Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5825)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Croak by Gina Damico ExcerptDocument29 pagesCroak by Gina Damico ExcerptHoughton Mifflin Harcourt0% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Choices, Values, FramesDocument8 pagesChoices, Values, Framesrandyzzz0% (1)
- IMA - Rules and Bye-Laws, 2019 PDFDocument100 pagesIMA - Rules and Bye-Laws, 2019 PDFManish Chandra PrabhakarNo ratings yet
- 5 X 5 Rmnch+aDocument2 pages5 X 5 Rmnch+aManish Chandra Prabhakar0% (1)
- National Guidelines For Screening of Hypothyroidism During PregnancyDocument48 pagesNational Guidelines For Screening of Hypothyroidism During PregnancyManish Chandra PrabhakarNo ratings yet
- Manish Chandra Prabhakar Mgims: 1 Reference-Harrison's Internal Medicine 18th EditionDocument79 pagesManish Chandra Prabhakar Mgims: 1 Reference-Harrison's Internal Medicine 18th EditionManish Chandra PrabhakarNo ratings yet
- Mhcet 2015 v44 KeyDocument2 pagesMhcet 2015 v44 KeyChemudupati BharaniNo ratings yet
- Concept Origin Development of Social SecuritiesDocument48 pagesConcept Origin Development of Social SecuritiesManish Chandra PrabhakarNo ratings yet
- Guidelines For Maternal Death Surveillance & ResponseDocument148 pagesGuidelines For Maternal Death Surveillance & ResponseManish Chandra Prabhakar100% (3)
- Social Security in India - Historical Development and Labour PolicyDocument29 pagesSocial Security in India - Historical Development and Labour PolicyManish Chandra Prabhakar100% (1)
- Maharashtra Medical PG Entrance 2014 QuestionDocument32 pagesMaharashtra Medical PG Entrance 2014 QuestionManish Chandra PrabhakarNo ratings yet
- Research Article Published in Plose One - Manish Chandra PrabhakarDocument6 pagesResearch Article Published in Plose One - Manish Chandra PrabhakarManish Chandra Prabhakar100% (1)
- Diabetes Care Guidelines - ADA 2014Document9 pagesDiabetes Care Guidelines - ADA 2014Manish Chandra PrabhakarNo ratings yet
- Stipend Increased For Intern Doctors at MUHS NashikDocument2 pagesStipend Increased For Intern Doctors at MUHS NashikManish Chandra Prabhakar100% (1)
- A Small Truth To Make Life 100%Document9 pagesA Small Truth To Make Life 100%qistina16No ratings yet
- Sri Sri Durga Saptshati (Sanskrit - Hindi)Document241 pagesSri Sri Durga Saptshati (Sanskrit - Hindi)Mukesh K. Agrawal62% (13)
- NEET PG 2012 Entrance Examination and PatternDocument4 pagesNEET PG 2012 Entrance Examination and PatternManish Chandra Prabhakar100% (1)
- NEET PG 2013 Information Booklet FINALDocument88 pagesNEET PG 2013 Information Booklet FINALManish Chandra PrabhakarNo ratings yet
- ICMR STS 2010 Report Submission ResultsDocument27 pagesICMR STS 2010 Report Submission ResultsManish Chandra PrabhakarNo ratings yet
- Icmr Sts Result 2011Document32 pagesIcmr Sts Result 2011Manish Chandra PrabhakarNo ratings yet
- How To WriteDocument13 pagesHow To WriteSebastian Quiroz FloresNo ratings yet
- Dizziness in The Elderly: Steven Zweig, MD Family and Community Medicine MU School of MedicineDocument34 pagesDizziness in The Elderly: Steven Zweig, MD Family and Community Medicine MU School of MedicineManish Chandra PrabhakarNo ratings yet
- Brubaker - 2009 - Ethnicity, Race, and NationalismDocument25 pagesBrubaker - 2009 - Ethnicity, Race, and NationalismGustavo RossiNo ratings yet
