Download as pdf or txt
You might also like
- Insert - Elecsys T3.ms - 11731360122.v26.enDocument4 pagesInsert - Elecsys T3.ms - 11731360122.v26.enGuneyden Guneyden100% (3)
- Total T4: For Use On The IMMULITE® and IMMULITE® 1000 SystemsDocument34 pagesTotal T4: For Use On The IMMULITE® and IMMULITE® 1000 SystemsEdgar GalvánNo ratings yet
- Inserto TSHDocument10 pagesInserto TSHyandros666No ratings yet
- 25 Tt4hu E01 PDFDocument9 pages25 Tt4hu E01 PDFDzejmenMerlinaNo ratings yet
- Sensitive Thyroid Stimulating Hormone (S-TSH) Enzyme Immunoassay Test Kit Catalog Number: BC-1003Document4 pagesSensitive Thyroid Stimulating Hormone (S-TSH) Enzyme Immunoassay Test Kit Catalog Number: BC-1003Juan SánchezNo ratings yet
- Free Triiodothyronine (Ft3) Enzyme Immunoassay Test Kit Catalog Number: BC-1006Document3 pagesFree Triiodothyronine (Ft3) Enzyme Immunoassay Test Kit Catalog Number: BC-1006Juan SánchezNo ratings yet
- Package Insert - TSH3Document6 pagesPackage Insert - TSH3Kadek Ayang Cendana Prahayu100% (1)
- ELISA Test For The Quantitative Determination of Total Triiodothyronine (T3) in Human Serum or PlasmaDocument2 pagesELISA Test For The Quantitative Determination of Total Triiodothyronine (T3) in Human Serum or PlasmaNghi NguyenNo ratings yet
- Myoglobin ELISA: For The Quantitative Determination of Myoglobin in Human SerumDocument8 pagesMyoglobin ELISA: For The Quantitative Determination of Myoglobin in Human SerumTanveerNo ratings yet
- Inserto T3Document2 pagesInserto T3cesiahdez0% (2)
- Protocol: 190989 Dentin Sialoprotein (DSP) Bioassay™ Elisa Kit (Human)Document4 pagesProtocol: 190989 Dentin Sialoprotein (DSP) Bioassay™ Elisa Kit (Human)MSKANo ratings yet
- NBL Rna Prep TrizolDocument7 pagesNBL Rna Prep Trizolmannukr565No ratings yet
- Enzyme Immunoassay Test Kit Catalog Number: 10304: Thyroid Stimulating Hormone (TSH)Document2 pagesEnzyme Immunoassay Test Kit Catalog Number: 10304: Thyroid Stimulating Hormone (TSH)petertrungNo ratings yet
- Can-Fte-260 - Free TestosteroneDocument2 pagesCan-Fte-260 - Free TestosteronevijayaNo ratings yet
- Helg0220ba 2020-08-09 Ka-Ab Lot 123Document40 pagesHelg0220ba 2020-08-09 Ka-Ab Lot 123yousrazeidan1979No ratings yet
- Total T3: For Use On The IMMULITE and Immulite 1000 SystemsDocument31 pagesTotal T3: For Use On The IMMULITE and Immulite 1000 SystemsEdgar Galván0% (1)
- Package Insert - 07204 - I - en - 30403 T3 PDFDocument5 pagesPackage Insert - 07204 - I - en - 30403 T3 PDFadybaila4680No ratings yet
- El TSHDocument2 pagesEl TSHMaherNo ratings yet
- FT3Document26 pagesFT3Florea RodicaNo ratings yet
- Access TSH (3rd IS) Instructions For Use ThyrotropinDocument13 pagesAccess TSH (3rd IS) Instructions For Use ThyrotropincarineNo ratings yet
- Elisa MethodDocument7 pagesElisa MethodNandia SeptiyoriniNo ratings yet
- Thyroid Stimulating Hormone (TSH) CLIADocument2 pagesThyroid Stimulating Hormone (TSH) CLIAp11.sethiaNo ratings yet
