Download as pdf or txt
You might also like
- 1.pharmacy Technician Study GuideDocument31 pages1.pharmacy Technician Study GuideAlan Hao93% (14)
- Pharmacology UNIT 1 - Lesson 1Document29 pagesPharmacology UNIT 1 - Lesson 1Bea Bianca CruzNo ratings yet
- Malnutrition Screening Tool (MST) : Obtain Consent To Complete This Screening by AskingDocument2 pagesMalnutrition Screening Tool (MST) : Obtain Consent To Complete This Screening by AskingAku dienaNo ratings yet
- Species Common/Other Name Pathogenesis Mot/Infective Stage Diagnostic Stage I. NematodesDocument2 pagesSpecies Common/Other Name Pathogenesis Mot/Infective Stage Diagnostic Stage I. NematodesautumntreesNo ratings yet
- Izotope Ozone 5 Help DocumentationDocument149 pagesIzotope Ozone 5 Help DocumentationJoao PessoaNo ratings yet
- Status Gizi BB U AsupanDocument5 pagesStatus Gizi BB U AsupanPavlovaNo ratings yet
- Fall 2013 PDFDocument10 pagesFall 2013 PDFlopezmegoNo ratings yet
- HP Latex 310 - 1 PDFDocument4 pagesHP Latex 310 - 1 PDFHuma NicolaeNo ratings yet
- For The Security of CitizensDocument33 pagesFor The Security of CitizensWissem DhaouadiNo ratings yet
- PC3 Drum MapDocument1 pagePC3 Drum MapTaichiaikidokaNo ratings yet
- Treadmill Repair Service PDFDocument2 pagesTreadmill Repair Service PDFSabeur ShabouNo ratings yet
- 9 SC - I-ZoologyDocument3 pages9 SC - I-ZoologyNikhil SinhaNo ratings yet
- Alter Ego + A1 - Livre de L'élève (218p) PDFDocument218 pagesAlter Ego + A1 - Livre de L'élève (218p) PDFAnderson PereiraNo ratings yet
- Oxygen Pro Mini - User Guide - V1.1Document54 pagesOxygen Pro Mini - User Guide - V1.1Joker KillNo ratings yet
- In Flames LyricsDocument4 pagesIn Flames LyricsniyammmNo ratings yet
- General Knowledge and Trivia Quiz Sheets For Teenagers With Answers (1) - February 2015Document2 pagesGeneral Knowledge and Trivia Quiz Sheets For Teenagers With Answers (1) - February 2015Annie MartinezNo ratings yet
- 8047 en 03Document84 pages8047 en 03José CarlosNo ratings yet
- 21-Day Abundance Challenge (Intro)Document1 page21-Day Abundance Challenge (Intro)FNHANo ratings yet
- CFD Analysis of Regenerator of Gifford Mcmahon Cryocooler at 2k TemperatureDocument6 pagesCFD Analysis of Regenerator of Gifford Mcmahon Cryocooler at 2k TemperatureIJIRSTNo ratings yet
- Zeiss Ikon Contaflex BookDocument24 pagesZeiss Ikon Contaflex BookAnonymous Pr8IgKeNo ratings yet
- List MAC AddressDocument2,172 pagesList MAC AddressidnetskyNo ratings yet
- AWS Certified SysOps Administrator - Associate (Retiring July 26th, 2021)Document2 pagesAWS Certified SysOps Administrator - Associate (Retiring July 26th, 2021)Franter OkNo ratings yet
- Basic Operation of Cryocoolers and Related Thermal MachinesDocument58 pagesBasic Operation of Cryocoolers and Related Thermal MachinesJoão PinaNo ratings yet
- EASN Ksma Upute HR 2008 PDFDocument64 pagesEASN Ksma Upute HR 2008 PDFregistracijusNo ratings yet
- 9914659r02 PDFDocument157 pages9914659r02 PDFCathy CadellNo ratings yet
- LinuxCBT Feat. OpenPGP Edition NotesDocument10 pagesLinuxCBT Feat. OpenPGP Edition NotesAnghel FlorinNo ratings yet
- Addictive Drums Keymap PDFDocument1 pageAddictive Drums Keymap PDFEma VidovikNo ratings yet
- Canon Ir C2570 C3100 C3170Document174 pagesCanon Ir C2570 C3100 C3170nieblaashxNo ratings yet
- DiabetesDocument8 pagesDiabetesDanielValenciaNo ratings yet
