Download as pdf or txt
You might also like
- Final Report RSADocument27 pagesFinal Report RSAMounesh Panchal67% (3)
- Acellular Pertussis Vaccine Effectiveness Over Time: ObjectivesDocument11 pagesAcellular Pertussis Vaccine Effectiveness Over Time: ObjectivesLee제노No ratings yet
- Acellular Pertussis Vaccine Effectiveness Over Time: ObjectivesDocument11 pagesAcellular Pertussis Vaccine Effectiveness Over Time: Objectives[JC]No ratings yet
- 9.2018. Updates On Tdap Vaccination During PregnancyDocument2 pages9.2018. Updates On Tdap Vaccination During Pregnancyrosatikah ahmadNo ratings yet
- Peds 2012-3836 FullDocument9 pagesPeds 2012-3836 FullAnonymous hK8RDoNo ratings yet
- Pertussis Fact Sheet: National Centre For Immunisation Research and SurvelianceDocument4 pagesPertussis Fact Sheet: National Centre For Immunisation Research and SurveliancePaul GallagherNo ratings yet
- Peds 2023-062664Document11 pagesPeds 2023-062664Asti NuriatiNo ratings yet
- Protecting Infants From Pertussis: Child Health UpdateDocument3 pagesProtecting Infants From Pertussis: Child Health UpdateFadjrin Muhammad BazliNo ratings yet
- The Optimal Strategy For Pertussis Vaccination: A Systematic Review and Meta-Analysis of Randomized Control Trials and Real-World DataDocument26 pagesThe Optimal Strategy For Pertussis Vaccination: A Systematic Review and Meta-Analysis of Randomized Control Trials and Real-World DataIdmNo ratings yet
- Tdap Toolkit 2017Document8 pagesTdap Toolkit 2017Nica Joy DesquitadoNo ratings yet
- Apnea e InmunizacionDocument6 pagesApnea e InmunizacionLucía PaolinNo ratings yet
- C-Reactive Protein and Respiratory Distress SyndromeDocument1 pageC-Reactive Protein and Respiratory Distress SyndromeYunusNo ratings yet
- 1 s2.0 S1875957210000185 Main PDFDocument4 pages1 s2.0 S1875957210000185 Main PDFirs2407No ratings yet
- Profilaxis FiebreDocument10 pagesProfilaxis FiebreAlicia Montagud TeijeloNo ratings yet
- Pi Is 1875957219305510Document10 pagesPi Is 1875957219305510madimadi11No ratings yet
- Fimmu 11 00555Document14 pagesFimmu 11 00555Paula VargasNo ratings yet
- E20181565 Full-2 PDFDocument13 pagesE20181565 Full-2 PDFtazNo ratings yet
- Jurnal Anak RirinDocument10 pagesJurnal Anak RirinDexter BluesNo ratings yet
- DPBH Technical Bulletin 06-06-16 - Use of Tdap and TD VaccineDocument1 pageDPBH Technical Bulletin 06-06-16 - Use of Tdap and TD VaccineBlayne OsbornNo ratings yet
- Wright Et Al 2022 PDFDocument9 pagesWright Et Al 2022 PDFRadu CiprianNo ratings yet
- Infancy Interchangeability of 2 Diphtheria-Tetanus-Acellular Pertussis Vaccines inDocument9 pagesInfancy Interchangeability of 2 Diphtheria-Tetanus-Acellular Pertussis Vaccines inMargaretha MonikaNo ratings yet
- Combined Tetanus, Diphtheria, and 5-Component Pertussis Vaccine For Use in Adolescents and AdultsDocument10 pagesCombined Tetanus, Diphtheria, and 5-Component Pertussis Vaccine For Use in Adolescents and Adultsatika sgrtNo ratings yet
- Joc 50057Document10 pagesJoc 50057Sudarman Abdul RahmanNo ratings yet
- Tugas Ujian Akhir Semester Epidemiologi LanjutDocument12 pagesTugas Ujian Akhir Semester Epidemiologi LanjutYuniar PutriNo ratings yet
- Can Tey 2015Document4 pagesCan Tey 2015irenesmbNo ratings yet