- El ft3Document2 pagesEl ft3Nghi NguyenNo ratings yet
- TSH Accubind Elisa Rev 3Document0 pagesTSH Accubind Elisa Rev 3Rafael ZevallosNo ratings yet
- ELISA Test For The Quantitative Determination of Thyrotropin (TSH) in Human SerumDocument2 pagesELISA Test For The Quantitative Determination of Thyrotropin (TSH) in Human SerumMaherNo ratings yet
- T4Document26 pagesT4Florea RodicaNo ratings yet
- El TestoDocument2 pagesEl TestoMaherNo ratings yet
- Rapid TSH Immulite - 230524111657469Document31 pagesRapid TSH Immulite - 230524111657469laboratorio almarNo ratings yet
- KAQ0621 Rev1Document16 pagesKAQ0621 Rev124redred4578No ratings yet
- Thyroid Stimulating Hormone (TSH) : Enzyme Immunoassay Test Kit Catalog Number: 10303Document2 pagesThyroid Stimulating Hormone (TSH) : Enzyme Immunoassay Test Kit Catalog Number: 10303Yousra ZeidanNo ratings yet
- 30 400 Vidas TSH: Summary and Explanation PrincipleDocument7 pages30 400 Vidas TSH: Summary and Explanation PrincipleWarda Niah100% (1)
- TSH ImmuliteDocument35 pagesTSH ImmuliteEdgar Galván50% (2)
- Biomérieux 30 400 Vidas TSH: Summary and Explanation PrincipleDocument7 pagesBiomérieux 30 400 Vidas TSH: Summary and Explanation Principlecass50% (2)
- MTT Proliferation Assay ProtocolsdaDocument2 pagesMTT Proliferation Assay ProtocolsdadwinugrohojuandaNo ratings yet
- 43 Hahhu E01Document8 pages43 Hahhu E01Cao Thi Le ChiNo ratings yet
- TSHDocument25 pagesTSHFlorea RodicaNo ratings yet
- Mouse TNF-α ELISA KitDocument13 pagesMouse TNF-α ELISA KitAnogenNo ratings yet
- Free T3 - IMMULITE 2000 Systems - Rev 24 DXDCM 09017fe9802975f7-1538193198932Document36 pagesFree T3 - IMMULITE 2000 Systems - Rev 24 DXDCM 09017fe9802975f7-1538193198932Jorge Stban PerezNo ratings yet
- Ft3 IiiDocument4 pagesFt3 IiihairiNo ratings yet
- Kit Insert Anti Toxoplasma Gondii IgGDocument13 pagesKit Insert Anti Toxoplasma Gondii IgGAghnia Asy S.No ratings yet
- In Vitro Methods For Detecting Cytotoxicity: UNIT 2.6Document27 pagesIn Vitro Methods For Detecting Cytotoxicity: UNIT 2.6hiền nguyễnNo ratings yet
- (Intended Use) : Instruction ManualDocument8 pages(Intended Use) : Instruction ManualTPNo ratings yet
- bc-1001 TSHDocument5 pagesbc-1001 TSHJuan SánchezNo ratings yet
- Human DSP (Dentin Sialoprotein) ELISA KitDocument9 pagesHuman DSP (Dentin Sialoprotein) ELISA Kitmsk adiwiryaNo ratings yet
- Elecsys FT3Document4 pagesElecsys FT3Arnaz AdisaputraNo ratings yet
- H Alpha 1 Antitrypsin: Immunoperoxidase Assay For Determination of Alpha 1-Antitrypsin in Human SamplesDocument4 pagesH Alpha 1 Antitrypsin: Immunoperoxidase Assay For Determination of Alpha 1-Antitrypsin in Human Samplesyunitaekawati1459No ratings yet
- Elisa KitDocument5 pagesElisa KitYani Nyiik0% (1)
- El ft4Document2 pagesEl ft4Nghi NguyenNo ratings yet
