Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Measure It Up!: Performance Task Grade 7 - Mathematics Quarter 2Document1 pageMeasure It Up!: Performance Task Grade 7 - Mathematics Quarter 2ROSELYN SANTIAGO100% (5)
- Department of Foreign Affairs - Payment FacilityDocument1 pageDepartment of Foreign Affairs - Payment FacilityMa. Cristina TanadaNo ratings yet
- Letter To PostmasterDocument2 pagesLetter To Postmastermary100% (2)
- Negotiating With International Customers Partners and RegulatorsDocument18 pagesNegotiating With International Customers Partners and RegulatorsMirza420No ratings yet
- 2019 BIT Rare Behavior Change For Nature DigitalDocument84 pages2019 BIT Rare Behavior Change For Nature DigitalMa. Cristina TanadaNo ratings yet
- 2014 Accomplishment Report I. Executive SummaryDocument21 pages2014 Accomplishment Report I. Executive SummaryMa. Cristina TanadaNo ratings yet
- No Communities # of Families Sample HH CodingDocument1 pageNo Communities # of Families Sample HH CodingMa. Cristina TanadaNo ratings yet
- Child-Centred Multi-Risk Assessments: A Field Guide and ToolkitDocument60 pagesChild-Centred Multi-Risk Assessments: A Field Guide and ToolkitMa. Cristina TanadaNo ratings yet
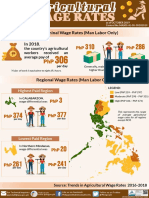
- 2018 Agricultural Wage RatesDocument1 page2018 Agricultural Wage RatesMa. Cristina TanadaNo ratings yet
- 2013 Household Survey GuideDocument34 pages2013 Household Survey GuideMa. Cristina TanadaNo ratings yet
- Prevalence and Treatment of Children Diarrhea Among Children, by Background Characteristics: 2008, 2013Document4 pagesPrevalence and Treatment of Children Diarrhea Among Children, by Background Characteristics: 2008, 2013Ma. Cristina TanadaNo ratings yet
- Proportion of 1-Year-Old Immunized Against Selected Diseases, by Background Characteristics: 2008, 2013Document3 pagesProportion of 1-Year-Old Immunized Against Selected Diseases, by Background Characteristics: 2008, 2013Ma. Cristina TanadaNo ratings yet
- Outline For Country LandscapeDocument7 pagesOutline For Country LandscapeMa. Cristina TanadaNo ratings yet
- Speechreading 101 (.1 Ceu) : 11-14-13 ASHA Conference Chicago, ILDocument47 pagesSpeechreading 101 (.1 Ceu) : 11-14-13 ASHA Conference Chicago, ILMansi DabhiNo ratings yet
- A Biomimicry Primer Janine Benyus PDFDocument10 pagesA Biomimicry Primer Janine Benyus PDFBernard CarbonNo ratings yet
- Value Stream MappingDocument40 pagesValue Stream Mappingjinyue7302No ratings yet
- Maharashtra University of Health Sciences, Nashik: II Year Post Basic B.SC NursingDocument25 pagesMaharashtra University of Health Sciences, Nashik: II Year Post Basic B.SC NursingshivaNo ratings yet
- Company ProfileDocument16 pagesCompany ProfileChu Minh Hoi100% (1)
- MadridDocument1 pageMadridscoch20No ratings yet
- Coaching Zone Logo Creative BriefDocument3 pagesCoaching Zone Logo Creative BriefsayaadalahseorangkapNo ratings yet
- CriminalisticDocument7 pagesCriminalisticJestonie DavidNo ratings yet
- Week 7 Seminar DronesDocument25 pagesWeek 7 Seminar DronesCha FraNo ratings yet
- ENG40001 Final Year Research Project 1 Semester 2, 2020: RubricsDocument8 pagesENG40001 Final Year Research Project 1 Semester 2, 2020: RubricsAS V KameshNo ratings yet
- Internal Audit PolicyDocument7 pagesInternal Audit PolicyRUBELNo ratings yet
- EF4e Pre-Int File Test 2A Answer SheetDocument1 pageEF4e Pre-Int File Test 2A Answer SheetB McNo ratings yet
- People V JumamoyDocument17 pagesPeople V JumamoyJane BiebsNo ratings yet
- 1000 Most Common Words in EnglishDocument29 pages1000 Most Common Words in EnglishSebastian ChavezNo ratings yet
- M. S. Bidve Engineering College, Latur: "Online Shopping System"Document61 pagesM. S. Bidve Engineering College, Latur: "Online Shopping System"Priti PatilNo ratings yet
- Prelim Exam EssayDocument1 pagePrelim Exam EssayKeanu PeraltaNo ratings yet
- Civil Drip IrrigationDocument11 pagesCivil Drip Irrigationmohan mohanNo ratings yet
- Noc16-Mg07 Week 04 Assignment 01Document3 pagesNoc16-Mg07 Week 04 Assignment 01Tara ReashaNo ratings yet
- Artificial Intelligence Research CenterDocument20 pagesArtificial Intelligence Research Centerpatmos666No ratings yet
- Suffolk Times Classifieds and Service Directory: June 29, 2017Document14 pagesSuffolk Times Classifieds and Service Directory: June 29, 2017TimesreviewNo ratings yet
- Clean Up Drive: Narrative ReportDocument5 pagesClean Up Drive: Narrative ReportNorie Jose100% (1)
- NBS Learning Scenario Aromatic PlantsDocument6 pagesNBS Learning Scenario Aromatic PlantsMaria Celestina Ançã HenriquesNo ratings yet
- Pragyan 08-01Document104 pagesPragyan 08-01PRAGYAN,Tinsukia CollegeNo ratings yet
- Energy and Water Conservation in Housekeeping DepartmentDocument4 pagesEnergy and Water Conservation in Housekeeping Departmentmadhu anvekarNo ratings yet
- Senior Citizen Services in PennsylvaniaDocument2 pagesSenior Citizen Services in PennsylvaniaJesse WhiteNo ratings yet
- GMP Engineering Manual Simatic Wincc v7 5 enDocument150 pagesGMP Engineering Manual Simatic Wincc v7 5 enhuykhiemNo ratings yet
- Presentation On Marketing MixDocument11 pagesPresentation On Marketing MixTriciaGay DaleyNo ratings yet