Download as pdf or txt
You might also like
- Blood Type Punnett Square PracticeDocument3 pagesBlood Type Punnett Square PracticeGary Garlan100% (1)
- 01) 2013-38 이석근Document12 pages01) 2013-38 이석근Nosya RachmawatiNo ratings yet
- Ameloblastic Fibro-Odontoma: A Case ReportDocument4 pagesAmeloblastic Fibro-Odontoma: A Case Reportoral pathNo ratings yet
- Tumores Odontogenicos Patología PDFDocument17 pagesTumores Odontogenicos Patología PDFDayanara Medina AldazNo ratings yet
- 2017 - Ameloblastic Fibroodontoma Uncommon Case Presentation in A 6 Year Old ChildDocument4 pages2017 - Ameloblastic Fibroodontoma Uncommon Case Presentation in A 6 Year Old ChildSyifa IKNo ratings yet
- Ameloblastic Fibroma: Report of A Case: Su-Gwan Kim, DDS, PHD, and Hyun-Seon Jang, DDS, PHDDocument3 pagesAmeloblastic Fibroma: Report of A Case: Su-Gwan Kim, DDS, PHD, and Hyun-Seon Jang, DDS, PHDdoktergigikoeNo ratings yet
- Tumores OdontogenicDocument17 pagesTumores OdontogenicrachmaniabudiatiNo ratings yet
- Odontogenic Tumor Ameloblastoma: Presented By: Ankita Singh Bds Final Year Roll No 37Document73 pagesOdontogenic Tumor Ameloblastoma: Presented By: Ankita Singh Bds Final Year Roll No 37ankita sethiNo ratings yet
- Información Épuli FibromatosoDocument3 pagesInformación Épuli FibromatosoDaniela IbarraNo ratings yet
- 6 Pediatric Odontogenic Tumors. Oral and Maxillofacial Surgery Clinics of North AmericaDocument14 pages6 Pediatric Odontogenic Tumors. Oral and Maxillofacial Surgery Clinics of North AmericaalexandreNo ratings yet
- Odontogenic TumorsDocument62 pagesOdontogenic TumorsMeera SNo ratings yet
- Meta 2.1 Ocampo LibroDocument21 pagesMeta 2.1 Ocampo LibrogermanNo ratings yet
- Meta 2.1 Ocampo Libro (01-07)Document7 pagesMeta 2.1 Ocampo Libro (01-07)germanNo ratings yet
- Flint Cumming Otolaryngology CHAPTER 93 - Odontogenesis Odontogenic Cysts and Odontogenic TumorsDocument20 pagesFlint Cumming Otolaryngology CHAPTER 93 - Odontogenesis Odontogenic Cysts and Odontogenic TumorsNicco Jake AlegroNo ratings yet
- Ipe Varghese. V Sudha. S Resmi G. Nair Sherin. NDocument5 pagesIpe Varghese. V Sudha. S Resmi G. Nair Sherin. NeditorompjNo ratings yet
- Case Report Ameloblastic Fibroma: Report of 3 Cases and Literature ReviewDocument5 pagesCase Report Ameloblastic Fibroma: Report of 3 Cases and Literature ReviewcareNo ratings yet
- 3.podoplanin Antibody MainDocument6 pages3.podoplanin Antibody MainNitin KhanduriNo ratings yet
- Mixed Tumors of Odontogenic Origin WordDocument31 pagesMixed Tumors of Odontogenic Origin WordAshimNo ratings yet
- Ameloblastic Fibro-Odontoma in A BovineDocument4 pagesAmeloblastic Fibro-Odontoma in A BovineAndrea Carolina Rojas MendezNo ratings yet
- Unicystic Ameloblastoma - Investigation Into An Enigma: IOSR Journal of Dental and Medical Sciences February 2020Document5 pagesUnicystic Ameloblastoma - Investigation Into An Enigma: IOSR Journal of Dental and Medical Sciences February 2020dr.filipcristian87No ratings yet
- 55-Submission File-100-1-10-20190812Document4 pages55-Submission File-100-1-10-20190812I Dewa Wisnu PutraNo ratings yet