- CSB E13415hDocument14 pagesCSB E13415hhuripNo ratings yet
- Rat PDGF (Platelet-Derived Growth Factor) ELISA Kit: Instruction ManualDocument9 pagesRat PDGF (Platelet-Derived Growth Factor) ELISA Kit: Instruction ManualSigit Harya HutamaNo ratings yet
- U TSHDocument2 pagesU TSHpetertrungNo ratings yet
- Anti-Thyroid Peroxidase Antibody (Anti-TPO) CLIA: 2 X 50 Test 52025070Document2 pagesAnti-Thyroid Peroxidase Antibody (Anti-TPO) CLIA: 2 X 50 Test 52025070p11.sethiaNo ratings yet
- Mouse IL-8 (Interleukin 8) ELISA Kit: Instruction ManualDocument9 pagesMouse IL-8 (Interleukin 8) ELISA Kit: Instruction ManualAak An NasherNo ratings yet
- A TpoDocument4 pagesA TpoJimboreanu György PaulaNo ratings yet
- MTT AssayDocument2 pagesMTT AssayBatlia GonzalezNo ratings yet
- ELISA Kit For Angiotensin II (AngII) E90005RaDocument8 pagesELISA Kit For Angiotensin II (AngII) E90005RaTan Jie HuiNo ratings yet
- B77706K AccessTSH 3rdDocument13 pagesB77706K AccessTSH 3rdТатьяна ИсаеваNo ratings yet
- TSH OrigeneDocument3 pagesTSH OrigeneAlejandro AlvaradoNo ratings yet
- IfU ATG1010engl, DT, Es-18062014 Ab Lot 016Document23 pagesIfU ATG1010engl, DT, Es-18062014 Ab Lot 016f.baxyNo ratings yet
- Tramadolparacetamol Fixed-Dose Combination in TheDocument21 pagesTramadolparacetamol Fixed-Dose Combination in ThecitrahdynNo ratings yet
- Daftar Nutrisi ParenteralDocument6 pagesDaftar Nutrisi Parenteralcitrahdyn100% (1)
- HPLC Analysis of Nicotinamide Pyridoxine Riboflavi PDFDocument9 pagesHPLC Analysis of Nicotinamide Pyridoxine Riboflavi PDFcitrahdynNo ratings yet
- Comparison of Physicochemical Properties of Suppositories Containing Starch HydrolysatesDocument5 pagesComparison of Physicochemical Properties of Suppositories Containing Starch HydrolysatescitrahdynNo ratings yet
- MPRA Paper 23362Document12 pagesMPRA Paper 23362citrahdynNo ratings yet
- Fullpapers Jakic6136c3c4efullDocument8 pagesFullpapers Jakic6136c3c4efullcitrahdynNo ratings yet
- Mzuzu Diocese Chemistry Paper IDocument14 pagesMzuzu Diocese Chemistry Paper IMoses SamalaniNo ratings yet
- Frequently Used Terms in Vedic AstrologyDocument3 pagesFrequently Used Terms in Vedic AstrologyNarayana Remala100% (1)
- Summary Sheet: Client Consultant Contractor Project: Package Ii: Document Name: Document No. 2 REVDocument42 pagesSummary Sheet: Client Consultant Contractor Project: Package Ii: Document Name: Document No. 2 REVPramod B.Wankhade100% (1)
- IV Infusion: Purpose of Starting IV'sDocument6 pagesIV Infusion: Purpose of Starting IV'sKiara Denise TamayoNo ratings yet
- Guia de Aprendizaje-QuantifiersDocument8 pagesGuia de Aprendizaje-Quantifiersangelita berdugoNo ratings yet
- NTP 2020 Kakatiya - Mega - Textile - ParkDocument2 pagesNTP 2020 Kakatiya - Mega - Textile - ParkNv MannaNo ratings yet
- Consumer Electronics Servicing Learning Module 130610203451 Phpapp02Document145 pagesConsumer Electronics Servicing Learning Module 130610203451 Phpapp02Maureen Pusing80% (10)
