
ACL Reconstruction Using Quadriceps Tendon: HE Utting DGE
ACL Reconstruction Using Quadriceps Tendon: HE Utting DGE
You might also like
- Can't Hurt Me by David GogginsDocument5 pagesCan't Hurt Me by David GogginsInfinit1376% (17)
- Kris Gethin Shred-KM-4WRK2LEAN-FINAL PDFDocument57 pagesKris Gethin Shred-KM-4WRK2LEAN-FINAL PDFSarmad Sultan67% (3)
- Triple ArthrodesisDocument10 pagesTriple ArthrodesisdrkbarryNo ratings yet
- Journal Homepage: - : IntroductionDocument7 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Magnetic Resonance Imagination of The Peroneus Longus Tendon After Anterior Cruciate Ligament ReconstructionDocument5 pagesMagnetic Resonance Imagination of The Peroneus Longus Tendon After Anterior Cruciate Ligament Reconstructionfebyan yohanesNo ratings yet
- V1 PLCDocument18 pagesV1 PLCBartoszNo ratings yet
- Tibiotalocalcaneal Arthrodesis With Intramedullary Fibular Strut Graft and Adjuvant Hardware FixationDocument3 pagesTibiotalocalcaneal Arthrodesis With Intramedullary Fibular Strut Graft and Adjuvant Hardware Fixationvijaypatel4282No ratings yet
- A Modified Direct Lateral Approach in Total Hip ArthroplastyDocument5 pagesA Modified Direct Lateral Approach in Total Hip ArthroplastyAbhishek JirelNo ratings yet
- Arthroscopic Biceps Tenodesis: Operative Technique: Technical NoteDocument3 pagesArthroscopic Biceps Tenodesis: Operative Technique: Technical NoteDaulay AldyNo ratings yet
- Functional Outcomes of Nonunion Scaphoid Fracture Treated by PDFDocument6 pagesFunctional Outcomes of Nonunion Scaphoid Fracture Treated by PDFHazorthoNo ratings yet
- Suchenski 1992Document6 pagesSuchenski 1992piyush joshiNo ratings yet
- Quads ReconDocument7 pagesQuads ReconNuno PaisNo ratings yet
- Jurnal Reading WirdahDocument17 pagesJurnal Reading Wirdahwirdah ulfahaini m.No ratings yet
- PCL AvulsionDocument4 pagesPCL Avulsionharpreet singhNo ratings yet
- Gust Ke 2005Document4 pagesGust Ke 2005Akshay DudhanaleNo ratings yet
- Total Elbow TechniqueDocument7 pagesTotal Elbow Techniquedidit satmokoNo ratings yet
- Arthroscopic Fixation of Anterior Cruciate Ligament Tibial Avulsion Fractures Using Fibre Wire With EndobuttonDocument6 pagesArthroscopic Fixation of Anterior Cruciate Ligament Tibial Avulsion Fractures Using Fibre Wire With EndobuttonQamar AzeezNo ratings yet
- Knee Disarticulation Versus Above-Knee Amputation : Balgrist Orthopaedic Hospital, University of ZurichDocument5 pagesKnee Disarticulation Versus Above-Knee Amputation : Balgrist Orthopaedic Hospital, University of ZurichAlfred JacksonNo ratings yet
- Allogreftfehm 2010Document8 pagesAllogreftfehm 2010Gökhan PehlivanoğluNo ratings yet
- The Proximally Based Sural Artery Flap For Coverage of Soft Tissue Defects Around The Knee and On The Proximal Third and Middle Third of The Lower LegDocument7 pagesThe Proximally Based Sural Artery Flap For Coverage of Soft Tissue Defects Around The Knee and On The Proximal Third and Middle Third of The Lower LegMarco Antonio MiraveteNo ratings yet
- Azar 2003 Otsm Repair of Acute Distal Biceps Tendon RuptureDocument4 pagesAzar 2003 Otsm Repair of Acute Distal Biceps Tendon RuptureKuozram No MasNo ratings yet
- Evolution in ACL Autograft Harvesting Techniques .3Document8 pagesEvolution in ACL Autograft Harvesting Techniques .3cooperorthopaedicsNo ratings yet
- Anatomy of IER Review 2016Document6 pagesAnatomy of IER Review 2016Ahmed MortadaNo ratings yet
