Download as pdf or txt
You might also like
- Immediate Management of Major Postpartum Haemorrhage (PPH) : Call For HelpDocument1 pageImmediate Management of Major Postpartum Haemorrhage (PPH) : Call For HelpSALMA HANINA100% (1)
- CTG Made Easy by Susan Gauge B006hgipbc PDFDocument6 pagesCTG Made Easy by Susan Gauge B006hgipbc PDFmashawahabNo ratings yet
- OPD 2 2019 Clinical Teaching PlanDocument3 pagesOPD 2 2019 Clinical Teaching PlanGee Ridad50% (2)
- Clinical Teaching Plan OBDocument7 pagesClinical Teaching Plan OBMyrtle Yvonne Ragub80% (5)
- Clinical Trial Feasibility ChecklistDocument3 pagesClinical Trial Feasibility ChecklistIrina NeiNo ratings yet
- Nursing Leadership and Management: Role Definitions and DifferencesDocument4 pagesNursing Leadership and Management: Role Definitions and DifferenceszainuddinNo ratings yet
- FU M1 CU4 LEC Critical Thinking and Assessment Foundation of Quality Nursing CareDocument8 pagesFU M1 CU4 LEC Critical Thinking and Assessment Foundation of Quality Nursing CareAthena Gonzales100% (1)
- AnatomyDocument6 pagesAnatomyKadulum100% (1)
- Training For Obstetric EmergenciesDocument34 pagesTraining For Obstetric EmergenciesElsaIsabelSilaen100% (1)
- Eradicating the Cancer of Religion: Hint: All People Have It!From EverandEradicating the Cancer of Religion: Hint: All People Have It!No ratings yet
- Israel 365 Your Hagaddah E-BookDocument61 pagesIsrael 365 Your Hagaddah E-BookMyrian Elizabeth DauerNo ratings yet
- Leadership & Amp Management 1 - SHIELADocument32 pagesLeadership & Amp Management 1 - SHIELAYvonne Kyla HabibonNo ratings yet
- Gelofusine: Iso-Oncotic Gelatine Solution For Intravenous Volume Substitution. Modified GelatineDocument6 pagesGelofusine: Iso-Oncotic Gelatine Solution For Intravenous Volume Substitution. Modified GelatineAshish KhomaneNo ratings yet
- Care of The High Risk NewbornDocument309 pagesCare of The High Risk NewbornClaire Alvarez OngchuaNo ratings yet
- Thesis Protocol: DR - Manali Kagathara Narayanamultispeciality Hospital, JaipurDocument15 pagesThesis Protocol: DR - Manali Kagathara Narayanamultispeciality Hospital, JaipurMaitree PNo ratings yet
- Preterm LaborDocument10 pagesPreterm Laborzuzuyasi65No ratings yet
- The Hidden Power of Prayer Amp FastingDocument7 pagesThe Hidden Power of Prayer Amp FastingWASHINGTON MANGAVUNo ratings yet
- Let's Get Healthy, Saints!: The Guide for Biblical HealthFrom EverandLet's Get Healthy, Saints!: The Guide for Biblical HealthNo ratings yet
- Ob Rapid Response Team Plan1Document20 pagesOb Rapid Response Team Plan1api-255697457100% (1)
- Algorithms For IV Fluid Therapy in Children and Young People in Hospital Set of 6 PDF 2190274957 PDFDocument6 pagesAlgorithms For IV Fluid Therapy in Children and Young People in Hospital Set of 6 PDF 2190274957 PDFFurqon AfandriNo ratings yet
- Anaesthesia Outside The Operating Theatre Update 2010Document5 pagesAnaesthesia Outside The Operating Theatre Update 2010Marcella Amadea100% (1)
- Ptl/Pprom and Multifetal Gestation: Anna Buabbud MD Ms3 LectureDocument38 pagesPtl/Pprom and Multifetal Gestation: Anna Buabbud MD Ms3 LectureNik C0% (1)
- Hemorragia PP OMSDocument48 pagesHemorragia PP OMSAsPonceMichNo ratings yet
