Download as pdf or txt
You might also like
- Bad Pharma - A Fraud in Clinical Trail DataDocument27 pagesBad Pharma - A Fraud in Clinical Trail DataSimran WaghelaNo ratings yet
- (INFEKSI) - FKUI - Nelwan Score Typhoid Fever.2016Document10 pages(INFEKSI) - FKUI - Nelwan Score Typhoid Fever.2016Yolanda FitrianiNo ratings yet
- Referat Nutrition in Critical IllDocument56 pagesReferat Nutrition in Critical Illsyahnas yarahmaNo ratings yet
- Protein and Nutrition in Critically Ill PatientDocument43 pagesProtein and Nutrition in Critically Ill PatientTom KristiantoNo ratings yet
- Clinical Case Report Powerpoint PresentationDocument24 pagesClinical Case Report Powerpoint Presentationapi-354139540100% (1)
- Pathology Outlines - Papillary Carcinoma - GeneralDocument6 pagesPathology Outlines - Papillary Carcinoma - Generalpatka1rNo ratings yet
- Slide Chronic Pain-Rudy Hidayat-Iai PDFDocument30 pagesSlide Chronic Pain-Rudy Hidayat-Iai PDFAsri ArrachmanNo ratings yet
- Nutrition Support in Critically Ill PatientDocument19 pagesNutrition Support in Critically Ill PatienttantoNo ratings yet
- Target Range For Glycemic Control: 80-140 MG/DL (Generally 110 MG/DL)Document3 pagesTarget Range For Glycemic Control: 80-140 MG/DL (Generally 110 MG/DL)Otchi Pudtrie Wijaya100% (1)
- Hepatorenal SyndromeDocument6 pagesHepatorenal SyndromeEveline YNo ratings yet
- Nutrisi - Dr. Afiatin PDFDocument68 pagesNutrisi - Dr. Afiatin PDFekorahmanadiNo ratings yet
- Blanko PX LAB BaruDocument2 pagesBlanko PX LAB Barupus purnamaNo ratings yet
- Medical Nutrition Therap y For Gastroenterohepatology DisordersDocument61 pagesMedical Nutrition Therap y For Gastroenterohepatology DisordersFeby Tegar KsatriaNo ratings yet
- Otsuka CairanDocument60 pagesOtsuka Cairan_LipRaa_No ratings yet
- Pemeriksaan Fisik Tanda VitalDocument39 pagesPemeriksaan Fisik Tanda VitalOmHada'No ratings yet
- Electrolyte Imbalance - Handout PDFDocument23 pagesElectrolyte Imbalance - Handout PDFFaisal Ridho SaktiNo ratings yet
- Konsep EWS Di RSDocument50 pagesKonsep EWS Di RSRadenroro Atih Utari RizkyNo ratings yet
- National Clinical Guidelines For Stroke Fourth EditionDocument232 pagesNational Clinical Guidelines For Stroke Fourth EditionRosa Mabel Sanchez RoncalNo ratings yet
- Kliren Kreatinin Norepinefrin Dopamine: Rumus: (140 X Umur) X BB 72 X CRDocument2 pagesKliren Kreatinin Norepinefrin Dopamine: Rumus: (140 X Umur) X BB 72 X CRAL FI ANNo ratings yet
- Nutrisi - Dr. AfiatinDocument68 pagesNutrisi - Dr. Afiatinkhumaira1982No ratings yet
- 2.2. Anang Achmadi PENDEKATAN ASAM BASA STEWART AG KEPERAWATANDocument51 pages2.2. Anang Achmadi PENDEKATAN ASAM BASA STEWART AG KEPERAWATANTheresia Avila KurniaNo ratings yet
- Nutrisi EnteralDocument11 pagesNutrisi EnteralFirmansyah Chaniago100% (2)
- AKI & Indikasi CRRTDocument25 pagesAKI & Indikasi CRRTMaya Sari BaharumNo ratings yet