- The Revolution of The Antidiabetic Drugs in CardiologyEuropean Heart Journal SupplementDocument5 pagesThe Revolution of The Antidiabetic Drugs in CardiologyEuropean Heart Journal Supplementgabriela naranjoNo ratings yet
- Standar Medical TreatmentDocument17 pagesStandar Medical TreatmentIba SuprasabaNo ratings yet
- Ada 2 PDFDocument21 pagesAda 2 PDFdepy oktaNo ratings yet
- Sustaine 10Document10 pagesSustaine 10Ivan Dario Hernandez ErazoNo ratings yet
- GlucoseDocument5 pagesGlucosebagsouravNo ratings yet
- Adverse Effects and Safety of SGLT-2 Inhibitors: Diabetes & Metabolism December 2014Document8 pagesAdverse Effects and Safety of SGLT-2 Inhibitors: Diabetes & Metabolism December 2014Sahrul RiadiNo ratings yet
- Hba Measurement Improves The Detection of Type 2 Diabetes in High-Risk Individuals With Nondiagnostic Levels of Fasting Plasma GlucoseDocument7 pagesHba Measurement Improves The Detection of Type 2 Diabetes in High-Risk Individuals With Nondiagnostic Levels of Fasting Plasma GlucoseStone WangNo ratings yet
- VildagliptinDocument7 pagesVildagliptinwanburyNo ratings yet
- Comparison of Efficacy and Safety Profile of Empagliflozin Versus Dapagliflozin As Add On Therapy in Type 2 Diabetic PatientsDocument6 pagesComparison of Efficacy and Safety Profile of Empagliflozin Versus Dapagliflozin As Add On Therapy in Type 2 Diabetic Patientsthomas albertNo ratings yet
- Cardiovascular Outcomes StudiesDocument5 pagesCardiovascular Outcomes StudiesAnonymous LOeICSOqNo ratings yet
- Dia Care 2011 Bonora S184 90Document7 pagesDia Care 2011 Bonora S184 90castillojessNo ratings yet
- Diabetes Mellitus Postrasplante y Prediabetes en Receptores de Trasplante Renal 2021Document13 pagesDiabetes Mellitus Postrasplante y Prediabetes en Receptores de Trasplante Renal 2021Casti Garcia GomezNo ratings yet
- Clinical Study: The Effects of Glucose Fluctuation On The Severity of Coronary Artery Disease in Type 2 Diabetes MellitusDocument6 pagesClinical Study: The Effects of Glucose Fluctuation On The Severity of Coronary Artery Disease in Type 2 Diabetes MellitusEgi Dwi SatriaNo ratings yet
- Comparison of Hba1C and Ogtt For The Diagnosis of Type 2 Diabetes in Children at Risk of DiabetesDocument7 pagesComparison of Hba1C and Ogtt For The Diagnosis of Type 2 Diabetes in Children at Risk of DiabetesAnnisa FujiantiNo ratings yet
- Slide Deck RTD Pre Diabetes - FinalDocument39 pagesSlide Deck RTD Pre Diabetes - FinalVieca FauziahNo ratings yet
- SGLT2 Inhibitors: The Future For Treatment of Type 2 Diabetes Mellitus and Other Chronic DiseasesDocument6 pagesSGLT2 Inhibitors: The Future For Treatment of Type 2 Diabetes Mellitus and Other Chronic DiseasesLucian Siriteanu100% (1)
- E001279 FullDocument9 pagesE001279 FullgasiasiNo ratings yet
- Biomarkeri Diabet 2011 PDFDocument9 pagesBiomarkeri Diabet 2011 PDFKaycsa AdrianaNo ratings yet
- Management of The Patient With Heart Failure and Diabetes May Insulin Be A ProblemDocument16 pagesManagement of The Patient With Heart Failure and Diabetes May Insulin Be A ProblemGIBSON JOEL CUNYA YAHUANANo ratings yet
- Research ArticleDocument12 pagesResearch ArticleRodas GetachewNo ratings yet
- Diabetes Care Glucosa Promedio EstimadaDocument6 pagesDiabetes Care Glucosa Promedio EstimadaGemeneza GonzalesNo ratings yet
- Continuous Glucose Monitoring: A Review of Recent Studies Demonstrating Improved Glycemic OutcomesDocument13 pagesContinuous Glucose Monitoring: A Review of Recent Studies Demonstrating Improved Glycemic OutcomesguillermocochaNo ratings yet
