Download as pdf or txt
You might also like
- Lifestyle DiseasesDocument44 pagesLifestyle Diseaseskyro draxNo ratings yet
- HIV Practice TestDocument2 pagesHIV Practice TestJoslyn GrossNo ratings yet
- What Is A Gallbladder?: Recommended Diet For Gallbladder DiseaseDocument3 pagesWhat Is A Gallbladder?: Recommended Diet For Gallbladder DiseaseIam SriNo ratings yet
- A Quick Guide To MudrasDocument13 pagesA Quick Guide To MudrasKishoreBijja95% (21)
- Abg PPT NewDocument69 pagesAbg PPT NewMalaka Atapattu100% (3)
- ABG AnalysisDocument21 pagesABG Analysismrs_jrufusNo ratings yet
- Blood CollectionDocument22 pagesBlood CollectionMegbaruNo ratings yet
- 2 Acid-Base ImbalanceDocument9 pages2 Acid-Base ImbalanceKhuzema SaeedNo ratings yet
- Liver Function Test: Prepared By: Siti Norhaiza Binti HadzirDocument33 pagesLiver Function Test: Prepared By: Siti Norhaiza Binti Hadzirmhafiziab100% (1)
- Acid Base DisordersDocument5 pagesAcid Base DisordersjohnshenryNo ratings yet
- 2 Renal PhysiologyDocument56 pages2 Renal PhysiologyNoraine Princess TabangcoraNo ratings yet
- Acid-Base Homeostasis: Dr. Abeer KhurshidDocument42 pagesAcid-Base Homeostasis: Dr. Abeer Khurshidسلة فواكة100% (2)
- Plasma ProteinDocument79 pagesPlasma ProteinnadieNo ratings yet
- Approach To The Child With Metabolic Acidosis - UDocument3 pagesApproach To The Child With Metabolic Acidosis - URishi Shrestha100% (1)
- Bleeding Disorders: LCDR Art GeorgeDocument54 pagesBleeding Disorders: LCDR Art Georgesatya_mdsNo ratings yet
- Acid-Base BalanceDocument28 pagesAcid-Base Balanceps4only100% (1)
- Assessment of Metabolic AcidosisDocument34 pagesAssessment of Metabolic Acidosisfatha100% (1)
- Abg Analysis and InterpretationDocument27 pagesAbg Analysis and InterpretationvaishnaviNo ratings yet
- Clinical SignificanceDocument31 pagesClinical Significancejav israelNo ratings yet
- Acidification of UrineDocument30 pagesAcidification of UrineNanditha SureshNo ratings yet
- Isotonic Saline (0.9%Nacl-Normal Saline) IndicationDocument3 pagesIsotonic Saline (0.9%Nacl-Normal Saline) IndicationJared AllenNo ratings yet
- Hormonal Control of Calcium and Phosphate MetabolismDocument50 pagesHormonal Control of Calcium and Phosphate MetabolismhamidNo ratings yet
- Diabetic Ketoacidosis (DKA) - Presentation Slide EditedDocument22 pagesDiabetic Ketoacidosis (DKA) - Presentation Slide EditedTerence Chin0% (1)
- Disorders of Lipid Metabolism LectureDocument55 pagesDisorders of Lipid Metabolism LectureRichard SiahaanNo ratings yet
- Case Histo PDFDocument19 pagesCase Histo PDFsomayya waliNo ratings yet
- Renal Regulation of Acid-Base BalanceDocument10 pagesRenal Regulation of Acid-Base BalanceMarianela Vásquez ArayaNo ratings yet
- Potassium HomeostasisDocument47 pagesPotassium HomeostasisMayuresh ChaudhariNo ratings yet
- Principles of Fluid Therapy On The Basis ofDocument29 pagesPrinciples of Fluid Therapy On The Basis ofhendrytzNo ratings yet
- Study GuideDocument43 pagesStudy GuideWahaj Mujahid100% (1)
- Acid Base Balance PhysiologyDocument49 pagesAcid Base Balance PhysiologyDarshini Nagarajan100% (1)
- Genpath 04 - RENAL LABORATORY TESTS - ppt.MEd 2016 (Ninaarajade's Conflicted Copy 2016-10-29) (ASUS's Conflicted Copy 2016-11-14)Document67 pagesGenpath 04 - RENAL LABORATORY TESTS - ppt.MEd 2016 (Ninaarajade's Conflicted Copy 2016-10-29) (ASUS's Conflicted Copy 2016-11-14)RjDNo ratings yet