- Programmable 3 Channel Power Supply 526Document2 pagesProgrammable 3 Channel Power Supply 526digiarkanandNo ratings yet
- Space - The Final FrontierDocument51 pagesSpace - The Final FrontierAbdul Shakoor100% (1)
- Cost CurvesDocument2 pagesCost CurvesSumit Ray100% (1)
- Envision Math 3th GR Topic 5Document28 pagesEnvision Math 3th GR Topic 5Anna K. RiveraNo ratings yet
- 2003 Corkscrew Bike Trail StudyDocument25 pages2003 Corkscrew Bike Trail StudyJoey KulkinNo ratings yet
- LPile 2015 Technical ManualDocument238 pagesLPile 2015 Technical ManualMahesh HanmawaleNo ratings yet
- Rectus Femoris in Gait CycleDocument5 pagesRectus Femoris in Gait CycleanjelikaNo ratings yet
- 10 Herbal Medicines Approved by The DohDocument13 pages10 Herbal Medicines Approved by The DohLark SantiagoNo ratings yet
- Precos Souza CruzDocument12 pagesPrecos Souza CruzPablo ToazzaNo ratings yet
- Sistemas de Refrigeracion Industrial en AmoniacoDocument102 pagesSistemas de Refrigeracion Industrial en AmoniacoDiego Trinidad100% (8)
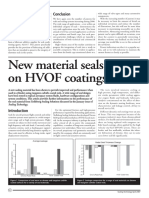
- New Material Seals Better On HVOF CoatingsDocument2 pagesNew Material Seals Better On HVOF Coatingssandbad2100% (2)
- Turbine Cat SolarDocument2 pagesTurbine Cat SolarAbid Lakhani100% (1)
- Directional Terms and Body TermsDocument26 pagesDirectional Terms and Body TermsMartinArciniegaNo ratings yet
- Wire Nails Manufacturing Business. How To Start Nail Factory. Profitable Small Business Ideas in India-887813Document63 pagesWire Nails Manufacturing Business. How To Start Nail Factory. Profitable Small Business Ideas in India-887813MuazNo ratings yet
- ODME FailureDocument3 pagesODME FailureNatalie JonesNo ratings yet
- AccurioLabel 400 - Basic - Demo - Script - v1.0 - EDocument33 pagesAccurioLabel 400 - Basic - Demo - Script - v1.0 - EDiego LanderosNo ratings yet
- Why Jesus Is Worthy of WorshipDocument7 pagesWhy Jesus Is Worthy of Worshiprukmani27No ratings yet
- PDF Mechanical Circulatory Support Principles and Applications 2Nd Edition David L Joyce MD Ebook Full ChapterDocument53 pagesPDF Mechanical Circulatory Support Principles and Applications 2Nd Edition David L Joyce MD Ebook Full Chapterglen.webb399100% (5)
- HIPPROSTHESISCATALOGDocument98 pagesHIPPROSTHESISCATALOGBrenda Martinez RomanNo ratings yet
- Seal of History Our Inheritance in The Great Seal of USDocument207 pagesSeal of History Our Inheritance in The Great Seal of USAlfred E. NewmanNo ratings yet
- TXP® BTC: GeometryDocument2 pagesTXP® BTC: GeometryLeonardo BarriosNo ratings yet
- PhiloDocument2 pagesPhilomia jane AguilarNo ratings yet
- Hows The Soil? Maniyar Village Has Red Soil and Black Soil For Its Villages. (Document4 pagesHows The Soil? Maniyar Village Has Red Soil and Black Soil For Its Villages. (Chinmay KaranNo ratings yet