Download as pdf or txt
You might also like
- Blumgart's Surgery of The Liver, Biliary Tract, and Pancreas 6ed 2017 2vols 2401pag PDFDocument2,401 pagesBlumgart's Surgery of The Liver, Biliary Tract, and Pancreas 6ed 2017 2vols 2401pag PDFLucia Maria De Castro Mendes94% (32)
- New Vet Jumpstart Guide: Twenty common general practice cases simplifiedFrom EverandNew Vet Jumpstart Guide: Twenty common general practice cases simplifiedNo ratings yet
- Pharmacy Calculation Workbook: 250 Questions to Prepare for the NAPLEX and PTCB ExamFrom EverandPharmacy Calculation Workbook: 250 Questions to Prepare for the NAPLEX and PTCB ExamRating: 5 out of 5 stars5/5 (2)
- Paediatric Dosage of Some DrugsDocument46 pagesPaediatric Dosage of Some DrugsS S LNo ratings yet
- Pediatrics Drug Doses - DocToon PDFDocument49 pagesPediatrics Drug Doses - DocToon PDFBharat Jamod100% (1)
- Intern's Lecture On Pediatric Computation of MedicationsDocument26 pagesIntern's Lecture On Pediatric Computation of MedicationsTrish SantosidadNo ratings yet
- PedoDocument2 pagesPedoHenyo AkoNo ratings yet
- MisoprostolDocument2 pagesMisoprostolElvira Anita100% (2)
- Misoprostol Wheel 2017 ENDocument3 pagesMisoprostol Wheel 2017 ENMirahAvishaNo ratings yet
- Doses of Misoprostol Use Updated March 2018 PDFDocument2 pagesDoses of Misoprostol Use Updated March 2018 PDFDrFarah Emad AliNo ratings yet
- Dosage Guidelines MISOPROSTOLDocument4 pagesDosage Guidelines MISOPROSTOLIka FaoziawatiNo ratings yet
- Misoprostole in ObstetricsDocument11 pagesMisoprostole in ObstetricsDr-Saja O. DmourNo ratings yet
- Dosage Guidelines: Misoprostol in Obstetrics and GynaecologyDocument1 pageDosage Guidelines: Misoprostol in Obstetrics and GynaecologyFlorantia Setya NugrohoNo ratings yet
- Uso de Miso en Obstetricia Ipas Mexico PDFDocument39 pagesUso de Miso en Obstetricia Ipas Mexico PDFthedNo ratings yet
- Misoprostol Dosage Recommendations 2012 4Document1 pageMisoprostol Dosage Recommendations 2012 4Bonifacius Bayu Erlangga KusumaNo ratings yet
- Misoprostol Dosages For Reproductive HealthDocument1 pageMisoprostol Dosages For Reproductive HealthAnonymous b6xAErNo ratings yet
- Recommended Dosages: 1st Trimester 2nd Trimester 3rd Trimester PostpartumDocument1 pageRecommended Dosages: 1st Trimester 2nd Trimester 3rd Trimester PostpartumPutri Octavia SariNo ratings yet
- Empiric Antibiotic Treatment of Urinary Tract InfectionsDocument3 pagesEmpiric Antibiotic Treatment of Urinary Tract InfectionsVikas KumarNo ratings yet
- FIGO MifeMiso Chart 11 2023 FINALDocument1 pageFIGO MifeMiso Chart 11 2023 FINALmohammedyosif76No ratings yet
- FIGO MifeMiso Chart 11 2023 FINAL - 0Document1 pageFIGO MifeMiso Chart 11 2023 FINAL - 0Henzor Hezron WahgwaanNo ratings yet
- Mifepristone & Misoprostol Dosing Chart 2023Document1 pageMifepristone & Misoprostol Dosing Chart 2023Iriawan Indra PutraNo ratings yet
- Endometrial Preparation For FET: DR Astha Gupta, Fellow in Reproductive Medicine, IHRDocument65 pagesEndometrial Preparation For FET: DR Astha Gupta, Fellow in Reproductive Medicine, IHRDrAstha Gupta100% (1)
- Ivf: Therapeutics: Anti-Pyretics: PenicillinsDocument6 pagesIvf: Therapeutics: Anti-Pyretics: PenicillinsJenny CiNo ratings yet
- FormularyDocument5 pagesFormularyMichelle WongNo ratings yet
- Endometrialcarcinoma r0416 7941Document2 pagesEndometrialcarcinoma r0416 7941crisibarra911No ratings yet
- Picu NotesDocument65 pagesPicu NotesAhmed Mohammed100% (2)
- Misoprostol FigoDocument1 pageMisoprostol FigoBenyamin Rakhmatsyah TitaleyNo ratings yet
- FormulaDocument5 pagesFormulaEloiseBalasbasNo ratings yet
- Fabella NotesDocument96 pagesFabella NotesAndrassy Twinkle Alinea100% (1)
- Pediatric DosagesDocument6 pagesPediatric Dosagesfelisareyes28No ratings yet
- 1 PBDocument6 pages1 PBDouglas SabinoNo ratings yet
- Obstetrics and Gynecology Intern HandbookDocument23 pagesObstetrics and Gynecology Intern HandbookMonna PaaktachaayNo ratings yet