- Approach To Chronic DiarrheaDocument40 pagesApproach To Chronic DiarrheaJheng-Dao YangNo ratings yet
- Git Notes in ShortDocument13 pagesGit Notes in ShortNeville212No ratings yet
- Balamand Faculty of MedicineDocument32 pagesBalamand Faculty of MedicineAnonymous 5FtD4bONo ratings yet
- Could Be Used in Clinical or LabDocument18 pagesCould Be Used in Clinical or Labkatrinasd100% (1)
- Henoch Schönlein PurpuraDocument12 pagesHenoch Schönlein PurpuraRavania Rahadian Putri100% (1)
- Acid Base BalanceDocument35 pagesAcid Base BalanceDhanasvi Dessai100% (1)
- Disorders of Calcium and Phosphate MetabolismDocument20 pagesDisorders of Calcium and Phosphate MetabolismThirupathi Jakkani100% (1)
- Acid Base Balance PSN LHRDocument63 pagesAcid Base Balance PSN LHRPooran Kumar100% (2)
- Bohr Effect: Carbon DioxideDocument2 pagesBohr Effect: Carbon DioxideTiToNo ratings yet
- Tubulointerstitial Diseases: Dr. Raid JastaniaDocument48 pagesTubulointerstitial Diseases: Dr. Raid JastaniaThomas McconnellNo ratings yet
- Kerosene PoisoningDocument12 pagesKerosene PoisoningTheRHIC21No ratings yet
- Arterialbloodgasanalysis ppt-2Document43 pagesArterialbloodgasanalysis ppt-2Kresna Dharma SuryanaNo ratings yet
- Embryology and Development of KidneyDocument75 pagesEmbryology and Development of Kidneyranjitha sraateNo ratings yet
- BufferDocument17 pagesBufferNandita BasakNo ratings yet
- MCQ QuestionsDocument2 pagesMCQ QuestionsShriyans JainNo ratings yet
- Arterial Blood Gases - UpToDateDocument20 pagesArterial Blood Gases - UpToDateGuillermo MárquezNo ratings yet
- MCI FMGE Previous Year Solved Question Paper 2005 MarchDocument0 pagesMCI FMGE Previous Year Solved Question Paper 2005 MarchSharat Chandra0% (1)
- Metabolism of HemeDocument138 pagesMetabolism of HemeZafir MonNo ratings yet
- Mendelson's SyndromeDocument17 pagesMendelson's SyndromeYuvetha IndranNo ratings yet
- Spotters-Mlt Paper-1: Dr.S.Rashmi Dept of BiochemistryDocument22 pagesSpotters-Mlt Paper-1: Dr.S.Rashmi Dept of BiochemistrySamuvelrajNo ratings yet
- Renal PathologyDocument28 pagesRenal PathologyApril Deveras JudillaNo ratings yet
- Blood Supply of AbdomenDocument30 pagesBlood Supply of AbdomenShadowStormNo ratings yet
- Introduction To HematologyDocument95 pagesIntroduction To HematologyAhmad Farhan Hassan0% (1)
- Ketone BodiesDocument16 pagesKetone BodiesAsim Ali100% (1)
- Nephrotic SyndromeDocument34 pagesNephrotic SyndromeAnusikta PandaNo ratings yet
- BiochemistryDocument135 pagesBiochemistryPradip Hamal100% (1)
- Urine Dipstick Testing + Common Renal Problem 2012Document52 pagesUrine Dipstick Testing + Common Renal Problem 2012Ainul ArinaNo ratings yet
- MCQ GitDocument15 pagesMCQ Gitpriya009100% (1)
- Lung Development Biological and Clinical Perspectives: Biochemistry and PhysiologyFrom EverandLung Development Biological and Clinical Perspectives: Biochemistry and PhysiologyPhilip FarrellNo ratings yet
- Lung Metabolism: Proteolysis and Antioproteolysis Biochemical Pharmacology Handling of Bioactive SubstancesFrom EverandLung Metabolism: Proteolysis and Antioproteolysis Biochemical Pharmacology Handling of Bioactive SubstancesAlain JunodNo ratings yet