- Operative Approaches For Total HipDocument9 pagesOperative Approaches For Total HipEduardo GonzalezNo ratings yet
- Acl Recon With BPT GraftDocument6 pagesAcl Recon With BPT Graftpaper coe medanNo ratings yet
- Arthroscopic Treatment of Synovial Chondromatosis of The Proximal Tibiofibular JointDocument5 pagesArthroscopic Treatment of Synovial Chondromatosis of The Proximal Tibiofibular JointAnonymous cbu3AWeTBNo ratings yet
- Functional Free Muscle Transfer For BPIDocument7 pagesFunctional Free Muscle Transfer For BPIshininghmNo ratings yet
- Postoperative KneeDocument15 pagesPostoperative Kneeradiology residentsNo ratings yet
- 1 s2.0 S2212628721002589 MainDocument6 pages1 s2.0 S2212628721002589 MainEvans JohnNo ratings yet
- Mini Open Arthroscopically Assisted BrisDocument6 pagesMini Open Arthroscopically Assisted BrisBruno EstevesNo ratings yet
- Journal of Orthopaedic Surgery and ResearchDocument6 pagesJournal of Orthopaedic Surgery and ResearchDewye SartikaNo ratings yet
- True Ponte Osteotomy Ponte 2018Document10 pagesTrue Ponte Osteotomy Ponte 2018Azmi FarhadiNo ratings yet
- Bilimsel Makale Cerrahi GirişimDocument3 pagesBilimsel Makale Cerrahi GirişimBelizNo ratings yet
- J Jhsa 2014 12 025Document9 pagesJ Jhsa 2014 12 025Izan BallesterosNo ratings yet
- Percutaneous Femoral Derotational Osteotomy For Excessive Femoral TorsionDocument7 pagesPercutaneous Femoral Derotational Osteotomy For Excessive Femoral TorsionDouglas PrinaNo ratings yet
- The Optimum Temporo-Mandibular Joint Condyle Position in Clinical Practice.Document26 pagesThe Optimum Temporo-Mandibular Joint Condyle Position in Clinical Practice.Jose L LlanosNo ratings yet
- Locking T-Plate Repair of Ilial Fractures in Cats and Small DogsDocument8 pagesLocking T-Plate Repair of Ilial Fractures in Cats and Small DogsNayra Cristina Herreira do ValleNo ratings yet
- Arthroscopic-Assisted Pectoralis Minor Transfer For Irreparable Anterosuperior Massive Rotator Cuff TearDocument6 pagesArthroscopic-Assisted Pectoralis Minor Transfer For Irreparable Anterosuperior Massive Rotator Cuff TearGabriel Arturo Lorca OsorioNo ratings yet
- Reconstruction of A Ruptured Patellar TendonDocument5 pagesReconstruction of A Ruptured Patellar Tendonmarcelogascon.oNo ratings yet
- Patellar Tendon or Semitendinosus Tendon Autografts For Anterior Cruciate Ligament Reconstruction?Document7 pagesPatellar Tendon or Semitendinosus Tendon Autografts For Anterior Cruciate Ligament Reconstruction?lipemagalhaesNo ratings yet
- Successful Outcome With Minimally Invasive Plate Osteosynthesis For Periprosthetic Tibial Fracture After Total Knee ArthroplastyDocument6 pagesSuccessful Outcome With Minimally Invasive Plate Osteosynthesis For Periprosthetic Tibial Fracture After Total Knee ArthroplastyMohebNo ratings yet
- Hip AssessDocument6 pagesHip AssessAhmed SalmanNo ratings yet
- Kartus 2001Document10 pagesKartus 2001Waldo Luis González DuqueNo ratings yet
- PIIS2212628715002169Document6 pagesPIIS2212628715002169ich khuyNo ratings yet
- 4 in 1 Quadricepsplasty For Fixed and Habitual DisDocument8 pages4 in 1 Quadricepsplasty For Fixed and Habitual DisMinh ChíNo ratings yet
- 17/09/13 11:14 PM //transtibial (Below-Knee) AmputationsDocument7 pages17/09/13 11:14 PM //transtibial (Below-Knee) AmputationscmonmanNo ratings yet
- Using A Trevira TubeDocument8 pagesUsing A Trevira TubebranislavNo ratings yet
- 1 s2.0 S2212628721000864 MainDocument5 pages1 s2.0 S2212628721000864 MainLuthfi LazuardiNo ratings yet