- RebperDocument6 pagesRebperrosci563No ratings yet
- (REVISED) - Pre-Assignment - Klarissa Salma Raesita - 21640 - 6 IUPDocument11 pages(REVISED) - Pre-Assignment - Klarissa Salma Raesita - 21640 - 6 IUPKLARISSA SALMA R RNo ratings yet
- جرعات الاطفالDocument50 pagesجرعات الاطفالWael Hamdy100% (1)
- 1 s2.0 S0163445316300123 MainDocument2 pages1 s2.0 S0163445316300123 MainZara SaeedNo ratings yet
- Treatment of Canine Pyometra With The Gonadotropin-Releasing Hormone Antagonist Acyline: A Case SeriesDocument3 pagesTreatment of Canine Pyometra With The Gonadotropin-Releasing Hormone Antagonist Acyline: A Case SeriesValentina PimentelNo ratings yet
- Management of Convulsion in PaediatricsDocument21 pagesManagement of Convulsion in PaediatricsjuwelukgNo ratings yet
- Pedia Er Cheat SheetDocument2 pagesPedia Er Cheat SheetHarissa Katrina De LaraNo ratings yet
- Lung Cancer Treatment Regimens (Part 1 of 4)Document4 pagesLung Cancer Treatment Regimens (Part 1 of 4)Rubana Reaz TanaNo ratings yet
- National Malaria Drug PolicyDocument22 pagesNational Malaria Drug Policydocsaurabh777No ratings yet
- Red Book Abx Dosing 2021Document22 pagesRed Book Abx Dosing 2021reham ONo ratings yet
- Malaria Treatment TableDocument9 pagesMalaria Treatment Tableاحمد عرفاتNo ratings yet
- Endometrial Hyperplasia With Secretory ChangesDocument8 pagesEndometrial Hyperplasia With Secretory ChangesEloizaNo ratings yet
- OHSS Case Presentation Discussion - Jindal IVF CHDDocument41 pagesOHSS Case Presentation Discussion - Jindal IVF CHDJindal IVF ChandigarhNo ratings yet
- DR / Osama Ahmed: Contact UsDocument20 pagesDR / Osama Ahmed: Contact UsAhmed AliNo ratings yet
- Bovine Embryo TransferDocument34 pagesBovine Embryo TransferItzel MorenoNo ratings yet
- Regimen Revisions Due July 2022Document4 pagesRegimen Revisions Due July 2022Lucia FNo ratings yet
- Empiric Antibiotic Guidelines For Paediatric Intensive Care Unit (PICU)Document7 pagesEmpiric Antibiotic Guidelines For Paediatric Intensive Care Unit (PICU)Benny Chris TantoNo ratings yet
- LYRICE ProtocolDocument6 pagesLYRICE ProtocolInas UthmanNo ratings yet
- Essenc I Al TherapyDocument9 pagesEssenc I Al TherapyFabian Ramirez HincapiéNo ratings yet
- Denumire Cod Pret/buc Doza/animalDocument2 pagesDenumire Cod Pret/buc Doza/animalIacob IoanaNo ratings yet
- Malaria Treatment Table 202306Document10 pagesMalaria Treatment Table 202306Anam QadeerNo ratings yet
- MODULE 3 STANDARDIZE PATIENT - INTRAPARTUM StudentsDocument7 pagesMODULE 3 STANDARDIZE PATIENT - INTRAPARTUM StudentsalliahjaneadlawanNo ratings yet
- DOZE Animale de Companie PDFDocument12 pagesDOZE Animale de Companie PDFgabyNo ratings yet
- Menstrual Cycle Related Disorders: Volume 7: Frontiers in Gynecological EndocrinologyFrom EverandMenstrual Cycle Related Disorders: Volume 7: Frontiers in Gynecological EndocrinologySarah L. BergaNo ratings yet
- Physiology for General Surgical Sciences Examination (GSSE)From EverandPhysiology for General Surgical Sciences Examination (GSSE)S. Ali MirjaliliNo ratings yet
- Somatic Embryogenesis for Micropropagation of Coconut (Cocos nucifera L.)From EverandSomatic Embryogenesis for Micropropagation of Coconut (Cocos nucifera L.)No ratings yet
- New Assessment of Fetal Descent and Forceps DeliveryFrom EverandNew Assessment of Fetal Descent and Forceps DeliverySatoru TakedaNo ratings yet
- Progesterona La Hormona Definitiva del Bienestar FemeninoFrom EverandProgesterona La Hormona Definitiva del Bienestar FemeninoRating: 1 out of 5 stars1/5 (1)
- 09 JCR 009 Tandon Phenytoin ReportDocument3 pages09 JCR 009 Tandon Phenytoin ReportRosi IndahNo ratings yet
- Radiolucent Pulmonary Lesions: An Update and Diagnostic ProblemsDocument52 pagesRadiolucent Pulmonary Lesions: An Update and Diagnostic ProblemsRosi IndahNo ratings yet
