Download as docx, pdf, or txt
You might also like
- (Merrill Counseling) Patricia Stevens, Robert L. Smith - Substance Abuse Counseling - Theory and Practice-Pearson (2012) PDFDocument379 pages(Merrill Counseling) Patricia Stevens, Robert L. Smith - Substance Abuse Counseling - Theory and Practice-Pearson (2012) PDFaisyahwanzauki89% (9)
- Therapeutic Community - Present. Past. and Moving ForwardDocument12 pagesTherapeutic Community - Present. Past. and Moving ForwardChristine Acis0% (2)
- SMA07-4154 Clients Handbook MatrixDocument114 pagesSMA07-4154 Clients Handbook MatrixGerald Dawson100% (1)
- Essay On The Drug AbuseDocument3 pagesEssay On The Drug Abusejasbirldh86100% (3)
- Chapter 005Document4 pagesChapter 005Natalia Page TrevinoNo ratings yet
- Chapter - 011 Study NotesDocument5 pagesChapter - 011 Study Notesborisdevic223No ratings yet
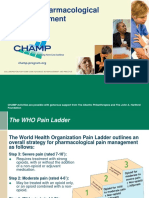
- Pain Management For ElderlyDocument14 pagesPain Management For ElderlyandikaisnaeniNo ratings yet
- Alleviating Cancer PainDocument9 pagesAlleviating Cancer PainSuresh KumarNo ratings yet
- Cu7 - Pain 1Document18 pagesCu7 - Pain 1FERMIL PASGALANo ratings yet
- Cancer Pain: A Husni TanraDocument51 pagesCancer Pain: A Husni TanraNur Farmawati Humayrah HassaniNo ratings yet
- Pain Management (Also Called Pain Medicine or Algiatry) Is A Branch of Medicine Employing AnDocument5 pagesPain Management (Also Called Pain Medicine or Algiatry) Is A Branch of Medicine Employing AnChristine QuironaNo ratings yet
- Management of PainDocument6 pagesManagement of PainSinging MedicNo ratings yet
- Cancer Pain ManagementDocument58 pagesCancer Pain ManagementReyza HasnyNo ratings yet
- NRR 36876 Tramadol Paracetamol Fixed Dose Combination in The Frontline 020113Document14 pagesNRR 36876 Tramadol Paracetamol Fixed Dose Combination in The Frontline 020113Intan KencanaNo ratings yet
- Pain Evaluation and MeasurementDocument7 pagesPain Evaluation and MeasurementUnnikrishnan VsNo ratings yet
- Lecture 8-Principles of Drug Use in Palliativ EcareDocument6 pagesLecture 8-Principles of Drug Use in Palliativ EcareMachukiNo ratings yet
- AnalgesicsDocument2 pagesAnalgesicsDhaval DudhatNo ratings yet
- Understanding of Usage of Painkillers in The Management of Terminal Cancer PatientDocument6 pagesUnderstanding of Usage of Painkillers in The Management of Terminal Cancer PatientGunners CoolNo ratings yet
- Migraines: Migraine Treatment and Prevention Options: The most important information you need to improve your healthFrom EverandMigraines: Migraine Treatment and Prevention Options: The most important information you need to improve your healthNo ratings yet
- QPostHerpeticNeauralgia NSinghDocument3 pagesQPostHerpeticNeauralgia NSinghDevi DamayantiNo ratings yet
- AIN Anagement: Christine K. O'NeilDocument14 pagesAIN Anagement: Christine K. O'NeilbencleeseNo ratings yet
- PCEP-PC Module 4 (Pain) NotesDocument12 pagesPCEP-PC Module 4 (Pain) NotesMan MedNo ratings yet
- Pain Management Research PaperDocument6 pagesPain Management Research Paperafnhbijlzdufjj100% (1)
- SIM For Palliative Care For Cancer PatientsDocument9 pagesSIM For Palliative Care For Cancer PatientsJasdeep KaurNo ratings yet
- Acspc 046379Document84 pagesAcspc 046379Екатерина КостюкNo ratings yet
- Tugas Terjemahan-Manajemen NyeriDocument50 pagesTugas Terjemahan-Manajemen NyeriNur MuawanaNo ratings yet
- Pain Relief Medications - OTC, Prescription & Side EffectsDocument9 pagesPain Relief Medications - OTC, Prescription & Side EffectsPratick DasNo ratings yet
- Opioid and Pain Management Final PaperDocument10 pagesOpioid and Pain Management Final Paperapi-318123395No ratings yet