- Orthopedic Nursing. Lecture Notes at Philipine Orthopedic CenterDocument7 pagesOrthopedic Nursing. Lecture Notes at Philipine Orthopedic Centerhannjazz100% (5)
- Prepared By:: Ma. Kristina G. CristobalDocument17 pagesPrepared By:: Ma. Kristina G. CristobalDiovy TahilanNo ratings yet
- Anatomy and Bio Mechanics of The KneeDocument15 pagesAnatomy and Bio Mechanics of The KneeaimanshalpyNo ratings yet
- PM TearDocument6 pagesPM TearPiotrek PłotkaNo ratings yet
- TKA Scope Arthrolysis Knee Surg Sports Traumatol Arthrosc 2010 Mar 18 (3) 346-351Document6 pagesTKA Scope Arthrolysis Knee Surg Sports Traumatol Arthrosc 2010 Mar 18 (3) 346-351Fayza RihastaraNo ratings yet
- Medial Patellofemoral Ligament Reconstruction Camanho TechniqueDocument5 pagesMedial Patellofemoral Ligament Reconstruction Camanho TechniqueRe DiazNo ratings yet
- Long Head Biceps Tendondnatural Patch For Massive Irreparable Rotator Cuff TearsDocument6 pagesLong Head Biceps Tendondnatural Patch For Massive Irreparable Rotator Cuff TearsDita Putri DamayantiNo ratings yet
- Anterior Approach For Total Hip Arthroplasty Beyond The Minimally Invasive TechniqueDocument7 pagesAnterior Approach For Total Hip Arthroplasty Beyond The Minimally Invasive Technique阿欧有怪兽No ratings yet
- Anterior Cable Reconstruction Using Autologous Long Head of The Biceps Tendon For Massive Irreparable Rotator Cuff TearsDocument11 pagesAnterior Cable Reconstruction Using Autologous Long Head of The Biceps Tendon For Massive Irreparable Rotator Cuff TearsjulioNo ratings yet
- Morphological Study of Plantaris Muscle PDFDocument3 pagesMorphological Study of Plantaris Muscle PDFcoco2000No ratings yet
- The Anatomical Foundations of Regional Anesthesia and Acute Pain MedicineFrom EverandThe Anatomical Foundations of Regional Anesthesia and Acute Pain MedicineNo ratings yet
- Module 2 Project Gap Analysis Strategy For Team #3Document20 pagesModule 2 Project Gap Analysis Strategy For Team #3Mary A. Dillard100% (2)
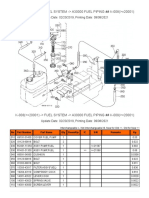
- K-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Document2 pagesK-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Martin LindbergNo ratings yet
- How To Configure The FTP Gateway ServiceDocument3 pagesHow To Configure The FTP Gateway Servicenmhung1097No ratings yet
- Aboriginal Cultural Competence 2008Document58 pagesAboriginal Cultural Competence 2008noddyNo ratings yet
- Timing Protection in AUTOSAR ISO 26262Document10 pagesTiming Protection in AUTOSAR ISO 26262Joseph KymmNo ratings yet
- Chemistry Ibdp Exam Syle QuestionsDocument37 pagesChemistry Ibdp Exam Syle QuestionsGEORGE MATTHEWNo ratings yet
- Clinical Liver Disease - 2022 - Memel - Intermittent Fasting As A Treatment For Nonalcoholic Fatty Liver Disease What IsDocument5 pagesClinical Liver Disease - 2022 - Memel - Intermittent Fasting As A Treatment For Nonalcoholic Fatty Liver Disease What Isarranguezjr5991No ratings yet
- Transverse Lie : Predisposing Factors, Maternal and Perinatal OutcomeDocument4 pagesTransverse Lie : Predisposing Factors, Maternal and Perinatal OutcomeErlangga DayudNo ratings yet
- Communication and Ethics in Pharmacy Practice: What Is To BeDocument23 pagesCommunication and Ethics in Pharmacy Practice: What Is To BeMuhammad RezaNo ratings yet
- Los Angeles Times 0831Document28 pagesLos Angeles Times 0831vlNo ratings yet
- Roach PreviewDocument14 pagesRoach PreviewDomênico GayNo ratings yet
- Consol P 200heDocument2 pagesConsol P 200heimmanuel lumbantobingNo ratings yet