- Management of Ruptured Uterus 6.0 PDFDocument14 pagesManagement of Ruptured Uterus 6.0 PDFpreethi preethaNo ratings yet
- Case History Ob & Gyne 4Document6 pagesCase History Ob & Gyne 4maksventileNo ratings yet
- Early Diagnosis & Prompt Treatment of Acute Abdominal Pain: Kiki Lukman The College of Surgeons of IndonesiaDocument69 pagesEarly Diagnosis & Prompt Treatment of Acute Abdominal Pain: Kiki Lukman The College of Surgeons of IndonesiaRani Silmi ZulafaNo ratings yet
- CQI by CommitteeDocument6 pagesCQI by CommitteeJhOy XiNo ratings yet
- Nyu Winthrop Hospital: Patient Flow Data and Joint Commission ComplianceDocument5 pagesNyu Winthrop Hospital: Patient Flow Data and Joint Commission ComplianceMarwa El SayedNo ratings yet
- ISQua Webinar - Nick Sevdalis - September 2017Document39 pagesISQua Webinar - Nick Sevdalis - September 2017utari dewiNo ratings yet
- Human Resources ManagementDocument27 pagesHuman Resources ManagementpoetriNo ratings yet
- Group Presentation 2Document19 pagesGroup Presentation 2api-509074425No ratings yet
- Implementation PlanDocument4 pagesImplementation Planapi-557858701No ratings yet
- 7.exercise On Formulating Quality Objectives and Use ofDocument63 pages7.exercise On Formulating Quality Objectives and Use ofMdnowfalNo ratings yet
- The Timeliness Initiative - Continuous Process Improvement For Prompt Initiation of Radiation Therapy TreatmentDocument8 pagesThe Timeliness Initiative - Continuous Process Improvement For Prompt Initiation of Radiation Therapy TreatmentnusantaramedikasolusindoNo ratings yet
- Turn Around Time.30901815Document6 pagesTurn Around Time.30901815Divya Shetty100% (1)
- 9nac 13 Integrating Assessment Into CPD ProgramsDocument65 pages9nac 13 Integrating Assessment Into CPD ProgramsNader ElbokleNo ratings yet
- Meresum Jurnal KeperawatanDocument9 pagesMeresum Jurnal KeperawatanRicky Ahmad FahreziNo ratings yet
- Leadership AnalysisDocument8 pagesLeadership Analysisapi-260554694No ratings yet
- Qip by DR James KleweDocument42 pagesQip by DR James KlewekumarNo ratings yet
- OB TriageDocument36 pagesOB TriagerelinNo ratings yet
- Aitken 2011Document8 pagesAitken 2011Denis MirandaNo ratings yet
- File 2Document24 pagesFile 2Johanine VillasantiagoNo ratings yet
- Safe Manual Transfers: Presenter: Kimberley Steeves, RN, DOHNDocument52 pagesSafe Manual Transfers: Presenter: Kimberley Steeves, RN, DOHNJasonJejametNo ratings yet
- STATION DESCRIPTIONS & FLOW CHARTS Face-to-Face Normal Circuit Patients in 4 Short Clinical StationsDocument25 pagesSTATION DESCRIPTIONS & FLOW CHARTS Face-to-Face Normal Circuit Patients in 4 Short Clinical StationsTom ChanNo ratings yet
- Effectiveness of Hourly RoundingDocument7 pagesEffectiveness of Hourly RoundingMaria Lpz100% (1)
- 04 Urinalysis CompetencyDocument20 pages04 Urinalysis Competencyمحمد عبدالواسع المسنيNo ratings yet
- Applying Lean/Toyota Production System Principles To Improve Phlebotomy Patient Satisfaction and WorkflowDocument6 pagesApplying Lean/Toyota Production System Principles To Improve Phlebotomy Patient Satisfaction and WorkflowHery IswantoNo ratings yet
- GiangaDocument12 pagesGiangaapi-504378310No ratings yet
- Clinical TeachingDocument29 pagesClinical TeachingJeonoh Florida100% (3)