- Mahfudh 2011Document3 pagesMahfudh 2011Azhari BaedlawiNo ratings yet
- Br. J. Anaesth.-2013-Fallon-105-11Document7 pagesBr. J. Anaesth.-2013-Fallon-105-11Tito Haposan TobingNo ratings yet
- 8 Chronic Pain ManagementDocument14 pages8 Chronic Pain ManagementEndang Dwi KurniaNo ratings yet
- The Role of Opioid in Cancer Pain ManagementDocument36 pagesThe Role of Opioid in Cancer Pain ManagementYipno Wanhar El MawardiNo ratings yet
- Pain Management For Medical StudentsDocument37 pagesPain Management For Medical Studentsamq aloqiliNo ratings yet
- 4058 PainSlidesDocument73 pages4058 PainSlidesSteven GodelmanNo ratings yet
- Pain ManagementDocument13 pagesPain ManagementusmanNo ratings yet
- Why Cancer PainDocument15 pagesWhy Cancer Paintitian rachmawatiNo ratings yet
- Assessment Task 1: Topic 3 - Cancer PainDocument8 pagesAssessment Task 1: Topic 3 - Cancer Painsween64No ratings yet
- Pain ManagementDocument24 pagesPain ManagementIbrahim DhouafliNo ratings yet
- PainDocument35 pagesPainixora n100% (1)
- Pain ManagementDocument67 pagesPain ManagementMohammad KhoderNo ratings yet
- Manejo Del Paciente Terminal: Lara Et Al, Cancerología 1 (2006) : 283-295Document13 pagesManejo Del Paciente Terminal: Lara Et Al, Cancerología 1 (2006) : 283-295Ivon Mendez DiazNo ratings yet
- Codeine Tips Pharmacy AssistantsDocument3 pagesCodeine Tips Pharmacy AssistantsSaraNo ratings yet
- Pain From Terminal IllnessDocument20 pagesPain From Terminal IllnessesyeehoNo ratings yet
- Management of Chronic Pain in The Elderly 2018Document8 pagesManagement of Chronic Pain in The Elderly 2018Dara Agusti MaulidyaNo ratings yet
- Asepsis ProceduresDocument23 pagesAsepsis ProceduresYashNo ratings yet
- DR - Muhammad Aasam Maan: Consultant Pain SpecialistDocument23 pagesDR - Muhammad Aasam Maan: Consultant Pain SpecialistMuhammad Aasim MaanNo ratings yet
- Review WHOPainLadder OpioidsandNonOpioidsDocument13 pagesReview WHOPainLadder OpioidsandNonOpioidsamajida fadia rNo ratings yet
- An Option Overview: Neuropathic PainDocument3 pagesAn Option Overview: Neuropathic PainAndi Tri SutrisnoNo ratings yet
- Acute Pain Management in Patients With Opioid ToleranceDocument6 pagesAcute Pain Management in Patients With Opioid ToleranceHendrikus Surya Adhi PutraNo ratings yet
- Pharmacological Management of Cancer-Related Pain: Photo Courtesy of Lisa Scholder. Solid Stance. 16" × 24"Document14 pagesPharmacological Management of Cancer-Related Pain: Photo Courtesy of Lisa Scholder. Solid Stance. 16" × 24"I Made AryanaNo ratings yet
- Chronic Pain NandaDocument7 pagesChronic Pain NandaJude Bello-AlvearNo ratings yet
- 2009 Pain Assessment and ManagementDocument22 pages2009 Pain Assessment and ManagementErnawa RikaNo ratings yet
- Importance of Opioid ToleranceDocument4 pagesImportance of Opioid ToleranceAdiAri RosiuNo ratings yet
- Adjuvant AnalgesicDocument14 pagesAdjuvant AnalgesicPradnya ParamitaNo ratings yet
- For The Clinician: Clinical Pharmacology Considerations in Pain Management in Patients With Advanced Kidney FailureDocument15 pagesFor The Clinician: Clinical Pharmacology Considerations in Pain Management in Patients With Advanced Kidney FailureflorcithaNo ratings yet
- Jurnal 2 Anes Dexa MedikaDocument4 pagesJurnal 2 Anes Dexa MedikaNurmawati At100% (1)
- 1TM Cancer Pain - Introduction & Principles 2012 (Trainer's Guide)Document39 pages1TM Cancer Pain - Introduction & Principles 2012 (Trainer's Guide)khairulfatinNo ratings yet
- Opiates TipsDocument39 pagesOpiates TipsroooNo ratings yet
- Pain ManagementDocument11 pagesPain Managementenam professorNo ratings yet