- Standard Muster List: NYK SMS Manual (Rev:2020/01/01)Document2 pagesStandard Muster List: NYK SMS Manual (Rev:2020/01/01)Cleanard HidalgoNo ratings yet
- P - Chapter 7Document17 pagesP - Chapter 7usa2017lapNo ratings yet
- Mnemonics For Block 3Document3 pagesMnemonics For Block 3sahana2791No ratings yet
- The Internet Addiction and The Academic Productivity of Grade 12 Students in Aclc OrmocDocument43 pagesThe Internet Addiction and The Academic Productivity of Grade 12 Students in Aclc OrmocKenberly DingleNo ratings yet
- Analette Manual Service Rev. D 2-6-08Document149 pagesAnalette Manual Service Rev. D 2-6-08RosanaCriolloNo ratings yet
- Heart DiseaseDocument88 pagesHeart DiseaseBruce Lawrence MadeirosNo ratings yet
- Ipsative Personality TestsDocument10 pagesIpsative Personality Testseman_tenan2220No ratings yet
- Sample ReviewDocument5 pagesSample Reviewdawit gebreyohansNo ratings yet
- The Science Behind AspirinDocument14 pagesThe Science Behind AspirindipetNo ratings yet
- TLE Cookery10 Q4 W3 V4Document7 pagesTLE Cookery10 Q4 W3 V4Maria Rose Tariga Aquino100% (2)
- Sma Negeri 1 Pare: Understanding Descriptive TextDocument13 pagesSma Negeri 1 Pare: Understanding Descriptive TextAnnisa FujiantiNo ratings yet
- DRRR2324 Q4 DRRDocument7 pagesDRRR2324 Q4 DRRh4gtg7n55gNo ratings yet
- OutbreakWksht UpdatedMay18 ADocument3 pagesOutbreakWksht UpdatedMay18 ASatya DwiparthaNo ratings yet
- ERBEJETDocument8 pagesERBEJETHossain TanjilaaNo ratings yet
- Activity No. 2 Disaster RiskDocument3 pagesActivity No. 2 Disaster RiskBUENAVENTURA, GABRIEL JOVANNo ratings yet
- Calibration of Dosimeters Used in Radiation TherapyDocument122 pagesCalibration of Dosimeters Used in Radiation TherapySOHON SINHA MAHAPATRANo ratings yet
























































































Download as pdf or txt
You might also like
- Can't Hurt Me by David GogginsDocument5 pagesCan't Hurt Me by David GogginsInfinit1376% (17)
- Kris Gethin Shred-KM-4WRK2LEAN-FINAL PDFDocument57 pagesKris Gethin Shred-KM-4WRK2LEAN-FINAL PDFSarmad Sultan67% (3)
- Triple ArthrodesisDocument10 pagesTriple ArthrodesisdrkbarryNo ratings yet
- Journal Homepage: - : IntroductionDocument7 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Magnetic Resonance Imagination of The Peroneus Longus Tendon After Anterior Cruciate Ligament ReconstructionDocument5 pagesMagnetic Resonance Imagination of The Peroneus Longus Tendon After Anterior Cruciate Ligament Reconstructionfebyan yohanesNo ratings yet
- V1 PLCDocument18 pagesV1 PLCBartoszNo ratings yet
- Tibiotalocalcaneal Arthrodesis With Intramedullary Fibular Strut Graft and Adjuvant Hardware FixationDocument3 pagesTibiotalocalcaneal Arthrodesis With Intramedullary Fibular Strut Graft and Adjuvant Hardware Fixationvijaypatel4282No ratings yet
- A Modified Direct Lateral Approach in Total Hip ArthroplastyDocument5 pagesA Modified Direct Lateral Approach in Total Hip ArthroplastyAbhishek JirelNo ratings yet
- Arthroscopic Biceps Tenodesis: Operative Technique: Technical NoteDocument3 pagesArthroscopic Biceps Tenodesis: Operative Technique: Technical NoteDaulay AldyNo ratings yet
- Functional Outcomes of Nonunion Scaphoid Fracture Treated by PDFDocument6 pagesFunctional Outcomes of Nonunion Scaphoid Fracture Treated by PDFHazorthoNo ratings yet
- Suchenski 1992Document6 pagesSuchenski 1992piyush joshiNo ratings yet
- Quads ReconDocument7 pagesQuads ReconNuno PaisNo ratings yet
