Download as pdf or txt
You might also like
- Letter of Intent (LOI) TemplateDocument1 pageLetter of Intent (LOI) Templatesmvhora100% (1)
- Breast Cancer Missed at Screening Hindsight or MiDocument6 pagesBreast Cancer Missed at Screening Hindsight or MideaNo ratings yet
- Screening Breast MRI in Patients Previously Treated For Breast CancerDocument7 pagesScreening Breast MRI in Patients Previously Treated For Breast CancerkhadijawhasNo ratings yet
- 10.1148 Radiol.212873Document12 pages10.1148 Radiol.212873RonWuNo ratings yet
- Contrast Enhancement in Breast Cancer and Background Mammary-Gland Tissue During The Super-Early Phase of Dynamic Breast Magnetic Resonance ImagingDocument7 pagesContrast Enhancement in Breast Cancer and Background Mammary-Gland Tissue During The Super-Early Phase of Dynamic Breast Magnetic Resonance ImagingBenitaNo ratings yet
- Knut Tel 2014Document6 pagesKnut Tel 2014IridaeNo ratings yet
- RM Menores de 35 Años Con CA de MamaDocument7 pagesRM Menores de 35 Años Con CA de MamaAzucena BCNo ratings yet
- (Review) Comparison of The Clinical Application Value of Mo-Targeted X-Ray, Color Doppler Ultrasound and MRI in Preoperative Comprehensive Evaluation of Breast CancerDocument5 pages(Review) Comparison of The Clinical Application Value of Mo-Targeted X-Ray, Color Doppler Ultrasound and MRI in Preoperative Comprehensive Evaluation of Breast Cancer최윤No ratings yet
- BreastDocument14 pagesBreastAnitei GabrielaNo ratings yet
- Omidiji 2017Document7 pagesOmidiji 2017Dewa OkaNo ratings yet
- Case-Control Study of Mammographic Density and Breast Cancer Risk Using Processed Digital MammogramsDocument4 pagesCase-Control Study of Mammographic Density and Breast Cancer Risk Using Processed Digital MammogramsEmasHarnasAkbarNo ratings yet
- MedicineDocument6 pagesMedicineJEAN CARLOS GALLO VALVERDENo ratings yet
- Breast CA ScreeningDocument8 pagesBreast CA Screeningchristelm_1No ratings yet
- MammogrpahyDocument11 pagesMammogrpahyferolonoNo ratings yet
- Image Features of True Positive and False Negative Cancers in Screening MammogramsDocument9 pagesImage Features of True Positive and False Negative Cancers in Screening MammogramsTher RayNo ratings yet
- Potential Impact of Tomosynthesis On The Detection and Diagnosis of Breast LesionsDocument11 pagesPotential Impact of Tomosynthesis On The Detection and Diagnosis of Breast LesionsMR Emam - GamingNo ratings yet
- Four Risk of Malignancy Indices in Evaluation of Pelvic MassesDocument8 pagesFour Risk of Malignancy Indices in Evaluation of Pelvic MassesherryNo ratings yet
- Optical Imaging InbreastsDocument11 pagesOptical Imaging InbreastsCezara RasinarNo ratings yet
- Impact of Breast Cancer Subtypes On Prognosis of Women With Operable Invasive Breast Cancer: A Population-Based Study Using SEER DatabaseDocument10 pagesImpact of Breast Cancer Subtypes On Prognosis of Women With Operable Invasive Breast Cancer: A Population-Based Study Using SEER DatabasesilviatengkerNo ratings yet
- Curroncol 29 00159 v2Document20 pagesCurroncol 29 00159 v2rachid oumouloudNo ratings yet
- Association of 18F-FDG-PET SUV and Tumor Size in Cervical CancerDocument1 pageAssociation of 18F-FDG-PET SUV and Tumor Size in Cervical CancerRomildo da SilvaNo ratings yet