- Diabetes Mellitus: Dr. Beny Ghufron, SP - PD. SMF Penyakit Dalam Rsud DR Haryoto LumajangDocument70 pagesDiabetes Mellitus: Dr. Beny Ghufron, SP - PD. SMF Penyakit Dalam Rsud DR Haryoto LumajangDendian Berlia JelitaNo ratings yet
- Liver Cirrhosis: Dr. Rudy Dwi LaksonoDocument26 pagesLiver Cirrhosis: Dr. Rudy Dwi LaksonoMarthalena Simamora100% (1)
- Kuliah Blok Growth and DevelopmentDocument44 pagesKuliah Blok Growth and Developmentjaish8904No ratings yet
- 2019 Dr. Sumarjo GerdDocument18 pages2019 Dr. Sumarjo GerdAnnisa Ayu Nabila100% (1)
- Jurnal KMC Dan Musik LullabyDocument8 pagesJurnal KMC Dan Musik LullabyKowe Bento TenanNo ratings yet
- Farmakologi Obat Analgesik, Anti Piretik & Anti Inflamasi: Andri Tilaqza, M.Farm., AptDocument45 pagesFarmakologi Obat Analgesik, Anti Piretik & Anti Inflamasi: Andri Tilaqza, M.Farm., AptDark BlueNo ratings yet
- Gawat JantungDocument127 pagesGawat JantungSyamsul PutraNo ratings yet
- Dr. Erlieza Roosdhania, SP - PD (CKD)Document38 pagesDr. Erlieza Roosdhania, SP - PD (CKD)Pon PondNo ratings yet
- Makalah Bhom 2018 PDFDocument354 pagesMakalah Bhom 2018 PDFAndrian KHoerul Anwar SiiGogon100% (2)
- MATERI EWS PerbaikanDocument24 pagesMATERI EWS PerbaikanagusNo ratings yet
- 1.Dr - Haerani Rasyid-Simposium Prinsip Terapi Nutrisi DialisisDocument41 pages1.Dr - Haerani Rasyid-Simposium Prinsip Terapi Nutrisi DialisisZaza ZunitaNo ratings yet
- ICU Management of Acute PancreatitisDocument77 pagesICU Management of Acute PancreatitisAndriy SubieNo ratings yet
- EMERGENCIES IN DM (KAD Dan HHS)Document26 pagesEMERGENCIES IN DM (KAD Dan HHS)ozNo ratings yet
- HEICSDocument36 pagesHEICSYeli Asti100% (1)
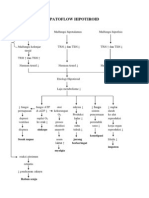
- Patoflow Hipotiroid: Sinkope Konstipasi Sesak Napas Jarang Berkeringat Impoten MyalgiaDocument1 pagePatoflow Hipotiroid: Sinkope Konstipasi Sesak Napas Jarang Berkeringat Impoten MyalgiaDessyana Paulus50% (2)
- Kelainan Esophagus & GasterDocument83 pagesKelainan Esophagus & GasterajikwaNo ratings yet
- Materi DR Rita Zahara NewDocument31 pagesMateri DR Rita Zahara NewIrfanNo ratings yet
- Askep MCI - AchirmanDocument53 pagesAskep MCI - AchirmanmarthaNo ratings yet
- PEWS Training IndonesiaDocument36 pagesPEWS Training IndonesiaBbenq Prasetyo100% (1)
- Sepsis & MOFs StudentDocument57 pagesSepsis & MOFs StudentKatherine LiNo ratings yet
- Physiology CO Guyton ModelDocument42 pagesPhysiology CO Guyton Modelcovid kojaNo ratings yet
- Nutrition in ICU: DR Rahul VarshenyDocument50 pagesNutrition in ICU: DR Rahul VarshenyAntar InenigogNo ratings yet
- Terapi CairanDocument41 pagesTerapi CairanRatu Qurroh AinNo ratings yet
- Transportation and Stabilitation in Critically Ill Patient - 2015Document36 pagesTransportation and Stabilitation in Critically Ill Patient - 2015Gustav Valentino100% (1)
- Analgesic ClassificationDocument4 pagesAnalgesic Classificationvie_apt6299No ratings yet
- Eras - Eko SDocument24 pagesEras - Eko SFerdyNo ratings yet
- TB Dan DMDocument27 pagesTB Dan DMMindiRahayuNo ratings yet
- IPDIDocument30 pagesIPDIaris budionoNo ratings yet