- Jurnal Reading WirdahDocument17 pagesJurnal Reading Wirdahwirdah ulfahaini m.No ratings yet
- PCL AvulsionDocument4 pagesPCL Avulsionharpreet singhNo ratings yet
- Gust Ke 2005Document4 pagesGust Ke 2005Akshay DudhanaleNo ratings yet
- Total Elbow TechniqueDocument7 pagesTotal Elbow Techniquedidit satmokoNo ratings yet
- Arthroscopic Fixation of Anterior Cruciate Ligament Tibial Avulsion Fractures Using Fibre Wire With EndobuttonDocument6 pagesArthroscopic Fixation of Anterior Cruciate Ligament Tibial Avulsion Fractures Using Fibre Wire With EndobuttonQamar AzeezNo ratings yet
- Knee Disarticulation Versus Above-Knee Amputation : Balgrist Orthopaedic Hospital, University of ZurichDocument5 pagesKnee Disarticulation Versus Above-Knee Amputation : Balgrist Orthopaedic Hospital, University of ZurichAlfred JacksonNo ratings yet
- Allogreftfehm 2010Document8 pagesAllogreftfehm 2010Gökhan PehlivanoğluNo ratings yet
- The Proximally Based Sural Artery Flap For Coverage of Soft Tissue Defects Around The Knee and On The Proximal Third and Middle Third of The Lower LegDocument7 pagesThe Proximally Based Sural Artery Flap For Coverage of Soft Tissue Defects Around The Knee and On The Proximal Third and Middle Third of The Lower LegMarco Antonio MiraveteNo ratings yet
- Azar 2003 Otsm Repair of Acute Distal Biceps Tendon RuptureDocument4 pagesAzar 2003 Otsm Repair of Acute Distal Biceps Tendon RuptureKuozram No MasNo ratings yet
- Evolution in ACL Autograft Harvesting Techniques .3Document8 pagesEvolution in ACL Autograft Harvesting Techniques .3cooperorthopaedicsNo ratings yet
- Anatomy of IER Review 2016Document6 pagesAnatomy of IER Review 2016Ahmed MortadaNo ratings yet
- Operative Approaches For Total HipDocument9 pagesOperative Approaches For Total HipEduardo GonzalezNo ratings yet
- Acl Recon With BPT GraftDocument6 pagesAcl Recon With BPT Graftpaper coe medanNo ratings yet
- Arthroscopic Treatment of Synovial Chondromatosis of The Proximal Tibiofibular JointDocument5 pagesArthroscopic Treatment of Synovial Chondromatosis of The Proximal Tibiofibular JointAnonymous cbu3AWeTBNo ratings yet
- Functional Free Muscle Transfer For BPIDocument7 pagesFunctional Free Muscle Transfer For BPIshininghmNo ratings yet
- Postoperative KneeDocument15 pagesPostoperative Kneeradiology residentsNo ratings yet
- 1 s2.0 S2212628721002589 MainDocument6 pages1 s2.0 S2212628721002589 MainEvans JohnNo ratings yet
- Mini Open Arthroscopically Assisted BrisDocument6 pagesMini Open Arthroscopically Assisted BrisBruno EstevesNo ratings yet
- Journal of Orthopaedic Surgery and ResearchDocument6 pagesJournal of Orthopaedic Surgery and ResearchDewye SartikaNo ratings yet
- True Ponte Osteotomy Ponte 2018Document10 pagesTrue Ponte Osteotomy Ponte 2018Azmi FarhadiNo ratings yet
- Bilimsel Makale Cerrahi GirişimDocument3 pagesBilimsel Makale Cerrahi GirişimBelizNo ratings yet
- J Jhsa 2014 12 025Document9 pagesJ Jhsa 2014 12 025Izan BallesterosNo ratings yet
- Percutaneous Femoral Derotational Osteotomy For Excessive Femoral TorsionDocument7 pagesPercutaneous Femoral Derotational Osteotomy For Excessive Femoral TorsionDouglas PrinaNo ratings yet
- The Optimum Temporo-Mandibular Joint Condyle Position in Clinical Practice.Document26 pagesThe Optimum Temporo-Mandibular Joint Condyle Position in Clinical Practice.Jose L LlanosNo ratings yet
- Locking T-Plate Repair of Ilial Fractures in Cats and Small DogsDocument8 pagesLocking T-Plate Repair of Ilial Fractures in Cats and Small DogsNayra Cristina Herreira do ValleNo ratings yet