- Role of Computed Tomography (CT) Scan in Staging of Cervical CarcinomaDocument6 pagesRole of Computed Tomography (CT) Scan in Staging of Cervical CarcinomaTriponiaNo ratings yet
- European Journal of Radiology: Research ArticleDocument4 pagesEuropean Journal of Radiology: Research ArticlekhadijawhasNo ratings yet
- Trends in Delayed Breast Cancer Diagnosis After ReDocument9 pagesTrends in Delayed Breast Cancer Diagnosis After ReeugeniaNo ratings yet
- Simple Ultrasound Rules To Distinguish Between Benign and Malignant Adnexal Masses Before Surgery: Prospective Validation by IOTA GroupDocument16 pagesSimple Ultrasound Rules To Distinguish Between Benign and Malignant Adnexal Masses Before Surgery: Prospective Validation by IOTA GroupherryNo ratings yet
- JURNAL RadiologiDocument16 pagesJURNAL RadiologiBintang Saputra PilliangNo ratings yet
- 3-1 Can Artificial Intelligence Reduce The Interval Cancer RateDocument8 pages3-1 Can Artificial Intelligence Reduce The Interval Cancer Rate14mervekaya01No ratings yet
- Comparative Effectiveness of Digital Breast Tomosynthesis For Breast Cancer Screening Among Women 40-64 Years OldDocument8 pagesComparative Effectiveness of Digital Breast Tomosynthesis For Breast Cancer Screening Among Women 40-64 Years OldAmalia fhyNo ratings yet
- Rycan 2021210036Document7 pagesRycan 2021210036Imagenologia Hospital de ClinicasNo ratings yet
- 10.1186 - s13058 017 0846 1Document14 pages10.1186 - s13058 017 0846 1Ober Van Gómez LópezNo ratings yet
- Current and Future Use of Radiological Images in The Management of Gynecological Malignancies - A Survey of Practice in The UKDocument21 pagesCurrent and Future Use of Radiological Images in The Management of Gynecological Malignancies - A Survey of Practice in The UKKrishna PanduNo ratings yet
- Cervical Cancer Diagnostics Healthcare System Using Hybrid Object Detection Adversarial NetworksDocument10 pagesCervical Cancer Diagnostics Healthcare System Using Hybrid Object Detection Adversarial Networkskeerthana samalaNo ratings yet
- Editorial: Molecular Imaging in Breast CancerDocument4 pagesEditorial: Molecular Imaging in Breast CancerKurnia AlkatiriNo ratings yet
- Ca MamaDocument5 pagesCa MamaAlberto MonroyNo ratings yet
- Tamizaje Ecográfico CombinadoDocument12 pagesTamizaje Ecográfico CombinadoLuis Cesar Amador SalgadoNo ratings yet
- Indications For Breast MRI: Case-Based Review: ObjectiveDocument14 pagesIndications For Breast MRI: Case-Based Review: ObjectiveFandie PratamaNo ratings yet
- Ultrasound Imaging Technologies For: Version of RecordDocument76 pagesUltrasound Imaging Technologies For: Version of Recordmaha88eceNo ratings yet
- Downgrading of Breast Massess by Optoacoustic ImaginDocument11 pagesDowngrading of Breast Massess by Optoacoustic ImaginChadiIbrahimNo ratings yet
- Cancer de MamaDocument11 pagesCancer de MamaIng SánchezNo ratings yet
- Breast Tomosynthesis in Clinical PracticeDocument9 pagesBreast Tomosynthesis in Clinical PracticedeadcorpsesNo ratings yet
- Papaer Prueba 2Document9 pagesPapaer Prueba 2Joselyn CastroNo ratings yet
- Diagnosis of Breast Tumours and Evaluation of Prognostic Risk by Using Machine Learning ApproachesDocument11 pagesDiagnosis of Breast Tumours and Evaluation of Prognostic Risk by Using Machine Learning ApproachesPhạm Quốc DưNo ratings yet
