Download as pdf or txt
You might also like
- Principles and Guidelines For The Conduct of Microbiological Risk AssessmentDocument6 pagesPrinciples and Guidelines For The Conduct of Microbiological Risk Assessmentudomsri_iNo ratings yet
- Chemical Safety: Ayala BLVD., Ermita, Manila, 1000, PhilippinesDocument26 pagesChemical Safety: Ayala BLVD., Ermita, Manila, 1000, PhilippinesJersey Mae PerlasNo ratings yet
- Risk Assessment - CharacterizationDocument10 pagesRisk Assessment - CharacterizationKladees WorldNo ratings yet
- ToxicologyDocument1 pageToxicologyGuilianNo ratings yet
- PHM205 Lec 6Document3 pagesPHM205 Lec 6Russ WestNo ratings yet
- Seminar Exposure AssessmentDocument15 pagesSeminar Exposure AssessmentDevi SreeNo ratings yet
- EnvironmentalDocument7 pagesEnvironmentalSaud Al MutawaNo ratings yet
- Unit 6: Risk, Exposure, and Health: SectionsDocument33 pagesUnit 6: Risk, Exposure, and Health: Sectionsapi-286231291No ratings yet
- CAC - GL 30-1999 Principles and Guidelines For The Conduct of Microbiological Risk AssessmentDocument4 pagesCAC - GL 30-1999 Principles and Guidelines For The Conduct of Microbiological Risk AssessmenttruongnguyenphiNo ratings yet
- 01 3 Risk Assessment Env PolicyDocument5 pages01 3 Risk Assessment Env Policyyi liaoNo ratings yet
- Presentation On Risk Assessment and ManagementDocument30 pagesPresentation On Risk Assessment and ManagementNavotsana ShubhangiNo ratings yet
- Risk AssessmentDocument30 pagesRisk AssessmentHend maarofNo ratings yet
- Science of Risk AssessmentDocument4 pagesScience of Risk AssessmentDrBishnu Prasad MahalaNo ratings yet
- Figure 1: A Schematic Illustrating The Chemical Risk Assessment ProcessDocument10 pagesFigure 1: A Schematic Illustrating The Chemical Risk Assessment ProcessrexlloydNo ratings yet
- P I F C R M: ART Undamental Oncepts IN ISK AnagementDocument23 pagesP I F C R M: ART Undamental Oncepts IN ISK Anagementbaaziz2015No ratings yet
- Risk Perc NPDocument6 pagesRisk Perc NPDaniel VenablesNo ratings yet
- WK - 15 Risk AssessmentDocument28 pagesWK - 15 Risk AssessmentMuhammad JafarNo ratings yet
- Assignment 2Document6 pagesAssignment 2api-642452301No ratings yet
- Unit Title: Demonstrate Occupational Safety and Health Practices Unit Code: It/Os/Ict/Bc/07 SEMESTER 2 2021/2022 Lecturer: Ms. Esther MachariaDocument25 pagesUnit Title: Demonstrate Occupational Safety and Health Practices Unit Code: It/Os/Ict/Bc/07 SEMESTER 2 2021/2022 Lecturer: Ms. Esther MachariaJOEL JUMANo ratings yet
- Risk Analysis in Healthcare Organizations: Methodological Framework and Critical VariablesDocument15 pagesRisk Analysis in Healthcare Organizations: Methodological Framework and Critical VariablesIvan PavlovicNo ratings yet
- Challenges in Risk Assessment: Quantitative Risk Assessment: SciencedirectDocument8 pagesChallenges in Risk Assessment: Quantitative Risk Assessment: SciencedirectFikri ZoldakNo ratings yet
- Chapter 3pptxDocument42 pagesChapter 3pptxsinatra DNo ratings yet
- M5 Chapter2Document32 pagesM5 Chapter2jrpatel18853No ratings yet
- Report 5 Risk Assessment of ChemicalsDocument5 pagesReport 5 Risk Assessment of ChemicalsDee KlikNo ratings yet
- Lec 3 EraDocument18 pagesLec 3 Erag4goharNo ratings yet
- Unit V Safety & RiskDocument67 pagesUnit V Safety & Riskvicky0457No ratings yet
- Ecological RiskDocument14 pagesEcological RiskTmt TarekNo ratings yet
- 1Document40 pages1nguyenlekhanh.x02No ratings yet
- Risk Analysis: Assoc. Prof. Dr. John Tang Yew HuatDocument37 pagesRisk Analysis: Assoc. Prof. Dr. John Tang Yew HuatFarah GhazaliNo ratings yet
- THC Module 1 - Unit 1Document10 pagesTHC Module 1 - Unit 1Arthur AquinoNo ratings yet
- GE15 ULOeDocument5 pagesGE15 ULOeKyle Adrian MartinezNo ratings yet
- 3 - Environmental Risk Assessment - EPA ProceduresDocument19 pages3 - Environmental Risk Assessment - EPA Procedurestasniimm87No ratings yet
- SQRA Singapore PDFDocument48 pagesSQRA Singapore PDFroem1104No ratings yet