- Comparison of Salbutamol and Nifedipine in Treatment of Preterm LabourDocument4 pagesComparison of Salbutamol and Nifedipine in Treatment of Preterm LabourAnonymous nhaFUpOLNo ratings yet
- Pediatric Critical Care MedicineDocument107 pagesPediatric Critical Care Medicinerahmawatusayu100% (1)
- Immune Interference (Blunting) in The Context of Maternal Immunization With Tdap-Containing Vaccines: Is It A Class Effect?Document13 pagesImmune Interference (Blunting) in The Context of Maternal Immunization With Tdap-Containing Vaccines: Is It A Class Effect?TheBNo ratings yet
- Safety Surveillance of Diphtheria and Tetanus Toxoids and Acellular Pertussis (Dtap) VaccinesDocument9 pagesSafety Surveillance of Diphtheria and Tetanus Toxoids and Acellular Pertussis (Dtap) VaccinesHansley Templeton CookNo ratings yet
- Association of Tdap Vaccination With Acute Events and Adverse Birth Outcomes Among Pregnant Women With Prior Tetanus-Containing ImmunizationsDocument7 pagesAssociation of Tdap Vaccination With Acute Events and Adverse Birth Outcomes Among Pregnant Women With Prior Tetanus-Containing ImmunizationsJosselyn PilcoNo ratings yet
- CEP Fluconazole Prophylaxis For Prevention of Invasive Candidiasis in Extremely Preterm InfantsDocument2 pagesCEP Fluconazole Prophylaxis For Prevention of Invasive Candidiasis in Extremely Preterm InfantsElison J PanggaloNo ratings yet
- Objective Study Design: M P, MD, S B. K, MD, K L. A, P D, H S. B, MDDocument6 pagesObjective Study Design: M P, MD, S B. K, MD, K L. A, P D, H S. B, MDSY LodhiNo ratings yet
- Poi 130021Document5 pagesPoi 130021Olivia DwimaswastiNo ratings yet
- Nur Fad IllahDocument7 pagesNur Fad Illahnirma sariNo ratings yet
- Immunizations in PregnancyDocument47 pagesImmunizations in Pregnancymiss_izzniNo ratings yet
- Epinephrine and Dexamethasone in Children With BronchiolitisDocument11 pagesEpinephrine and Dexamethasone in Children With BronchiolitisAdelina Wahyuni LubisNo ratings yet
- Multicentric Hospital-Based Surveillance of Pertussis Amongst Infants Admitted in Tertiary Care Facilities in IndiaDocument11 pagesMulticentric Hospital-Based Surveillance of Pertussis Amongst Infants Admitted in Tertiary Care Facilities in IndiaOleOhhNo ratings yet
- Postvaccination Febrile Seizure Severity and OutcomeDocument11 pagesPostvaccination Febrile Seizure Severity and OutcomeGrace Malinda LimopranotoNo ratings yet
- StefanelliDocument5 pagesStefanelliYuscha AnindyaNo ratings yet
- Tdap Vaccine Effectiveness in Adolescents (Acosta 2017)Document11 pagesTdap Vaccine Effectiveness in Adolescents (Acosta 2017)gd_hbarNo ratings yet
- Blum Er 2016Document7 pagesBlum Er 2016Vinsensius Rubin Ferreri ArismarjiantoNo ratings yet
- 2001 - Diagnosis of Pediatric Tuberculosis Using The Indonesian National Concencus For Pediatric TuberculosisDocument5 pages2001 - Diagnosis of Pediatric Tuberculosis Using The Indonesian National Concencus For Pediatric TuberculosisTammy Utami DewiNo ratings yet
- Non-Specific Effects of Diphtheria-Tetanus-Pertussis and Measles Vaccinations? An Analysis of Surveillance Data From Navrongo, GhanaDocument14 pagesNon-Specific Effects of Diphtheria-Tetanus-Pertussis and Measles Vaccinations? An Analysis of Surveillance Data From Navrongo, GhanaDyane VatriciaNo ratings yet