- Terapi Cairan Pada AnakDocument48 pagesTerapi Cairan Pada AnakAstri Novia RizqiNo ratings yet
- Titrasi Obat Emegency 28 JanuariDocument27 pagesTitrasi Obat Emegency 28 JanuariaspaNo ratings yet
- Jurnal Acute Decompensated Heart FailureDocument4 pagesJurnal Acute Decompensated Heart FailureMayang Sri WulandNo ratings yet
- Presentasi Dr. Basuki Rachmad, Sp. An. KICDocument39 pagesPresentasi Dr. Basuki Rachmad, Sp. An. KICinstalasi kamar bedah RSMINo ratings yet
- Penyakit Ginjal Kronik Dan Indikasi Dialisis DR Ratih Tri KD MAJUDocument56 pagesPenyakit Ginjal Kronik Dan Indikasi Dialisis DR Ratih Tri KD MAJUFitriana WijayatiNo ratings yet
- Response To Trauma and Metabolic Changes: Posttraumatic MetabolismDocument13 pagesResponse To Trauma and Metabolic Changes: Posttraumatic MetabolismCar OrdzNo ratings yet
- Burns ..: CA Loubser Department of Surgery University of The Free SateDocument32 pagesBurns ..: CA Loubser Department of Surgery University of The Free SateAndre LoubserNo ratings yet
- Quemados FisioDocument15 pagesQuemados FisioRoberto OrtizNo ratings yet
- Porter 2015 The Role of Exercise in The RehabilDocument14 pagesPorter 2015 The Role of Exercise in The RehabilLuisa MendozaNo ratings yet
- Metabolismo QuemaduraDocument19 pagesMetabolismo Quemaduraalan mendezNo ratings yet
- Metabolisme Dan Perubahan Fungsi Saluran Cerna, Serta Gizi Optimal Pada Perioperatif Bedah DigestifDocument57 pagesMetabolisme Dan Perubahan Fungsi Saluran Cerna, Serta Gizi Optimal Pada Perioperatif Bedah DigestifEnik GuntyastutikNo ratings yet
- Conversion DisorderDocument8 pagesConversion DisorderMaria Von ShaftNo ratings yet
- Care Plan - Patient2Document15 pagesCare Plan - Patient2jmzxmdy597No ratings yet
- Mayaderm: Indian Institute of Management Ahmedabad IIMA/BP0385Document10 pagesMayaderm: Indian Institute of Management Ahmedabad IIMA/BP0385Vamsi Vasisht50% (2)
- Traditional Medicine in Ethiopia - PDF AbbyyDocument167 pagesTraditional Medicine in Ethiopia - PDF Abbyyselemon assefaNo ratings yet
- Physical and Medical Standards: Appendix A General InstructionsDocument22 pagesPhysical and Medical Standards: Appendix A General InstructionssreyasNo ratings yet
- Sedivet 1.0% Injection: Sedative and Analgesic For HorsesDocument4 pagesSedivet 1.0% Injection: Sedative and Analgesic For HorsesandreisandorNo ratings yet
- 72 Chemical Fertilizersand Pesticidesin Indian Agriculture Effecton Human Healthand Environment Vedpriya AryaDocument17 pages72 Chemical Fertilizersand Pesticidesin Indian Agriculture Effecton Human Healthand Environment Vedpriya AryaSanchit NigamNo ratings yet
- Mitral Valve ProlapseDocument6 pagesMitral Valve ProlapseMary Joy FrancoNo ratings yet
- The Revelation of HealthDocument64 pagesThe Revelation of Healthkristinamoja100% (2)
- George M Foster and Barbara Gallatin Anderson Medical Anthropology Chichester John Wiley 1978 8vo PP X 354 Pound975Document2 pagesGeorge M Foster and Barbara Gallatin Anderson Medical Anthropology Chichester John Wiley 1978 8vo PP X 354 Pound975Hilal farooqNo ratings yet