- Risk ManaGementDocument4 pagesRisk ManaGementBeverly RamosNo ratings yet
- Biosafety and Risk AssessmentDocument27 pagesBiosafety and Risk AssessmentDharlie Flean ParillaNo ratings yet
- SM Incinerators 4Document24 pagesSM Incinerators 4Pasindu PramodNo ratings yet
- Accessing and Minimizing The Risk From HazardsDocument2 pagesAccessing and Minimizing The Risk From HazardsSaad SarwarNo ratings yet
- Risk AssessmentDocument5 pagesRisk AssessmentValentin RadulescuNo ratings yet
- Env Audit - 2024Document27 pagesEnv Audit - 2024nuhel.nasifNo ratings yet
- Research Article: Subjective Risk Assessment and Perception in The Greek and English Bakery IndustriesDocument9 pagesResearch Article: Subjective Risk Assessment and Perception in The Greek and English Bakery IndustriesJoaquin SabaghNo ratings yet
- Greater Than Minimal RiskDocument2 pagesGreater Than Minimal RiskJheny Bee AgaloosNo ratings yet
- Health Risk Assessments: Opportunities and Pitfalls: Common Errors Relating To EnvironmentalDocument32 pagesHealth Risk Assessments: Opportunities and Pitfalls: Common Errors Relating To EnvironmentalOmar HeshamNo ratings yet
- Quantitative Health Risk Assessment - NSWPHB - 2003Document27 pagesQuantitative Health Risk Assessment - NSWPHB - 2003PublicHealthbyDesignNo ratings yet
- CFDA Cosmetic Safety Evaluation Guideline EnglishDocument40 pagesCFDA Cosmetic Safety Evaluation Guideline EnglishromicaNo ratings yet
- Public Health Risk Assessment - EhraDocument28 pagesPublic Health Risk Assessment - EhraElga Melani RohmawatiNo ratings yet
- Cosmetic Hazards Identification and Safety Risk Assessment-Xavier Couvignou PDFDocument35 pagesCosmetic Hazards Identification and Safety Risk Assessment-Xavier Couvignou PDFHendra SaputraNo ratings yet
- Week6 8Document5 pagesWeek6 8Roxan ReyesNo ratings yet
- Chemical Risk AssessmentDocument4 pagesChemical Risk Assessmentوائل مصطفىNo ratings yet
- Challenges in Risk Assessment: Quantitative Risk Assessment: SciencedirectDocument8 pagesChallenges in Risk Assessment: Quantitative Risk Assessment: SciencedirectOsman GünerNo ratings yet
- Risk Assessment in ToxicologyDocument5 pagesRisk Assessment in ToxicologysaberNo ratings yet
- DRM Fact Sheet Chemical SafetyDocument2 pagesDRM Fact Sheet Chemical SafetyalexcostelaNo ratings yet
- Risk Based Regulation of Pharmacy Full Draft RevisedDocument39 pagesRisk Based Regulation of Pharmacy Full Draft RevisedsehrNo ratings yet
- Risk Assessment: Elaine M. FaustmanDocument29 pagesRisk Assessment: Elaine M. FaustmanZHARICK DAYYANA GARZON ROANo ratings yet
- Envi Sci & Eng'g. Learning Material-Topic 5Document27 pagesEnvi Sci & Eng'g. Learning Material-Topic 5Janice C. PusposNo ratings yet
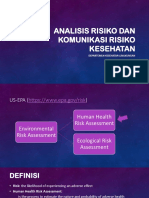
- KL-2 Analisis Risiko & Komunikasi Risiko Kesehatan - 2020Document31 pagesKL-2 Analisis Risiko & Komunikasi Risiko Kesehatan - 2020Reza DaraNo ratings yet
- CHAPTER4Document52 pagesCHAPTER4Seble GetachewNo ratings yet
- Risk AssessmentDocument62 pagesRisk Assessmentpia_shupaNo ratings yet
- Health Risk Assessment GuideDocument12 pagesHealth Risk Assessment GuideMuhammad syarifuddinNo ratings yet
- Brockville Risk Checklist 4 (Brc4): Scoring Manual: A Guide for Using a Forensic Risk Assessment ToolFrom EverandBrockville Risk Checklist 4 (Brc4): Scoring Manual: A Guide for Using a Forensic Risk Assessment ToolNo ratings yet
- Applications of Toxicogenomics in Safety Evaluation and Risk AssessmentFrom EverandApplications of Toxicogenomics in Safety Evaluation and Risk AssessmentDarrell R. BoverhofNo ratings yet
- Numericals in Chromatography PDFDocument25 pagesNumericals in Chromatography PDFrajbioNo ratings yet
- Tamil - HindiDocument261 pagesTamil - Hindirajbio100% (1)
- Surface Chemistry-1Document29 pagesSurface Chemistry-1rajbioNo ratings yet
- Evs Nov Dec 2014Document2 pagesEvs Nov Dec 2014rajbioNo ratings yet
