo ratings yet
- Meningococcal Disease: Communicable Diseases FactsheetDocument3 pagesMeningococcal Disease: Communicable Diseases FactsheetDaisy HuntlyNo ratings yet
- A Simple Guide to Childhood Infectious DiseasesFrom EverandA Simple Guide to Childhood Infectious DiseasesRating: 5 out of 5 stars5/5 (1)
- Practical Insights into Atopic DermatitisFrom EverandPractical Insights into Atopic DermatitisKwang Hoon LeeNo ratings yet
- The Application of Kvaal's Dental Age Calculation Technique On Panoramic Dental RadiographsDocument11 pagesThe Application of Kvaal's Dental Age Calculation Technique On Panoramic Dental RadiographsgiselaNo ratings yet
- Sperti Bapa Sayang AnaknyaDocument3 pagesSperti Bapa Sayang AnaknyagiselaNo ratings yet
- Pus TakaDocument2 pagesPus TakagiselaNo ratings yet
- Colors of The WindDocument1 pageColors of The WindgiselaNo ratings yet
- VirologyLearnTable 2017-Sketchy PDFDocument4 pagesVirologyLearnTable 2017-Sketchy PDFdfgbdfgNo ratings yet
- Autoimmunity Reviews: A. Greco, M. Fusconi, A. Gallo, C. Marinelli, G.F. Macri, M. de VincentiisDocument6 pagesAutoimmunity Reviews: A. Greco, M. Fusconi, A. Gallo, C. Marinelli, G.F. Macri, M. de Vincentiisronaldyohanesf87No ratings yet
- Enteroviruses: Presented By: Andrea Dora J. Ortaliz MD-2Document56 pagesEnteroviruses: Presented By: Andrea Dora J. Ortaliz MD-2Andrea Dora OrtalizNo ratings yet
- National Public Health Laboratory Test Handbook 2018 FINAL (28082018)Document276 pagesNational Public Health Laboratory Test Handbook 2018 FINAL (28082018)MelvinNo ratings yet
- Viral MeningitisDocument4 pagesViral MeningitisSam TagardaNo ratings yet
- Protocolo Meningitis Def Marzo 2017Document29 pagesProtocolo Meningitis Def Marzo 2017Marcos Alberto Añasco ArelaNo ratings yet
- Chapter 32 - Viral Infections of The Nervous System and Prion DiseasesDocument46 pagesChapter 32 - Viral Infections of The Nervous System and Prion DiseasesUmar IslamiNo ratings yet
- Herpangina StatPearls NCBIBookshelfDocument2 pagesHerpangina StatPearls NCBIBookshelfThaysa BarbosaNo ratings yet
- Rhino VirusesDocument20 pagesRhino VirusesstudymedicNo ratings yet
- Viral Meningitis: David R. ChadwickDocument14 pagesViral Meningitis: David R. ChadwickVina HardiantiNo ratings yet
- Coxsackievirus: Incubation Period: 2-9 DaysDocument4 pagesCoxsackievirus: Incubation Period: 2-9 DaysrachellesliedeleonNo ratings yet
- Picornaviridae - CDocument9 pagesPicornaviridae - Cميمونه عبد الرحيم مصطفىNo ratings yet
- Acute Encephalitis SyndromeDocument116 pagesAcute Encephalitis SyndromePrateek Kumar PandaNo ratings yet
- PICORNAVIRUS (Enterovirus & Rhinovirus)Document27 pagesPICORNAVIRUS (Enterovirus & Rhinovirus)FarlogyNo ratings yet
- Literature Review Hand Foot Mouth DiseaseDocument5 pagesLiterature Review Hand Foot Mouth Diseasetqpkpiukg100% (1)
- Virology Micro D&R AgamDocument142 pagesVirology Micro D&R AgamNirosha Arul100% (1)
- Success VirologyDocument7 pagesSuccess VirologyRosh Hashana Louisse MatbaganNo ratings yet
- General Characteristics and Classification of The Picornavirus Family, Distribution in NatureDocument13 pagesGeneral Characteristics and Classification of The Picornavirus Family, Distribution in NatureSalma Mohamed RezkNo ratings yet
- Wastewater CharacteristicsDocument64 pagesWastewater CharacteristicsRicamaeNo ratings yet
- Virology TableDocument6 pagesVirology TablejeffdelacruzNo ratings yet
- RNA VirusesDocument11 pagesRNA VirusesKate Alyssa CatonNo ratings yet
- Viral MeningitisDocument4 pagesViral MeningitisLucky PuspitasariNo ratings yet
- Meningitis MedscapeDocument73 pagesMeningitis MedscapeBujangNo ratings yet
- Aseptic MeningitisDocument4 pagesAseptic MeningitisCheng XinvennNo ratings yet
- Combine PDFDocument91 pagesCombine PDFIbrahim SawaftaNo ratings yet
- Aseptic Meningitis in Adults - UpToDateDocument16 pagesAseptic Meningitis in Adults - UpToDateKondász Antal Gábor MedNo ratings yet
- Aseptic Meningitis: Exams and TestsDocument8 pagesAseptic Meningitis: Exams and TestsJoylyn Sagon VergaraNo ratings yet
- MeningitisDocument23 pagesMeningitisPutri RamadhaniNo ratings yet
- Bacterial MeningitisDocument30 pagesBacterial MeningitisFaris Alarshani100% (1)
- Data CDC Gov PDFDocument176 pagesData CDC Gov PDFnowayNo ratings yet