- Defining The Nursing ProcessDocument6 pagesDefining The Nursing ProcessBrandy RaeNo ratings yet
- Implementing Early Mobilisation in The Intensive Care Unit - An Integrative ReviewDocument15 pagesImplementing Early Mobilisation in The Intensive Care Unit - An Integrative ReviewfabianneassisNo ratings yet
- Early Postoperative Ambulation Back To Basics A Quality Improvement Project PDFDocument7 pagesEarly Postoperative Ambulation Back To Basics A Quality Improvement Project PDFIndra MulianiNo ratings yet
- ZerobasedbudgetproposalDocument13 pagesZerobasedbudgetproposalapi-317112346No ratings yet
- ULHT Ward Rounds Plan From Every ReviewDocument23 pagesULHT Ward Rounds Plan From Every Reviewramansharma993399No ratings yet
- The Model For ImprovementDocument17 pagesThe Model For Improvementapi-487551161100% (1)
- Topic 6Document29 pagesTopic 6shalvenNo ratings yet
- Development and Application of Relactor Nursing Delegation Modelin IndonesiaDocument7 pagesDevelopment and Application of Relactor Nursing Delegation Modelin IndonesiaAstridNo ratings yet
- Qi Poster-Team HuddlesDocument1 pageQi Poster-Team Huddlesapi-258915393No ratings yet
- Global Rating Scale 2017-FinalDocument4 pagesGlobal Rating Scale 2017-Finalapi-396515657No ratings yet
- Spesifikasi Video Colposcope SLV 101Document1 pageSpesifikasi Video Colposcope SLV 101ponekNo ratings yet
- E-Catalog Borcad GracieDocument1 pageE-Catalog Borcad GracieponekNo ratings yet
- Spesifikasi Medgyn Al 106Document1 pageSpesifikasi Medgyn Al 106ponekNo ratings yet
- Gracie Brochure PDFDocument16 pagesGracie Brochure PDFponekNo ratings yet
- Leadership in Surgery Leadership in Surgery, or How To Create A Successful Surgical Unit UnitDocument37 pagesLeadership in Surgery Leadership in Surgery, or How To Create A Successful Surgical Unit UnitponekNo ratings yet
- Strategies To Developing An Institutional Program To Enhance Antimicrobial StewardshipDocument32 pagesStrategies To Developing An Institutional Program To Enhance Antimicrobial StewardshipponekNo ratings yet
- HHS Public Access: Estrogen Receptors and Human Disease: An UpdateDocument24 pagesHHS Public Access: Estrogen Receptors and Human Disease: An UpdateponekNo ratings yet
- Use of Aromatase Inhibitors To Treat Endometriosis-Related Pain Symptoms: A Systematic ReviewDocument10 pagesUse of Aromatase Inhibitors To Treat Endometriosis-Related Pain Symptoms: A Systematic ReviewponekNo ratings yet
- Review Article: Medical Treatments For Endometriosis-Associated Pelvic PainDocument12 pagesReview Article: Medical Treatments For Endometriosis-Associated Pelvic PainponekNo ratings yet
- Prof. Dr. Noor Pramono, M.med, SC, SP - Og (K)Document29 pagesProf. Dr. Noor Pramono, M.med, SC, SP - Og (K)ponekNo ratings yet
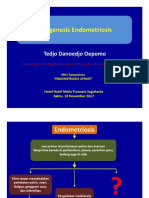
- Patogesis EndometriosisDocument39 pagesPatogesis EndometriosisponekNo ratings yet
- Ni Hms 454712Document14 pagesNi Hms 454712ponekNo ratings yet
- Perka BKN 1 TH 2013 Juklak PP 46 TH 2011Document39 pagesPerka BKN 1 TH 2013 Juklak PP 46 TH 2011ponekNo ratings yet
- Hospital-Based Triage of Obstetric Patients ACOGDocument4 pagesHospital-Based Triage of Obstetric Patients ACOGponekNo ratings yet