- Childhood Community Acquired Pneumonia A Review of Etiology and Antimicrobial Treatment Studies.Document10 pagesChildhood Community Acquired Pneumonia A Review of Etiology and Antimicrobial Treatment Studies.Andry Wahyudi AgusNo ratings yet
- 431 2019 Article 3563Document8 pages431 2019 Article 3563chindiaNo ratings yet
- Impact of Prophylactic Continuous Positive Airway Pressure On Transient Tachypnea of The Newborn and Neonatal Intensive Care Admission in Newborns Delivered by Elective Cesarean SectionDocument8 pagesImpact of Prophylactic Continuous Positive Airway Pressure On Transient Tachypnea of The Newborn and Neonatal Intensive Care Admission in Newborns Delivered by Elective Cesarean SectionFabiano SilvaNo ratings yet
- ftv074 PDFDocument9 pagesftv074 PDFanka_mihaelaNo ratings yet
- 2010 Early CPAP Vs Surfactant in EPTI NEJMDocument10 pages2010 Early CPAP Vs Surfactant in EPTI NEJMFiorella VilcaNo ratings yet
- PCP Pertussis Outbreak Rev 3 - 1Document3 pagesPCP Pertussis Outbreak Rev 3 - 1Mark Philipp AbanNo ratings yet
- Probiotics and Child Care Absence Due To Infections: A Randomized Controlled TrialDocument11 pagesProbiotics and Child Care Absence Due To Infections: A Randomized Controlled TrialMuhammad FebrianNo ratings yet
- The Value of Chest Radiography in Tuberculosis Preventive Treatment Screening in Children and AdolescentsDocument3 pagesThe Value of Chest Radiography in Tuberculosis Preventive Treatment Screening in Children and AdolescentsMaria José AlzateNo ratings yet
- Dargaville 2021Document10 pagesDargaville 2021Radu CiprianNo ratings yet
- Does Antenatal Corticosteroid Therapy Improve Neonatal Outcomes in Late Preterm Birth?Document8 pagesDoes Antenatal Corticosteroid Therapy Improve Neonatal Outcomes in Late Preterm Birth?faikaoesmaniaNo ratings yet
- J Pediatr 2023Document6 pagesJ Pediatr 2023cdsaludNo ratings yet
- Ped ProcalcitoninasepsisneoDocument11 pagesPed ProcalcitoninasepsisneoMirna Karime Gar CerNo ratings yet
- PertussisDocument8 pagesPertussisomjoshNo ratings yet
- A. Brief Resume of Intended WorkDocument6 pagesA. Brief Resume of Intended WorkRabi DhakalNo ratings yet
- Cap 2023Document9 pagesCap 2023Neonatología HGO4No ratings yet
- Bjgpopen18x101457 FullDocument8 pagesBjgpopen18x101457 FullchairunnisyaNo ratings yet
- A Practical Guide to Palliative Care in PaediatricsFrom EverandA Practical Guide to Palliative Care in PaediatricsRating: 5 out of 5 stars5/5 (1)
- A Practical Guide to Palliative Care in Paediatrics: Paediatric Palliative Care for Health ProfessionalsFrom EverandA Practical Guide to Palliative Care in Paediatrics: Paediatric Palliative Care for Health ProfessionalsNo ratings yet
- Jurnal DR AspriDocument18 pagesJurnal DR AspriManusia biasaNo ratings yet
- JPNC 04 00136Document5 pagesJPNC 04 00136Manusia biasaNo ratings yet
- Elis Statdas 1Document10 pagesElis Statdas 1Manusia biasaNo ratings yet
- No. NPM Nama K.1 K.Ii UTS UAS TugasDocument10 pagesNo. NPM Nama K.1 K.Ii UTS UAS TugasManusia biasaNo ratings yet