- Arthroscopic-Assisted Pectoralis Minor Transfer For Irreparable Anterosuperior Massive Rotator Cuff TearDocument6 pagesArthroscopic-Assisted Pectoralis Minor Transfer For Irreparable Anterosuperior Massive Rotator Cuff TearGabriel Arturo Lorca OsorioNo ratings yet
- Reconstruction of A Ruptured Patellar TendonDocument5 pagesReconstruction of A Ruptured Patellar Tendonmarcelogascon.oNo ratings yet
- Patellar Tendon or Semitendinosus Tendon Autografts For Anterior Cruciate Ligament Reconstruction?Document7 pagesPatellar Tendon or Semitendinosus Tendon Autografts For Anterior Cruciate Ligament Reconstruction?lipemagalhaesNo ratings yet
- Successful Outcome With Minimally Invasive Plate Osteosynthesis For Periprosthetic Tibial Fracture After Total Knee ArthroplastyDocument6 pagesSuccessful Outcome With Minimally Invasive Plate Osteosynthesis For Periprosthetic Tibial Fracture After Total Knee ArthroplastyMohebNo ratings yet
- Hip AssessDocument6 pagesHip AssessAhmed SalmanNo ratings yet
- Kartus 2001Document10 pagesKartus 2001Waldo Luis González DuqueNo ratings yet
- PIIS2212628715002169Document6 pagesPIIS2212628715002169ich khuyNo ratings yet
- 4 in 1 Quadricepsplasty For Fixed and Habitual DisDocument8 pages4 in 1 Quadricepsplasty For Fixed and Habitual DisMinh ChíNo ratings yet
- 17/09/13 11:14 PM //transtibial (Below-Knee) AmputationsDocument7 pages17/09/13 11:14 PM //transtibial (Below-Knee) AmputationscmonmanNo ratings yet
- Using A Trevira TubeDocument8 pagesUsing A Trevira TubebranislavNo ratings yet
- 1 s2.0 S2212628721000864 MainDocument5 pages1 s2.0 S2212628721000864 MainLuthfi LazuardiNo ratings yet
- Orthopedic Nursing. Lecture Notes at Philipine Orthopedic CenterDocument7 pagesOrthopedic Nursing. Lecture Notes at Philipine Orthopedic Centerhannjazz100% (5)
- Prepared By:: Ma. Kristina G. CristobalDocument17 pagesPrepared By:: Ma. Kristina G. CristobalDiovy TahilanNo ratings yet
- Anatomy and Bio Mechanics of The KneeDocument15 pagesAnatomy and Bio Mechanics of The KneeaimanshalpyNo ratings yet
- PM TearDocument6 pagesPM TearPiotrek PłotkaNo ratings yet
- TKA Scope Arthrolysis Knee Surg Sports Traumatol Arthrosc 2010 Mar 18 (3) 346-351Document6 pagesTKA Scope Arthrolysis Knee Surg Sports Traumatol Arthrosc 2010 Mar 18 (3) 346-351Fayza RihastaraNo ratings yet
- Medial Patellofemoral Ligament Reconstruction Camanho TechniqueDocument5 pagesMedial Patellofemoral Ligament Reconstruction Camanho TechniqueRe DiazNo ratings yet
- Long Head Biceps Tendondnatural Patch For Massive Irreparable Rotator Cuff TearsDocument6 pagesLong Head Biceps Tendondnatural Patch For Massive Irreparable Rotator Cuff TearsDita Putri DamayantiNo ratings yet
- Anterior Approach For Total Hip Arthroplasty Beyond The Minimally Invasive TechniqueDocument7 pagesAnterior Approach For Total Hip Arthroplasty Beyond The Minimally Invasive Technique阿欧有怪兽No ratings yet
- Anterior Cable Reconstruction Using Autologous Long Head of The Biceps Tendon For Massive Irreparable Rotator Cuff TearsDocument11 pagesAnterior Cable Reconstruction Using Autologous Long Head of The Biceps Tendon For Massive Irreparable Rotator Cuff TearsjulioNo ratings yet
- Morphological Study of Plantaris Muscle PDFDocument3 pagesMorphological Study of Plantaris Muscle PDFcoco2000No ratings yet