- MD India Preauth FormDocument2 pagesMD India Preauth FormM/s MicrotechNo ratings yet
- Melonorm CapsuleDocument3 pagesMelonorm Capsulehk_scribdNo ratings yet
- Aciclovir 400mg and 800mg TabletsDocument2 pagesAciclovir 400mg and 800mg TabletsKalyan NandanNo ratings yet
- PLENVUDocument24 pagesPLENVUDuwan ArismendyNo ratings yet
- Block BookDocument21 pagesBlock BookananaNo ratings yet
- General Abbreviations For Medical RecordsDocument9 pagesGeneral Abbreviations For Medical Recordsjainy12No ratings yet
- 5 Case Study Proper and History of Present IllnessDocument4 pages5 Case Study Proper and History of Present IllnessRegiena TamargoNo ratings yet
- Of Evaluation and Research in Education. 6 (1) : Daftar PustakaDocument3 pagesOf Evaluation and Research in Education. 6 (1) : Daftar PustakasukmaNo ratings yet
- Pediatric Lymphomas and Solid Tumors 0Document153 pagesPediatric Lymphomas and Solid Tumors 0yogendra madanNo ratings yet
- Carolyn Weiner ReportDocument4 pagesCarolyn Weiner ReportJerome Clark CidNo ratings yet
- Fess History Hand Splinting-MainDocument36 pagesFess History Hand Splinting-MainLilca Moraira Chaves100% (1)
- Medical Utopias: Ethical Reflections About Emerging Medical TechnologiesDocument35 pagesMedical Utopias: Ethical Reflections About Emerging Medical TechnologiesKPJConferenceNo ratings yet
- Mision Statements of Top 20 Pharmaceutical CompaniesDocument11 pagesMision Statements of Top 20 Pharmaceutical CompaniesRapstar VyNo ratings yet
- Interlabial Gap Behavior PDFDocument5 pagesInterlabial Gap Behavior PDFPatrícia BittencourtNo ratings yet
- What Is Deja Vu PresentationDocument8 pagesWhat Is Deja Vu PresentationSeskiara VivekaNo ratings yet
- 2008, Sanofi AventisDocument48 pages2008, Sanofi AventisAmeet DaulatNo ratings yet
- Thailand Dyspepsia Guidelines 2018Document12 pagesThailand Dyspepsia Guidelines 2018เด็กชายสมันตภัทร แฟนคลับอาจารย์กวงNo ratings yet
- Nursing Care Plan Acute Pain (Fronto-Temporal Mass)Document2 pagesNursing Care Plan Acute Pain (Fronto-Temporal Mass)deric100% (1)
- Clean Versus Sterile Management of Chronic WoundsDocument3 pagesClean Versus Sterile Management of Chronic WoundsDon RicaforteNo ratings yet
- Flail ChestDocument26 pagesFlail ChestStawan ChouguleNo ratings yet
- Alendronic Acid WarningsDocument13 pagesAlendronic Acid WarningsMihai VladescuNo ratings yet
- Artículo Terapia EsquemasDocument24 pagesArtículo Terapia EsquemasAna Salvador CastellanoNo ratings yet
- AppendicitisDocument21 pagesAppendicitisathya100% (1)
- Nclex Practice Exam Part1Document20 pagesNclex Practice Exam Part1stuffednurse40% (5)
- Rianti Soediro Suryo Tumor & Reconstruction Unit Cicendo Eye Hospital BandungDocument55 pagesRianti Soediro Suryo Tumor & Reconstruction Unit Cicendo Eye Hospital BandungyantiNo ratings yet
- Heart-Ily Fit 19Document4 pagesHeart-Ily Fit 19api-239426184No ratings yet
- Misoprostol PDFDocument5 pagesMisoprostol PDFEduardNo ratings yet
- Global Assessment (PG-SGA) : Scored Patient-Generated SubjectiveDocument1 pageGlobal Assessment (PG-SGA) : Scored Patient-Generated SubjectiveSafira Ridha UlyaNo ratings yet
- Jurnal Reading OsteomyelitisDocument11 pagesJurnal Reading Osteomyelitisfidela_ffNo ratings yet