- Muna Chemali - CVDocument4 pagesMuna Chemali - CVapi-542010683No ratings yet
- The Association Between Homocysteine Level and Balance Disorder Among Us Adults Varied in Different Sex Groups A Cross Sectional StudyDocument7 pagesThe Association Between Homocysteine Level and Balance Disorder Among Us Adults Varied in Different Sex Groups A Cross Sectional StudyHerald Scholarly Open AccessNo ratings yet
- (Human Anatomy and Physiology) Jane E. Middleton-Wound Healing - Process, Phases, and Promoting-Nova Science Publishers (2011)Document226 pages(Human Anatomy and Physiology) Jane E. Middleton-Wound Healing - Process, Phases, and Promoting-Nova Science Publishers (2011)Muhammad IrwaniNo ratings yet
- Low-Fluence 1,064-nm Laser Hair Reduction For Pseudofolliculitis Barbae in Skin Types IV, V, and VIDocument10 pagesLow-Fluence 1,064-nm Laser Hair Reduction For Pseudofolliculitis Barbae in Skin Types IV, V, and VIRada TrifonovNo ratings yet
- Pemb - Literasi Bahasa InggrisDocument13 pagesPemb - Literasi Bahasa Inggrisdani fitriyadiNo ratings yet
- ADR Reporting SystemDocument58 pagesADR Reporting SystemYash DevrukhkarNo ratings yet
- Respiratory Disorder Note BSC 3rd YearDocument41 pagesRespiratory Disorder Note BSC 3rd YearNancyNo ratings yet
- MR - Danish Haematology Haemoglobin (HB) 11.2 HaemoglobinDocument25 pagesMR - Danish Haematology Haemoglobin (HB) 11.2 Haemoglobinmaharanapratap1541No ratings yet
- To The Philosophy of The Human Person: Quarter 1 - Module 4.2: Care For The EnvironmentDocument21 pagesTo The Philosophy of The Human Person: Quarter 1 - Module 4.2: Care For The EnvironmentDustin EsguerraNo ratings yet
- Buy Tramadol 50mg TabletsDocument2 pagesBuy Tramadol 50mg TabletsSmith JackNo ratings yet
- CVP Vs Peep CorrectedDocument15 pagesCVP Vs Peep Correctedsabihul islamNo ratings yet
- Bryn Melyn Care: Business Continuity Plan 2018-2019 (This Reviewed Document Includes Reference To Brexit)Document11 pagesBryn Melyn Care: Business Continuity Plan 2018-2019 (This Reviewed Document Includes Reference To Brexit)sudeepjmNo ratings yet
- Addison & Cushing - Patho, Signs & TreatmentDocument1 pageAddison & Cushing - Patho, Signs & TreatmentVishalNo ratings yet
- PFOonDocument3 pagesPFOonInternational Medical PublisherNo ratings yet
- Ready Stock HRM CatalogueDocument4 pagesReady Stock HRM CatalogueAliabdulghaniNo ratings yet
- 1713603220englis PassageDocument6 pages1713603220englis Passageytmanny0No ratings yet
- Psoriasis Case Study by Dr. Neeraja KshirsagarDocument10 pagesPsoriasis Case Study by Dr. Neeraja KshirsagarDr Neeraja KshirsagarNo ratings yet
- Severe Symptomatic Bradycardia After Intravenous Immunoglobulin Infusion A Rare Manifestation PDFDocument4 pagesSevere Symptomatic Bradycardia After Intravenous Immunoglobulin Infusion A Rare Manifestation PDFAlvhiesBiruUlfiahAzisNo ratings yet