- Odontogenic Cysts and Neoplasms 2017 PDFDocument46 pagesOdontogenic Cysts and Neoplasms 2017 PDFFadly RasyidNo ratings yet
- Jurnal GilutDocument11 pagesJurnal GilutAvif PutraNo ratings yet
- Odontomes and Odontogenic TumoursDocument16 pagesOdontomes and Odontogenic TumoursHasan AlbalwaNo ratings yet
- Tumor Odontogenico EscamosoDocument4 pagesTumor Odontogenico Escamosoメカ バルカNo ratings yet
- Dr. Yoseph - The Role of Radiotherapy in The Management of Ameloblastoma and Ameloblastic CarcinomaDocument10 pagesDr. Yoseph - The Role of Radiotherapy in The Management of Ameloblastoma and Ameloblastic CarcinomaOnkologi Radiasi Angkatan 23No ratings yet
- Article 7-52250925Document4 pagesArticle 7-52250925AbinayaBNo ratings yet
- Ameloblastoma: Submitted byDocument9 pagesAmeloblastoma: Submitted byJana AliNo ratings yet
- Ameloblastic Fibro-Dentinoma of Mandible: A Case ReportDocument3 pagesAmeloblastic Fibro-Dentinoma of Mandible: A Case ReportBrutusRexNo ratings yet
- Review Article: Bone Diseases of The JawsDocument7 pagesReview Article: Bone Diseases of The Jawsh20pologtNo ratings yet
- 2013 Article 501Document3 pages2013 Article 501oral pathNo ratings yet
- Free Fibular Osteoseptocutaneus Flap For Reconstruction GiantameloblastomaDocument7 pagesFree Fibular Osteoseptocutaneus Flap For Reconstruction GiantameloblastomaLINDANo ratings yet
- Ameloblastoma 140624025211 Phpapp02Document51 pagesAmeloblastoma 140624025211 Phpapp02agusNo ratings yet
- Clasification of Odontogenic Tumours A ReviewDocument6 pagesClasification of Odontogenic Tumours A ReviewJuan Carlos MeloNo ratings yet
- dmf2SA Presentasi01Document5 pagesdmf2SA Presentasi01Iftinan LQNo ratings yet
- Odontomes and Odontogenic TumoursDocument16 pagesOdontomes and Odontogenic TumourssarahNo ratings yet
- Articulo 5Document8 pagesArticulo 5FernierNo ratings yet
- CH 30Document22 pagesCH 30Alejandra Oliveros VargasNo ratings yet
- Odontogenic Tumor: Oral PathologyDocument17 pagesOdontogenic Tumor: Oral PathologyJoker KillerNo ratings yet
- JPNR - S04 - 233Document6 pagesJPNR - S04 - 233Ferisa paraswatiNo ratings yet
- Ameloblastoma Arising in The Wall of Dentigerous Cyst - A Case ReportDocument3 pagesAmeloblastoma Arising in The Wall of Dentigerous Cyst - A Case ReportSenussi IbtisamNo ratings yet
- Maxillary Unicystic Ameloblastoma: A Review of The LiteratureDocument0 pagesMaxillary Unicystic Ameloblastoma: A Review of The LiteratureXatly OviedoNo ratings yet
- Histopathological Insight of An Adenomatoid Odontogenic Lesion - A Cyst, Tumor or Hamartoma?Document6 pagesHistopathological Insight of An Adenomatoid Odontogenic Lesion - A Cyst, Tumor or Hamartoma?gunawan121982No ratings yet
- Odontogenic Cysts 2015Document11 pagesOdontogenic Cysts 2015Fadly RasyidNo ratings yet
- Ameloblastoma Report CaseDocument6 pagesAmeloblastoma Report CaseYuzketNo ratings yet
- Case Report: Enamel Pearls Implications On Periodontal DiseaseDocument4 pagesCase Report: Enamel Pearls Implications On Periodontal DiseasenediaNo ratings yet