- Materi Kuliah - Introduction To EBMDocument40 pagesMateri Kuliah - Introduction To EBMRosi IndahNo ratings yet
- Height in Chronic Kidney DiseaseDocument3 pagesHeight in Chronic Kidney DiseaseRosi IndahNo ratings yet
- DailyPlanner V2Document2 pagesDailyPlanner V2Rosi IndahNo ratings yet
- NCP Kenezo, Female 17Document2 pagesNCP Kenezo, Female 17labanesstephanyNo ratings yet
- Music Intervention For Pain and AnxietyDocument37 pagesMusic Intervention For Pain and AnxietyVebryana RamadhaniaNo ratings yet
- Betty Neuman: The System ModelDocument32 pagesBetty Neuman: The System ModelVincent PolicarNo ratings yet
- New Utilisation of Herbals and Their Formulations in Natural Drug TreatmentDocument74 pagesNew Utilisation of Herbals and Their Formulations in Natural Drug TreatmentanburajjNo ratings yet
- Provisional State Merit ListDocument101 pagesProvisional State Merit Listimran khanNo ratings yet
- ICM Essential Competencies For Basic Midwifery Practice 2010, Revised 2013 PDFDocument19 pagesICM Essential Competencies For Basic Midwifery Practice 2010, Revised 2013 PDFKuurniiaa PraweestiiNo ratings yet
- Cheryl Ann Stohler CV by JdsDocument3 pagesCheryl Ann Stohler CV by Jdsapi-236756953No ratings yet
- PDF Midwifery Final Test 1Document7 pagesPDF Midwifery Final Test 1DianeNo ratings yet
- FM 4-02.1Document158 pagesFM 4-02.1"Rufus"No ratings yet
- C9ECh2 People As Resource PDFDocument19 pagesC9ECh2 People As Resource PDFPieNo ratings yet
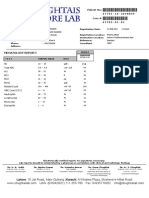
- ReportViewer3 CBCDocument1 pageReportViewer3 CBCMuhammad Munawar BuzdarNo ratings yet
- First Step To Achieve Your Objective - GomezDocument8 pagesFirst Step To Achieve Your Objective - GomezNicole Ivy GorimoNo ratings yet
- Nurse Notes OutlineDocument1 pageNurse Notes OutlineFaye G.No ratings yet
- Câu Hỏi Ôn Tập: (Các lớp Cao đẳng Dược)Document12 pagesCâu Hỏi Ôn Tập: (Các lớp Cao đẳng Dược)Di ThiênNo ratings yet
- EPI Lecture1Document43 pagesEPI Lecture1SoloNo ratings yet
- Indian Health Care System-Weaknesses, Schemes and The Way AheadDocument16 pagesIndian Health Care System-Weaknesses, Schemes and The Way AheadGaurav Prabhaker0% (1)
- Nursing Experience PDFDocument2 pagesNursing Experience PDFCadiffNo ratings yet
- Hailey Gilbreath Resume 07-23-2020Document1 pageHailey Gilbreath Resume 07-23-2020api-534716659No ratings yet
- SABA Reliance Questionnaire (SRQ) FulltextDocument34 pagesSABA Reliance Questionnaire (SRQ) FulltextPhụng KimNo ratings yet
- Trade and Health:: Towards Building A National StrategyDocument149 pagesTrade and Health:: Towards Building A National Strategymanjusri lalNo ratings yet
- Basic DefinitionDocument7 pagesBasic Definitionsamiurrehman4994No ratings yet
- BHCMS Barangay Health Center ManagementDocument39 pagesBHCMS Barangay Health Center Managementjoyce manangat100% (1)
- Levy Mwanawasa Medical University School of Public Health and Environmental Sciences Department of Public HealthDocument5 pagesLevy Mwanawasa Medical University School of Public Health and Environmental Sciences Department of Public HealthChristían KanyataNo ratings yet
- Physical, Leisure, and Daily Living Activities In.3Document11 pagesPhysical, Leisure, and Daily Living Activities In.3yogithajeganathan5197No ratings yet
- Narrative Report. Ate DaleDocument2 pagesNarrative Report. Ate DaleKryza Dale Bunado Batican89% (9)
- CHN PPT PrelimDocument101 pagesCHN PPT PrelimgmatbdotsNo ratings yet
- In Patient Satisfaction Survey-How Does It Help Our Health Care Delivery System (The Patient, The Health Care Giver and The Organization) ?Document10 pagesIn Patient Satisfaction Survey-How Does It Help Our Health Care Delivery System (The Patient, The Health Care Giver and The Organization) ?Pallavi PalluNo ratings yet
- Bronne Lo TaakDocument3 pagesBronne Lo TaakLuhan ErweeNo ratings yet
- Ageing Population Geography Case StudyDocument3 pagesAgeing Population Geography Case StudynosheenNo ratings yet