Download as docx, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5833)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Transformer Oil Test ReportDocument2 pagesTransformer Oil Test Reportibubu2380% (5)
- Samples Inspection ReportDocument5 pagesSamples Inspection ReportArun GuptaNo ratings yet
- 9 Annual Review in Internal Medicine: GastroenterologyDocument26 pages9 Annual Review in Internal Medicine: GastroenterologyChino Paolo SamsonNo ratings yet
- Female Physiology Before PregnancyDocument81 pagesFemale Physiology Before PregnancyChino Paolo SamsonNo ratings yet
- BIOENERGETICS Trans - IncDocument3 pagesBIOENERGETICS Trans - IncChino Paolo SamsonNo ratings yet
- Peptic Ulcer DiseaseDocument6 pagesPeptic Ulcer DiseaseChino Paolo SamsonNo ratings yet
- Protein-Calories, Malnutrition & Nutritional DeficienciesDocument14 pagesProtein-Calories, Malnutrition & Nutritional DeficienciesChino Paolo SamsonNo ratings yet
- Protein-Calories, Malnutrition & Nutritional DeficienciesDocument15 pagesProtein-Calories, Malnutrition & Nutritional DeficienciesChino Paolo SamsonNo ratings yet
- Cardiac ArrhythmiasDocument11 pagesCardiac ArrhythmiasChino Paolo SamsonNo ratings yet
- Adrenal Insufficiency & Addison'S Disease: April 13, 2016Document6 pagesAdrenal Insufficiency & Addison'S Disease: April 13, 2016Chino Paolo SamsonNo ratings yet
- Hemolytic DiseaseDocument10 pagesHemolytic DiseaseChino Paolo SamsonNo ratings yet
- Where Will We Hold OnDocument1 pageWhere Will We Hold OnChino Paolo SamsonNo ratings yet
- Fluid Blance SGDDocument11 pagesFluid Blance SGDChino Paolo SamsonNo ratings yet
- OB Chap 22 - Normal LaborDocument4 pagesOB Chap 22 - Normal LaborChino Paolo SamsonNo ratings yet
- The Depth of Christ's LoveDocument14 pagesThe Depth of Christ's LoveChino Paolo SamsonNo ratings yet
- Examination in Hematology: NameDocument1 pageExamination in Hematology: NameChino Paolo SamsonNo ratings yet
- Reproductive Endocrinology FinalDocument98 pagesReproductive Endocrinology FinalChino Paolo SamsonNo ratings yet
- Long Term Safety AnalysesDocument3 pagesLong Term Safety AnalysesChino Paolo SamsonNo ratings yet
- Osce FormDocument2 pagesOsce FormChino Paolo SamsonNo ratings yet
- What Is Hemolysis of Sample?Document3 pagesWhat Is Hemolysis of Sample?Chino Paolo Samson100% (1)
- If I Am To Change A Negative Attitude of Mine, I Would Like To Change My Being - Why?Document3 pagesIf I Am To Change A Negative Attitude of Mine, I Would Like To Change My Being - Why?Chino Paolo SamsonNo ratings yet
- Pengembangan Dan Validasi Metode Kromatografi Lapis Tipis-Densitometri Untuk Analisis Pewarna Merah Sintentik Pada Beberapa Merek Saus Sambal SachetDocument6 pagesPengembangan Dan Validasi Metode Kromatografi Lapis Tipis-Densitometri Untuk Analisis Pewarna Merah Sintentik Pada Beberapa Merek Saus Sambal SachetIlaNo ratings yet
- Boilar Mounting and AccessoriesDocument44 pagesBoilar Mounting and AccessoriesSyam RajuNo ratings yet
- Tech-Venting HCL TanksDocument2 pagesTech-Venting HCL TanksDHAVALESH AMNo ratings yet
- New Microsoft Word DocumentDocument79 pagesNew Microsoft Word DocumentalexpharmNo ratings yet
- đề 5Document8 pagesđề 5Thư NguyễnNo ratings yet
- Smart Aquaculture Controlling System (S-AQUA)Document13 pagesSmart Aquaculture Controlling System (S-AQUA)pintuNo ratings yet
- Pareek CV 1Document5 pagesPareek CV 1Govind PareekNo ratings yet
- Five Year Development Plan (2003-2008)Document190 pagesFive Year Development Plan (2003-2008)Saurav SenNo ratings yet
- Discovering Metals - A Historical OverviewDocument12 pagesDiscovering Metals - A Historical OverviewMonisha SharmaNo ratings yet
- Jan San 2013Document172 pagesJan San 2013American Hotel Register CompanyNo ratings yet
- Sulthan Seyed Trading and Contracting SPCDocument3 pagesSulthan Seyed Trading and Contracting SPCSEYED SULTHANNo ratings yet
- CESD-10 Website PDFDocument3 pagesCESD-10 Website PDFDoc HadiNo ratings yet
- Study of Manufacturing Process ManagementDocument73 pagesStudy of Manufacturing Process ManagementAnil Kumar Singh0% (1)
- Phase Transfer CatalysisDocument15 pagesPhase Transfer CatalysisUnnati SinariNo ratings yet
- Reading U2Document5 pagesReading U2Quỳnh Trang Mai ThịNo ratings yet
- Volume Changes of ConcreteDocument17 pagesVolume Changes of ConcreteAljawhara AlnadiraNo ratings yet
- Validation and Qualification of Heating, Ventilation, Air ConDocument18 pagesValidation and Qualification of Heating, Ventilation, Air ConJai MurugeshNo ratings yet
- Sociology Final ProjectDocument16 pagesSociology Final Projectabt09No ratings yet
- Traumatic Brain Injury A Case Report: SCORE:40/50Document10 pagesTraumatic Brain Injury A Case Report: SCORE:40/50Allan CastroNo ratings yet
- High-Speed USB PCB Layout Recommendations: Figure 1. Microstrip Model of Differential ImpedanceDocument4 pagesHigh-Speed USB PCB Layout Recommendations: Figure 1. Microstrip Model of Differential ImpedanceopicaNo ratings yet
- Comparative Study of HerzbergDocument2 pagesComparative Study of HerzbergRoy Peter DelizoNo ratings yet
- Analysis of The Main Characters in Little Women by AlcottDocument6 pagesAnalysis of The Main Characters in Little Women by AlcottMiguel VizcainoNo ratings yet
- Strengthen ShoulderDocument5 pagesStrengthen Shouldernacole78No ratings yet
- Hipertec Wall DetailsDocument1 pageHipertec Wall Detailsamadeus_x64No ratings yet
- UPDRS-8 Robert Hauser MD 5-7-12Document1 pageUPDRS-8 Robert Hauser MD 5-7-12Robert A. Hauser, MDNo ratings yet
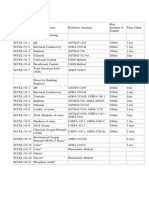
- Water, Soi & Aggregate Testing StandardsDocument2 pagesWater, Soi & Aggregate Testing StandardsSanjeewani Disna JayamaliNo ratings yet
- Hospital ReservesDocument84 pagesHospital ReservesThe Boston GlobeNo ratings yet
- Fluidisation: Stages in Fluidisation or Fluidisation CharacterisationDocument6 pagesFluidisation: Stages in Fluidisation or Fluidisation Characterisationdevilturn70No ratings yet