- Pain ManagementDocument40 pagesPain ManagementPutra Pratama100% (1)
- Kinard PPT Pain MGMNTDocument83 pagesKinard PPT Pain MGMNTDeddy WidjajaNo ratings yet
- I. ObjectiveDocument3 pagesI. ObjectiveisxyNo ratings yet
- Gov T Has Strong Case Vs Ongpin, ex-DBP Officials : Posted at 08/21/2011 7:49 PM - Updated As of 08/21/2011 7:49 PMDocument4 pagesGov T Has Strong Case Vs Ongpin, ex-DBP Officials : Posted at 08/21/2011 7:49 PM - Updated As of 08/21/2011 7:49 PMisxyNo ratings yet
- Clinical Evidence ConciseDocument4 pagesClinical Evidence ConciseisxyNo ratings yet
- Calculating Drip RateDocument7 pagesCalculating Drip RateisxyNo ratings yet
- Wednesday Thursday Friday Saturday Sunday Monday Tuesday: 7 Day's Diet RecallDocument7 pagesWednesday Thursday Friday Saturday Sunday Monday Tuesday: 7 Day's Diet RecallisxyNo ratings yet
- Problem Identification - Pure BlackDocument3 pagesProblem Identification - Pure BlackisxyNo ratings yet
- Drug AbuseDocument14 pagesDrug AbuseMandeep BatraNo ratings yet
- The Accidental AddictsDocument6 pagesThe Accidental AddictsnorthandsouthnzNo ratings yet
- Drug Addiction and Drug AbuseDocument23 pagesDrug Addiction and Drug Abuseannu panchalNo ratings yet
- Notes in DEVCDocument32 pagesNotes in DEVCEarl Jann LaurencioNo ratings yet
- Auricular AcupunctureDocument16 pagesAuricular AcupunctureRamiro GuerreroNo ratings yet
- Drug Enforcement Vice Control and Organized Week 4Document27 pagesDrug Enforcement Vice Control and Organized Week 4Enzo MacTavish SendohNo ratings yet
- Systematic Review SchizophreniaDocument79 pagesSystematic Review SchizophreniaJHWNo ratings yet
- EMS AddictionDocument8 pagesEMS AddictionEvi LykouNo ratings yet
- Relapse Prevention: Jayakrishnan Menon, Arun KandasamyDocument6 pagesRelapse Prevention: Jayakrishnan Menon, Arun KandasamyNorma FloresNo ratings yet
- Behavior Analysis and Substance DependenceDocument289 pagesBehavior Analysis and Substance DependenceDiana Lucia Useche DelgadoNo ratings yet
- House MD PDFDocument10 pagesHouse MD PDFMax1929No ratings yet
- Self-Development Groups Among Women in RecoveryDocument9 pagesSelf-Development Groups Among Women in RecoveryPaula FariaNo ratings yet
- Human Motivation 6th Edition Franken Test BankDocument22 pagesHuman Motivation 6th Edition Franken Test Bankhubertbak126100% (33)
- DOH DATRC IRR For R.A. 9165Document15 pagesDOH DATRC IRR For R.A. 9165Clark Edward Runes UyticoNo ratings yet
- Detailed Lesson Plan in Health For DemoDocument5 pagesDetailed Lesson Plan in Health For DemoloriemaecaracolNo ratings yet
- Opioids, Pain, and FearDocument3 pagesOpioids, Pain, and FearlucianaclarkNo ratings yet
- General Presentation - PSY 308Document38 pagesGeneral Presentation - PSY 308Oluwasegun OujemibolaNo ratings yet
- Alcohol Dependence SyndromeDocument3 pagesAlcohol Dependence SyndromeMohd AminuddinNo ratings yet
- HistoryDocument3 pagesHistorylorshie127No ratings yet
- Community As Treatment The Therapeutic Community Model in The Era of The Opioid Crisis 7F6rDocument5 pagesCommunity As Treatment The Therapeutic Community Model in The Era of The Opioid Crisis 7F6rSci TechnolNo ratings yet
- Cyber AddictionDocument35 pagesCyber AddictionWardinatul ImanNo ratings yet
- Opioid ComplaintDocument139 pagesOpioid ComplaintABC15 NewsNo ratings yet
- M.Mwaniki N493 6Document22 pagesM.Mwaniki N493 6berrick otienoNo ratings yet
- Case Study RossanizanDocument10 pagesCase Study RossanizanMohd Faizal Mat SaadNo ratings yet
- Drugs (IGCSE Biology)Document25 pagesDrugs (IGCSE Biology)Study Guy100% (2)
- Presentation4 DrugsDocument42 pagesPresentation4 DrugsAmy BCNo ratings yet