- CA LS Bướu Nhiều Hốc - Multilocular Radiolucency in the Body of MandibleDocument4 pagesCA LS Bướu Nhiều Hốc - Multilocular Radiolucency in the Body of MandibleThành Luân NguyễnNo ratings yet
- Follicular With Plexiform Ameloblastoma in Anterior Mandible: Report of Case and Literature ReviewDocument6 pagesFollicular With Plexiform Ameloblastoma in Anterior Mandible: Report of Case and Literature Reviewluckytung07No ratings yet
- 2007 HuDocument8 pages2007 HuKAREN ANAIS URGILES ESPINOZANo ratings yet
- Aggressive Granular Cell Ameloblastoma Arising From Radicular Cyst: A Case Report of An Unusual Variant and A Public Health ConcernDocument8 pagesAggressive Granular Cell Ameloblastoma Arising From Radicular Cyst: A Case Report of An Unusual Variant and A Public Health Concernkumar chandan srivastavaNo ratings yet
- Saudi Journal of Pathology and Microbiology (SJPM) : Case ReportDocument3 pagesSaudi Journal of Pathology and Microbiology (SJPM) : Case ReportSuman ChaturvediNo ratings yet
- AmeloblastomaDocument6 pagesAmeloblastomaNASTYHAIR 24No ratings yet
- Peripheral Ameloblastic FibromaDocument3 pagesPeripheral Ameloblastic FibromadoktergigikoeNo ratings yet
- Pathogenesis of Odontogenic Cysts: ArticleDocument5 pagesPathogenesis of Odontogenic Cysts: ArticleHusnul KhatimahNo ratings yet
- Who Is in and Who Is OutDocument6 pagesWho Is in and Who Is OutJuan Carlos MeloNo ratings yet
- Terjemahan Dari Ameloblastoma IndonesiaDocument2 pagesTerjemahan Dari Ameloblastoma IndonesiaATHALLAH NISRINA AMANDANo ratings yet
- Quistes y Tumores Odontogénicos 1Document9 pagesQuistes y Tumores Odontogénicos 1Rocio CacñahuarayNo ratings yet
- Odontogenic TumorDocument56 pagesOdontogenic TumoramieNo ratings yet
- Peripheral Ameloblastoma of The GingivaDocument5 pagesPeripheral Ameloblastoma of The GingivaLourena MarinhoNo ratings yet
- Multiple Enamel Pearls in Two Siblings Detected by Volumetric Computed TomographyDocument5 pagesMultiple Enamel Pearls in Two Siblings Detected by Volumetric Computed TomographySalma KilledarNo ratings yet
- The Dental Pulp: Biology, Pathology, and Regenerative TherapiesFrom EverandThe Dental Pulp: Biology, Pathology, and Regenerative TherapiesNo ratings yet
- Controlling Microbial Growth - MicrobiologyDocument9 pagesControlling Microbial Growth - MicrobiologyDanette PriceNo ratings yet
- Cambridge O Level: Biology 5090/21 May/June 2021Document14 pagesCambridge O Level: Biology 5090/21 May/June 2021uwu xdNo ratings yet
- READING PART 1 The Wonder of TreesDocument3 pagesREADING PART 1 The Wonder of TreesHenry Arias Soliz0% (1)
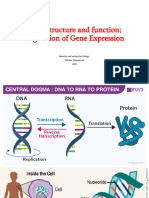
- Gene Structure and Function Regulation of Gene Expression - Part 1Document29 pagesGene Structure and Function Regulation of Gene Expression - Part 1Ana AbuladzeNo ratings yet
- The Antioxidant, Immunomodulatory, and Anti Inflammatory Activities of Spirulina: An OverviewDocument24 pagesThe Antioxidant, Immunomodulatory, and Anti Inflammatory Activities of Spirulina: An OverviewPlacido Rojas FrancoNo ratings yet