- Prediabetes A High Risk State For Diabetes Development PDFDocument12 pagesPrediabetes A High Risk State For Diabetes Development PDFDario Neri CortezNo ratings yet
- Guideline ADA 2010Document51 pagesGuideline ADA 2010Rivano Frits Henry PandalekeNo ratings yet
- General Aspects of Diabetes Mellitus20160808 31394 U4lcrv With Cover Page v2Document13 pagesGeneral Aspects of Diabetes Mellitus20160808 31394 U4lcrv With Cover Page v2PanjiNo ratings yet
- CE F (AnG) PF1 (MJ AP) PFA (MJ AP) PB (MJ AP) PN (AP)Document5 pagesCE F (AnG) PF1 (MJ AP) PFA (MJ AP) PB (MJ AP) PN (AP)Nimesh ModiNo ratings yet
- Dapa CKDDocument11 pagesDapa CKDCarlos Andres Tejeda PerezNo ratings yet
- Insulin Treatment in Patients With Diabetes Mellitus and Heart Failure in The Era of New Antidiabetic MedicationsDocument13 pagesInsulin Treatment in Patients With Diabetes Mellitus and Heart Failure in The Era of New Antidiabetic MedicationsIsamar AgostoNo ratings yet
- ADO in BRCDocument10 pagesADO in BRCVlahtNo ratings yet
- J of Inher Metab Disea - 2018 - Hoogeveen - A Preliminary Study of Telemedicine For Patients With Hepatic Glycogen StorageDocument8 pagesJ of Inher Metab Disea - 2018 - Hoogeveen - A Preliminary Study of Telemedicine For Patients With Hepatic Glycogen StorageDemetrius LacetNo ratings yet
- International Federation Diabetes 1 Hora Hiperglicemia IntermediaDocument21 pagesInternational Federation Diabetes 1 Hora Hiperglicemia IntermediaMundo Mariano Venezuela.No ratings yet
- Pathophysiology of Prediabetes and Treatment Implications For The Prevention of Type 2 Diabetes MellitusDocument10 pagesPathophysiology of Prediabetes and Treatment Implications For The Prevention of Type 2 Diabetes MellitusSamir BenmouffokNo ratings yet
- New Combination Treatments in The Management of Diabetes: Focus On Sitagliptin - MetforminDocument10 pagesNew Combination Treatments in The Management of Diabetes: Focus On Sitagliptin - MetforminGd PadmawijayaNo ratings yet
- Euglycemic Diabetic Ketoacidosis: A Predictable, Detectable, and Preventable Safety Concern With SGLT2 InhibitorsDocument5 pagesEuglycemic Diabetic Ketoacidosis: A Predictable, Detectable, and Preventable Safety Concern With SGLT2 InhibitorsPierreNo ratings yet
- E002619 FullDocument9 pagesE002619 FullUsee TvNo ratings yet
- Rose Pinwheel Potholder: Home Printer-Friendly PDF Printer-Friendly PDFDocument3 pagesRose Pinwheel Potholder: Home Printer-Friendly PDF Printer-Friendly PDFPriscilla ArtesNo ratings yet
- Cesta de Revista em CoraçãoDocument4 pagesCesta de Revista em CoraçãoPriscilla ArtesNo ratings yet
- WEB L SNC BouquetBasketsDocument2 pagesWEB L SNC BouquetBasketsPriscilla ArtesNo ratings yet
- Coats & Clark - 016 - Rose Rhapsody (C)Document4 pagesCoats & Clark - 016 - Rose Rhapsody (C)Priscilla ArtesNo ratings yet
- Coats & Clark - 09 - Crinoline Lady in CrochetDocument15 pagesCoats & Clark - 09 - Crinoline Lady in CrochetPriscilla ArtesNo ratings yet
- "Home Style Life Style Your Style.": P.O. Box 40 Listowel ON N4W 3H3Document1 page"Home Style Life Style Your Style.": P.O. Box 40 Listowel ON N4W 3H3Priscilla ArtesNo ratings yet
- Pastel Jute Baskets PDFDocument2 pagesPastel Jute Baskets PDFPriscilla ArtesNo ratings yet
- What Is It?: National Customer Service WeekDocument1 pageWhat Is It?: National Customer Service WeekPriscilla ArtesNo ratings yet