- Gareth 2014Document10 pagesGareth 2014marizal saputraNo ratings yet
- Comparison of Ultrasound and Mammography For Early DiagnosisDocument8 pagesComparison of Ultrasound and Mammography For Early Diagnosishdh1224No ratings yet
- Angiosarcoma MamaDocument5 pagesAngiosarcoma MamaRaul Matute MartinNo ratings yet
- Probabilistic Neural Network For Breast Cancer Classification - SpringerLinkDocument31 pagesProbabilistic Neural Network For Breast Cancer Classification - SpringerLinkberline djimeliNo ratings yet
- Mri - Best Practice - Bisi - 2020 PDFDocument7 pagesMri - Best Practice - Bisi - 2020 PDFBISI IndiaNo ratings yet
- Applsci 10 00767 v3Document30 pagesApplsci 10 00767 v3meneeeeeNo ratings yet
- IOTA, ADNEX and ORADSDocument9 pagesIOTA, ADNEX and ORADSzaaaidaNo ratings yet
- Automated Segmentation of Endometrial Cancer On MR Images Using Deep LearningDocument8 pagesAutomated Segmentation of Endometrial Cancer On MR Images Using Deep LearningKeerthana RobertNo ratings yet
- MRI Criteria For The Diagnosis of Pleomorphic Adenoma: A Validation StudyDocument6 pagesMRI Criteria For The Diagnosis of Pleomorphic Adenoma: A Validation Studysarah iriamanaNo ratings yet
- 10 1016@j Ejso 2020 03 188Document1 page10 1016@j Ejso 2020 03 188Andrіі DudashNo ratings yet
- A Deep Learning Mammography-Based Model For Improved Breast Cancer Risk PredictionDocument7 pagesA Deep Learning Mammography-Based Model For Improved Breast Cancer Risk PredictionFelipe ScolariNo ratings yet
- Thesis Protocol Final SarangDocument26 pagesThesis Protocol Final SarangRaj KotichaNo ratings yet
- Peprah 2018Document7 pagesPeprah 2018Dewa OkaNo ratings yet
- Application of Computer-Aided Diagnosis On Breast UltrasonographyDocument8 pagesApplication of Computer-Aided Diagnosis On Breast UltrasonographySummrina KanwalNo ratings yet
- Incidental Primary Breast Cancer Detected On PET-CTDocument8 pagesIncidental Primary Breast Cancer Detected On PET-CTMaxime PorcoNo ratings yet
- 1 s2.0 S0360301609016228Document2 pages1 s2.0 S0360301609016228andresNo ratings yet
- Multiparametric Ultrasound Diagnosis of Breast DiseasesFrom EverandMultiparametric Ultrasound Diagnosis of Breast DiseasesGennady T. SukhikhNo ratings yet
- Contrast-Enhanced MammographyFrom EverandContrast-Enhanced MammographyMarc LobbesNo ratings yet
- What Causes Iron-Deficiency Anemia?Document2 pagesWhat Causes Iron-Deficiency Anemia?AidaDesNo ratings yet
- Journal of Attention Disorders: Executive Function Impairments in High IQ Adults With ADHDDocument8 pagesJournal of Attention Disorders: Executive Function Impairments in High IQ Adults With ADHDLauren SerafiniNo ratings yet
- Example ResumeDocument1 pageExample Resumeduythuc_lqdNo ratings yet
- Assignment in PharmacologyDocument3 pagesAssignment in PharmacologyAlrick AsentistaNo ratings yet
- 1.pfizer Documents Reveal at Least 800 People Never Finished The COVID Vaccine Trial Due To Death, Injury or Withdrawn Consent - The ExposeDocument15 pages1.pfizer Documents Reveal at Least 800 People Never Finished The COVID Vaccine Trial Due To Death, Injury or Withdrawn Consent - The ExposeElvaNo ratings yet