- The Anatomical Foundations of Regional Anesthesia and Acute Pain MedicineFrom EverandThe Anatomical Foundations of Regional Anesthesia and Acute Pain MedicineNo ratings yet
- Module 2 Project Gap Analysis Strategy For Team #3Document20 pagesModule 2 Project Gap Analysis Strategy For Team #3Mary A. Dillard100% (2)
- K-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Document2 pagesK-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Martin LindbergNo ratings yet
- How To Configure The FTP Gateway ServiceDocument3 pagesHow To Configure The FTP Gateway Servicenmhung1097No ratings yet
- Aboriginal Cultural Competence 2008Document58 pagesAboriginal Cultural Competence 2008noddyNo ratings yet
- Timing Protection in AUTOSAR ISO 26262Document10 pagesTiming Protection in AUTOSAR ISO 26262Joseph KymmNo ratings yet
- Chemistry Ibdp Exam Syle QuestionsDocument37 pagesChemistry Ibdp Exam Syle QuestionsGEORGE MATTHEWNo ratings yet
- Clinical Liver Disease - 2022 - Memel - Intermittent Fasting As A Treatment For Nonalcoholic Fatty Liver Disease What IsDocument5 pagesClinical Liver Disease - 2022 - Memel - Intermittent Fasting As A Treatment For Nonalcoholic Fatty Liver Disease What Isarranguezjr5991No ratings yet
- Transverse Lie : Predisposing Factors, Maternal and Perinatal OutcomeDocument4 pagesTransverse Lie : Predisposing Factors, Maternal and Perinatal OutcomeErlangga DayudNo ratings yet
- Communication and Ethics in Pharmacy Practice: What Is To BeDocument23 pagesCommunication and Ethics in Pharmacy Practice: What Is To BeMuhammad RezaNo ratings yet
- Los Angeles Times 0831Document28 pagesLos Angeles Times 0831vlNo ratings yet
- Roach PreviewDocument14 pagesRoach PreviewDomênico GayNo ratings yet
- Consol P 200heDocument2 pagesConsol P 200heimmanuel lumbantobingNo ratings yet
- Standard Muster List: NYK SMS Manual (Rev:2020/01/01)Document2 pagesStandard Muster List: NYK SMS Manual (Rev:2020/01/01)Cleanard HidalgoNo ratings yet
- P - Chapter 7Document17 pagesP - Chapter 7usa2017lapNo ratings yet
- Mnemonics For Block 3Document3 pagesMnemonics For Block 3sahana2791No ratings yet
- The Internet Addiction and The Academic Productivity of Grade 12 Students in Aclc OrmocDocument43 pagesThe Internet Addiction and The Academic Productivity of Grade 12 Students in Aclc OrmocKenberly DingleNo ratings yet
- Analette Manual Service Rev. D 2-6-08Document149 pagesAnalette Manual Service Rev. D 2-6-08RosanaCriolloNo ratings yet
- Heart DiseaseDocument88 pagesHeart DiseaseBruce Lawrence MadeirosNo ratings yet
- Ipsative Personality TestsDocument10 pagesIpsative Personality Testseman_tenan2220No ratings yet
- Sample ReviewDocument5 pagesSample Reviewdawit gebreyohansNo ratings yet
- The Science Behind AspirinDocument14 pagesThe Science Behind AspirindipetNo ratings yet
- TLE Cookery10 Q4 W3 V4Document7 pagesTLE Cookery10 Q4 W3 V4Maria Rose Tariga Aquino100% (2)
- Sma Negeri 1 Pare: Understanding Descriptive TextDocument13 pagesSma Negeri 1 Pare: Understanding Descriptive TextAnnisa FujiantiNo ratings yet
- DRRR2324 Q4 DRRDocument7 pagesDRRR2324 Q4 DRRh4gtg7n55gNo ratings yet
- OutbreakWksht UpdatedMay18 ADocument3 pagesOutbreakWksht UpdatedMay18 ASatya DwiparthaNo ratings yet
- ERBEJETDocument8 pagesERBEJETHossain TanjilaaNo ratings yet
- Activity No. 2 Disaster RiskDocument3 pagesActivity No. 2 Disaster RiskBUENAVENTURA, GABRIEL JOVANNo ratings yet
- Calibration of Dosimeters Used in Radiation TherapyDocument122 pagesCalibration of Dosimeters Used in Radiation TherapySOHON SINHA MAHAPATRANo ratings yet