- Project: A Mother's Blessing: American Patchwork & Quilting - Quilt Sampler - Quilts and MoreDocument5 pagesProject: A Mother's Blessing: American Patchwork & Quilting - Quilt Sampler - Quilts and MorePriscilla ArtesNo ratings yet
- 213s-24 Flower Pot CozyDocument6 pages213s-24 Flower Pot CozyPriscilla ArtesNo ratings yet
- Daftar Pustaka: Affect Disord. 2003 73 (1-2) :123-31Document2 pagesDaftar Pustaka: Affect Disord. 2003 73 (1-2) :123-31Jumria Tandi PanggaloNo ratings yet
- Hypertensive Urgency: University of Perpetual Help System DALTA - Las PiñasDocument8 pagesHypertensive Urgency: University of Perpetual Help System DALTA - Las PiñasJustin HericoNo ratings yet
- ADRnewReporting Form 1.4Document2 pagesADRnewReporting Form 1.4Sourabh kundara50% (2)
- Spectrum - Bone Densitometry WOrkshopDocument16 pagesSpectrum - Bone Densitometry WOrkshopanbufelix1939No ratings yet
- Tugas Individu B.inggris (Midwifery Care)Document11 pagesTugas Individu B.inggris (Midwifery Care)irmanurulNo ratings yet
- Laporan Home Visit (Revin)Document24 pagesLaporan Home Visit (Revin)marinNo ratings yet
- CATS Clinical Guidelines Upper Airway Obstruction (UAO) : 1 AssessmentDocument4 pagesCATS Clinical Guidelines Upper Airway Obstruction (UAO) : 1 AssessmentJohn DoeNo ratings yet
- Links To Books and Additional MaterialDocument2 pagesLinks To Books and Additional MaterialCarl FernandesNo ratings yet
- Jurnal Hospitalisasi Pada AnakDocument9 pagesJurnal Hospitalisasi Pada Anaktrio hidayatNo ratings yet
- Screenshot 2021-11-20 at 7.28.44 AMDocument134 pagesScreenshot 2021-11-20 at 7.28.44 AMhhashemNo ratings yet
- Restrictions in Use and Availability of PharmaceuticalsDocument328 pagesRestrictions in Use and Availability of PharmaceuticalsinfooncoNo ratings yet
- ObjectiveDocument2 pagesObjectiveMarvinNo ratings yet
- Rajiv Gandhi University of Health Sciences Bangalore, KarnatakaDocument16 pagesRajiv Gandhi University of Health Sciences Bangalore, KarnatakaYadnya SaputraNo ratings yet
- Pregnancy and TBDocument24 pagesPregnancy and TBRoza MaulindraNo ratings yet
- Resume of Shirlene - R - SpatcherDocument1 pageResume of Shirlene - R - Spatcherapi-30461417No ratings yet
- New Jersey Health Department Report RE: Dr. John VecchioneDocument11 pagesNew Jersey Health Department Report RE: Dr. John VecchioneNews12NJWebNo ratings yet
- MBEB - Mindfulness-Based Emotional Balance Teacher Training IntensiveDocument10 pagesMBEB - Mindfulness-Based Emotional Balance Teacher Training IntensiveLina SantosNo ratings yet
- Loi - de Beer and THCDocument4 pagesLoi - de Beer and THCRyan TerblancheNo ratings yet
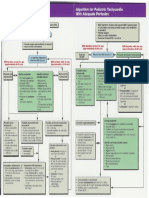
- Pediatric Tachycardia AlgorithmsDocument1 pagePediatric Tachycardia AlgorithmsGalih FatoniNo ratings yet
- Skull FractureDocument13 pagesSkull FractureEddie LimNo ratings yet
- Quiz Section: Level 1Document4 pagesQuiz Section: Level 1AinunZamiraNo ratings yet
- DR Prathap C ReddyDocument4 pagesDR Prathap C ReddyShakin ShaNo ratings yet
- Psych Unit I Part 1Document42 pagesPsych Unit I Part 1api-293070066No ratings yet
- Dowsing Resources & Techniques Joe Smith Diagnosing TechniqueDocument6 pagesDowsing Resources & Techniques Joe Smith Diagnosing TechniqueDina LazarosNo ratings yet
- Capítulo 10 SerdevDocument19 pagesCapítulo 10 SerdevErik BrooksNo ratings yet
- CSS Osteoarthritis GenuDocument33 pagesCSS Osteoarthritis Genufatimah putriNo ratings yet