- Instructions Faculty2017Document6 pagesInstructions Faculty2017rajbioNo ratings yet
- General KnowlwdgeDocument115 pagesGeneral KnowlwdgeMUDASSAR IDRIS98% (44)
- Background of The Study Example Research PaperDocument6 pagesBackground of The Study Example Research Paperqdvtairif100% (1)
- The Effect of Mind Map Technique On StudDocument5 pagesThe Effect of Mind Map Technique On StudRan DiNo ratings yet
- Statistics XIDocument332 pagesStatistics XIbhanu.chandu100% (1)
- EMPM01 Gather and Analyze Data InformationDocument28 pagesEMPM01 Gather and Analyze Data InformationAmal TharakaNo ratings yet
- Six Sigma Recap: BITS PilaniDocument32 pagesSix Sigma Recap: BITS PilaniFUNTV5No ratings yet
- Inventory Management PreetDocument28 pagesInventory Management PreetKawalpreet Singh MakkarNo ratings yet
- As Biology With Stafford Unit 3 Workbook AnswersDocument21 pagesAs Biology With Stafford Unit 3 Workbook Answersrifu91No ratings yet
- How To Write Common Types of EssaysDocument38 pagesHow To Write Common Types of EssaysВалерияNo ratings yet
- Edexcel English Language and Literature A Level CourseworkDocument7 pagesEdexcel English Language and Literature A Level Courseworkjlnggfajd100% (2)
- Transition and Theories of PopulationDocument68 pagesTransition and Theories of PopulationMBENOYNo ratings yet
- 1562 43343 1 PBDocument11 pages1562 43343 1 PBJb BrianNo ratings yet
- SM 38Document21 pagesSM 38ayushNo ratings yet
- Table of ContentsDocument4 pagesTable of Contentsapi-19625897100% (1)
- Internship Report On DBBL PDFDocument51 pagesInternship Report On DBBL PDFAnik Gagi100% (2)
- The Conceptualization of Sustainability in Operations ManagementDocument6 pagesThe Conceptualization of Sustainability in Operations ManagementNurul IzwaniNo ratings yet
- WHO CDS EPR 2007 6cDocument87 pagesWHO CDS EPR 2007 6cChifundo MandalaNo ratings yet
- Spatial Econometric S 5 ADocument19 pagesSpatial Econometric S 5 Acharls.maliteNo ratings yet
- Sales Skills AssessmentDocument5 pagesSales Skills Assessmentsinchanacr07No ratings yet
- UBC Press First Nations Studies Catalogue 2009-2010Document48 pagesUBC Press First Nations Studies Catalogue 2009-2010UBC Press University of British Columbia Press100% (2)
- Ich GCP: HistoryDocument57 pagesIch GCP: HistoryChandrashekhar Singh100% (1)
- The Particular Place of Anthropology in Interdisciplinary CurriculumDocument12 pagesThe Particular Place of Anthropology in Interdisciplinary CurriculumMariangela Manu MihaiNo ratings yet
- Correlation: Self Instructional Study Material Programme: M.A. Development StudiesDocument21 pagesCorrelation: Self Instructional Study Material Programme: M.A. Development StudiesSaima JanNo ratings yet
- Pr2 Module 1st Quarter Part 1Document13 pagesPr2 Module 1st Quarter Part 1Vanessa SantiagoNo ratings yet
- Mapping Your Innovation Strategy: Case Study CritiqueDocument5 pagesMapping Your Innovation Strategy: Case Study CritiqueHanan SalmanNo ratings yet
- Guide For Using LOINC Microbiology Terms: Logical Observation Identifiers Names and Codes (LOINC )Document124 pagesGuide For Using LOINC Microbiology Terms: Logical Observation Identifiers Names and Codes (LOINC )Ashwini KalantriNo ratings yet
- 268 cf3004Document7 pages268 cf3004api-535139620No ratings yet
- Programme Syllabus For Digital Leadership Master's Programme, 120 CreditsDocument9 pagesProgramme Syllabus For Digital Leadership Master's Programme, 120 CreditsA'del JummaNo ratings yet
- Group 1 RESEARCH PAPER The Effects of Modular Distance Learning MDL Approach in The Academic Performance of Grade 10 Students of NINHSDocument28 pagesGroup 1 RESEARCH PAPER The Effects of Modular Distance Learning MDL Approach in The Academic Performance of Grade 10 Students of NINHSjaylawrencebiluganfabonNo ratings yet
- WhereMathComesFrom Excerpt PDFDocument18 pagesWhereMathComesFrom Excerpt PDFStevanija StevanovicNo ratings yet
- CV Le Hung Viet BaoDocument4 pagesCV Le Hung Viet BaoNhat HoangNo ratings yet