- Qualitative Research in Management Addresing Complexity Context and PersonaDocument13 pagesQualitative Research in Management Addresing Complexity Context and Personaalbadr20205026No ratings yet
- Stat 372 Midterm W14 SolutionDocument4 pagesStat 372 Midterm W14 SolutionAdil AliNo ratings yet
- BPE 3.0 Service Creditcards.1.06Document12 pagesBPE 3.0 Service Creditcards.1.06rainashwetaNo ratings yet
- CD Revised Module For DTUDocument147 pagesCD Revised Module For DTUኃይለ ማርያም አዲሱNo ratings yet
- Eegame LogcatDocument42 pagesEegame LogcatKelvin AlexanderNo ratings yet
- Exploration of Geriatric Care Competencies In.4Document8 pagesExploration of Geriatric Care Competencies In.4Mesh CoyivNo ratings yet
- Chapter 3 SolidDocument59 pagesChapter 3 Solidatikah roshanNo ratings yet
- AS-B Specification Sheet - SmartStruxure SolutionDocument12 pagesAS-B Specification Sheet - SmartStruxure SolutionOs ShNo ratings yet
- Nova ZelandiaDocument1 pageNova ZelandiaVinicius BorsatoNo ratings yet
- List of Formulas Useful For Solving Aptitude QuestionsDocument5 pagesList of Formulas Useful For Solving Aptitude Questionssrokar1234No ratings yet
- Afm ButterflyDocument5 pagesAfm ButterflyAna-Maria MaticuNo ratings yet
- Nptel: Power Electronics Applications To Power Systems - Video CourseDocument2 pagesNptel: Power Electronics Applications To Power Systems - Video Courseprafful666No ratings yet
- 4e HydraulischePressenDocument28 pages4e HydraulischePressenTirtheshwar Singh100% (1)
- Ph-Metro Sobremesa Orion Serie Star A211Document2 pagesPh-Metro Sobremesa Orion Serie Star A211Silvana Elena Montecino San MartínNo ratings yet
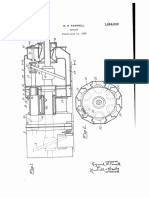
- Wwkzii: Jan. 10, 1933. R. H. FarwellDocument3 pagesWwkzii: Jan. 10, 1933. R. H. Farwellmonem2014100% (1)
- PC-Sample QuestionsDocument24 pagesPC-Sample QuestionsHeather EllaineNo ratings yet
- DD Env 12018-1998Document96 pagesDD Env 12018-1998Виктор ИсакNo ratings yet
- MarimbaDocument13 pagesMarimbarolaescobar16120% (1)
- 1 - Matrix Method of Structural AnalysisDocument5 pages1 - Matrix Method of Structural AnalysistrixiaNo ratings yet
- ALM 12 Benchmark Testing Tool DocumentationDocument22 pagesALM 12 Benchmark Testing Tool DocumentationjosephNo ratings yet
- 21mab102t Model MCQ Unit I To VDocument16 pages21mab102t Model MCQ Unit I To Vsd9422No ratings yet
- Impinj Monza R6 DatasheetDocument21 pagesImpinj Monza R6 Datasheettassa rifiutiNo ratings yet
- Intoduction To ComputingDocument292 pagesIntoduction To ComputingNem KumarNo ratings yet
- Nso Class-7Document3 pagesNso Class-7Swati AshtakeNo ratings yet
- Basics of Motor Starters and ContactorsDocument37 pagesBasics of Motor Starters and ContactorsTrifonas Krommidas100% (1)
- Page Description Change: Elektrobudowa SaDocument2 pagesPage Description Change: Elektrobudowa SaLý Chính ĐạoNo ratings yet
- Homeinteriorpaint FractionsdecimalsandpercentsDocument4 pagesHomeinteriorpaint Fractionsdecimalsandpercentsapi-281744400No ratings yet
- Ordinary Differential EquationsDocument317 pagesOrdinary Differential Equationsaaa1235No ratings yet
- Pin Mux Utility For ARM MPU Processors - Texas Instruments WikiDocument24 pagesPin Mux Utility For ARM MPU Processors - Texas Instruments WikiKuldeep KushwahaNo ratings yet