- Filología Neotestamentaria 50 - V.v.a.ADocument184 pagesFilología Neotestamentaria 50 - V.v.a.AGaspard de la Nuit100% (1)
- Doctor ZhivagoDocument3 pagesDoctor ZhivagoTaufiq XemoNo ratings yet
- NFC Technology Using RfidDocument7 pagesNFC Technology Using Rfidtrance 2k17No ratings yet
- UE18EE325 - Unit1 - Class4 - Performance Characteristics-StaticDocument16 pagesUE18EE325 - Unit1 - Class4 - Performance Characteristics-StaticGAYATHRI DEVI BNo ratings yet
- Sitaramarhi 1 PDFDocument33 pagesSitaramarhi 1 PDFnachNo ratings yet
- 2007 Justicia, Rebeca ECUADOR'S CHOCO ANDEAN CORRIDOR: A LANDSCAPE APPROACH FOR CONSERVATION AND SUSTAINABLE DEVELOPMENTDocument248 pages2007 Justicia, Rebeca ECUADOR'S CHOCO ANDEAN CORRIDOR: A LANDSCAPE APPROACH FOR CONSERVATION AND SUSTAINABLE DEVELOPMENTRebeca JusticiaNo ratings yet
- William - Shakespeare On The Double! Romeo and Juliet (Shakespeare On The Double!) (2006)Document243 pagesWilliam - Shakespeare On The Double! Romeo and Juliet (Shakespeare On The Double!) (2006)GogiGogos100% (1)
- Social PhilosophyDocument20 pagesSocial PhilosophyPrincess Diane Gravides100% (1)
- Viper 12ADocument21 pagesViper 12Aahmed hussainNo ratings yet
- NIS Daily Lesson Plan: Subject Unit/UOI TeacherDocument3 pagesNIS Daily Lesson Plan: Subject Unit/UOI TeacheraalshehabNo ratings yet
- The New Elliot Wave RuleDocument40 pagesThe New Elliot Wave RuleUlisses76100% (3)
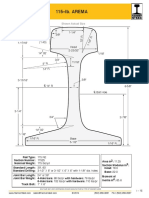
- Arema 115REDocument1 pageArema 115REAntonioNo ratings yet
- Dissertation Topics Substance MisuseDocument4 pagesDissertation Topics Substance MisuseBuyCollegePaperWestValleyCity100% (1)
- Characteristics That Define Our VictoryDocument5 pagesCharacteristics That Define Our VictoryLouie BiasongNo ratings yet
- Top 10 Machine Learning AlgorithmsDocument12 pagesTop 10 Machine Learning AlgorithmsUmang SoniNo ratings yet
- Labour Amendment ActDocument17 pagesLabour Amendment ActTakuNo ratings yet
- Matlab Review: Becoming Familiar With MATLABDocument13 pagesMatlab Review: Becoming Familiar With MATLABsolteanNo ratings yet
- Phonetics Activities PDF VersionDocument2 pagesPhonetics Activities PDF VersionBounouara MokhtariaNo ratings yet
- Prose Connotes Spoken or Written Discourse That Is Not Patterned Into Metric or Free VerseDocument5 pagesProse Connotes Spoken or Written Discourse That Is Not Patterned Into Metric or Free VerseElujekwute BenjaminNo ratings yet
- The Knowledge of First AidDocument9 pagesThe Knowledge of First AidMoon MyNo ratings yet
- Debugger BlackfinDocument26 pagesDebugger Blackfincarver_uaNo ratings yet
- A Transcription of Jean Françaix'S L'Horloge de Flore For Solo Oboe and Organ (Four Hands)Document67 pagesA Transcription of Jean Françaix'S L'Horloge de Flore For Solo Oboe and Organ (Four Hands)Juan MendozaNo ratings yet
- Effectiveness of Distribution Channel of Minute MaidDocument29 pagesEffectiveness of Distribution Channel of Minute MaidZil Shah0% (1)
- Newsletter Martha RogersDocument4 pagesNewsletter Martha Rogersapi-101279115No ratings yet
- The Perennial PhilosophyDocument14 pagesThe Perennial Philosophybrodie21100% (1)
- Final Test: Toefl Rekam Medik Semester 4: Zakaria Bintang Pamungkas, M.PD Grade: Semester 6 Part A GrammarDocument3 pagesFinal Test: Toefl Rekam Medik Semester 4: Zakaria Bintang Pamungkas, M.PD Grade: Semester 6 Part A Grammarbintang pamungkasNo ratings yet
- Kneehigh TheaterDocument2 pagesKneehigh Theaterapi-706488422No ratings yet