- Harvesting The DeadDocument6 pagesHarvesting The DeadDominic SistiNo ratings yet
- Nursing Pharmacology 1628877935Document771 pagesNursing Pharmacology 1628877935Arantxa HilarioNo ratings yet
- Chapter 45 Hormones & Endocrine SystemDocument9 pagesChapter 45 Hormones & Endocrine Systemblazianxviet0% (1)
- 18S rDNA Sequence-Structure Phylogeny of The Trypanosomatida (Kinetoplastea, Euglenozoa) With Special Reference On TrypanosomaDocument21 pages18S rDNA Sequence-Structure Phylogeny of The Trypanosomatida (Kinetoplastea, Euglenozoa) With Special Reference On TrypanosomaGustavo AndresNo ratings yet
- The Requirements of Mannose Binding LectinDocument2 pagesThe Requirements of Mannose Binding LectinNurul NadiaNo ratings yet
- Bellinger (FC) (Appellant) v. BellingerDocument15 pagesBellinger (FC) (Appellant) v. BellingerRichy2643100% (1)
- Materi MIMBAR 20 - BPK HadiDocument20 pagesMateri MIMBAR 20 - BPK HadiYoga RivaldiNo ratings yet
- Micropropagation of PapayaDocument1 pageMicropropagation of PapayamanojbanNo ratings yet
- DNADocument23 pagesDNAMuneeb Jan100% (1)
- Study Guide - CSTDDocument27 pagesStudy Guide - CSTDrbsmun9469No ratings yet
- HIV-associated Kaposi Sarcoma: Pathogenic MechanismsDocument9 pagesHIV-associated Kaposi Sarcoma: Pathogenic MechanismsafbmgNo ratings yet
- SWH AQA Revision Guide Biology 1Document42 pagesSWH AQA Revision Guide Biology 1afshinNo ratings yet
- PATHOPHYSIOLOGY OF OSTEOSARCOMaDocument1 pagePATHOPHYSIOLOGY OF OSTEOSARCOMakyawNo ratings yet
- Large Granular Lymphocytic Leukemia. Current Diagnostic and Therapeutic Approaches and Novel Treatment OptionsDocument29 pagesLarge Granular Lymphocytic Leukemia. Current Diagnostic and Therapeutic Approaches and Novel Treatment OptionsOrxan HumbetovNo ratings yet
- Stem Cell Research EssayDocument7 pagesStem Cell Research Essayapi-286667026No ratings yet
- Mechanism of Salivary GlandDocument5 pagesMechanism of Salivary GlandNirmala M. KarimatannisaNo ratings yet
- Michael Banton The Vertical and Horizontal Dimensions of The Word RaceDocument14 pagesMichael Banton The Vertical and Horizontal Dimensions of The Word RaceAldair RodriguesNo ratings yet
- Mechanism of Animal DispersalDocument19 pagesMechanism of Animal DispersalXainab SaeedNo ratings yet
- Timeline ActivityDocument2 pagesTimeline ActivityhanniemaelimonNo ratings yet
- Activity ProposalSeminarDocument6 pagesActivity ProposalSeminarWil AlgonesNo ratings yet
- Lupus Nephritis Diagnosis and ClassificationDocument37 pagesLupus Nephritis Diagnosis and ClassificationElena StepanNo ratings yet
- 1 PDFDocument467 pages1 PDFElena AsaveiNo ratings yet
- Planthormones 141025004114 Conversion Gate02 PDFDocument75 pagesPlanthormones 141025004114 Conversion Gate02 PDFSaiTimmarao100% (1)
- Antibacterial Activity of Cassia Alata Linn. (Akapulko) Leaf Extract On Staphylococcus Aureus-Associated Skin InfectionDocument15 pagesAntibacterial Activity of Cassia Alata Linn. (Akapulko) Leaf Extract On Staphylococcus Aureus-Associated Skin InfectionjennieNo ratings yet