- Hydrogr: Business Plan ReportDocument36 pagesHydrogr: Business Plan ReportJustEshads TvNo ratings yet
- Nihms 1028044Document18 pagesNihms 1028044NormanNo ratings yet
- Course Hero 1Document8 pagesCourse Hero 1sekhon.rajdeep27No ratings yet
- Safety Data Sheet Glass CleanerDocument25 pagesSafety Data Sheet Glass CleanerHewa PCNo ratings yet
- Drug Abuse: Short-Term EffectsDocument2 pagesDrug Abuse: Short-Term EffectsYeonjin ChoiNo ratings yet
- Gifted Child Quarterly: Myth 17: Gifted and Talented Individuals Do Not Have Unique Social and Emotional NeedsDocument4 pagesGifted Child Quarterly: Myth 17: Gifted and Talented Individuals Do Not Have Unique Social and Emotional NeedsChristianne do Rocio Storrer de OliveiraNo ratings yet
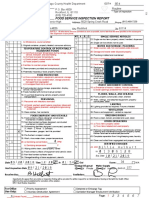
- Winnebago County Health Department, Food Service Inspection Report, Guilford High SchoolDocument7 pagesWinnebago County Health Department, Food Service Inspection Report, Guilford High Schoolcorina curryNo ratings yet
- Unit 18 Housing NeedDocument13 pagesUnit 18 Housing NeedhumaNo ratings yet
- Do 53-03Document6 pagesDo 53-03mefav7778520No ratings yet
- Neck and Trapezius Rehab PlanDocument15 pagesNeck and Trapezius Rehab PlanAnshika RanaNo ratings yet
- Nursing ShortageDocument16 pagesNursing Shortageapi-240927368No ratings yet
- Hospital Training ReportDocument27 pagesHospital Training ReportAdnan RAHAT50% (2)
- Community ProjectDocument10 pagesCommunity Projectapi-701329423No ratings yet
- (Perioperative Nursing Clinics 5 No. 3.) Goodman, Terri - Sterilization and Disinfection For The Perioperative Nurse (2010, Saunders) PDFDocument148 pages(Perioperative Nursing Clinics 5 No. 3.) Goodman, Terri - Sterilization and Disinfection For The Perioperative Nurse (2010, Saunders) PDFGokul SivaNo ratings yet
- Roberto Padlan (Resume)Document5 pagesRoberto Padlan (Resume)Merian PadlanNo ratings yet
- Enema PDFDocument2 pagesEnema PDFSandy Jusi100% (1)
- Academic Essay For Brighton University.Document4 pagesAcademic Essay For Brighton University.omelle AbubakarNo ratings yet
- Let Personnel TransferDocument12 pagesLet Personnel TransferKulveer YadavNo ratings yet
- Efektifitas Pemberian Jus Jambi Terhadap Kadar Hemoglobin Ibu Hamil Trimester Ii Dengan AnemiaDocument8 pagesEfektifitas Pemberian Jus Jambi Terhadap Kadar Hemoglobin Ibu Hamil Trimester Ii Dengan Anemiasiti rahayuNo ratings yet
- Personalized Medicine of Monoclonal Antibodies in in Ammatory Bowel Disease: Pharmacogenetics, Therapeutic Drug Monitoring, and BeyondDocument15 pagesPersonalized Medicine of Monoclonal Antibodies in in Ammatory Bowel Disease: Pharmacogenetics, Therapeutic Drug Monitoring, and BeyondJessica Asitimbay ZuritaNo ratings yet
- First Virtual Autopsy in Saudi ArabiaDocument5 pagesFirst Virtual Autopsy in Saudi ArabiaNatasyaNo ratings yet
- BiaDocument7 pagesBiaDian WijayantiNo ratings yet
- Project Paper On HR Practices in AB Bank LTDDocument97 pagesProject Paper On HR Practices in AB Bank LTDAshik Khan67% (3)
- Assessment Nursing Diagnosis Goal Planning Implementation Rationale EvaluationDocument2 pagesAssessment Nursing Diagnosis Goal Planning Implementation Rationale EvaluationRenju ThapaNo ratings yet