- Hepatorenal Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHepatorenal Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Asthma in the 21st Century: New Research AdvancesFrom EverandAsthma in the 21st Century: New Research AdvancesRachel NadifNo ratings yet
- Predictive Analytics: A Case Study in Machine-Learning and Claims DatabasesDocument6 pagesPredictive Analytics: A Case Study in Machine-Learning and Claims DatabasesReemaNo ratings yet
- What Is Viral Pneumonia?: 8th Leading Cause of Death Children and People Over 65Document10 pagesWhat Is Viral Pneumonia?: 8th Leading Cause of Death Children and People Over 65Andeariesa DarmansiusNo ratings yet
- Tourette Syndrome Educational Based-InterventionsDocument24 pagesTourette Syndrome Educational Based-InterventionsThelma Lizeth Cárdenas Macías100% (1)
- Acute Chronic Renal FailureDocument43 pagesAcute Chronic Renal FailureHigh Education100% (1)
- Prevention and Control of Soil-Transmitted Helminthiasis With Focus On DewormingDocument51 pagesPrevention and Control of Soil-Transmitted Helminthiasis With Focus On DewormingDaxw JlmiNo ratings yet
- Munch SyndromeDocument2 pagesMunch SyndromeGrigoras Laura IoanaNo ratings yet
- Iron Deficiency Anemia Among Pregnant Women in Nablus District Prevalence Knowledge Attitude and Practices PDFDocument72 pagesIron Deficiency Anemia Among Pregnant Women in Nablus District Prevalence Knowledge Attitude and Practices PDFEArl CopinaNo ratings yet
- Digestive SystemDocument29 pagesDigestive Systemsugar kookie0% (1)
- Drug Study and Mental Health AssessmentDocument8 pagesDrug Study and Mental Health AssessmentVincent Quitoriano100% (1)
- Asher - Bacteria, Inc.Document48 pagesAsher - Bacteria, Inc.Iyemhetep100% (1)
- Diabetes Mellitus LECTURE Yr IIIDocument27 pagesDiabetes Mellitus LECTURE Yr IIIMwanja Moses100% (1)
- Turner Syndrome Research PaperDocument7 pagesTurner Syndrome Research Paperapi-316370647100% (1)
- Review: Lenat Joffe, Elena J LadasDocument11 pagesReview: Lenat Joffe, Elena J LadasGUSTAVO BELLONo ratings yet
- Abnormal Psychology Summary (Chapter 1 - 2)Document29 pagesAbnormal Psychology Summary (Chapter 1 - 2)Louise Alenah LabragueNo ratings yet
- Listeria Monocytogenes (Listeriosis) 2-12-2015Document11 pagesListeria Monocytogenes (Listeriosis) 2-12-2015MohamedNo ratings yet
- Pead 3 - Abdominal Pain and VommitingDocument22 pagesPead 3 - Abdominal Pain and Vommitingbbyes100% (1)
- Referat EndosDocument29 pagesReferat EndosShenaquitaIvandraNo ratings yet
- Oral& Dental Health Lecture SlidesDocument40 pagesOral& Dental Health Lecture SlidesvelangniNo ratings yet
- Smoking - Effects On Your Body - Better Health ChannelDocument7 pagesSmoking - Effects On Your Body - Better Health ChannelUmair MalikNo ratings yet
- Dental Caries CaseDocument5 pagesDental Caries CaseEerrmmaa Ssaarrell Rroommaann PpaarraaNo ratings yet
- Reading Test 1 - Part A': Page - 1Document13 pagesReading Test 1 - Part A': Page - 1Ryu TseNo ratings yet
- Nut 3704 AssignmentDocument6 pagesNut 3704 AssignmentCebisile NeneNo ratings yet
- Oncologic Emergencies: Kristine P. Palisoc-Perez, MD Second Year ResidentDocument78 pagesOncologic Emergencies: Kristine P. Palisoc-Perez, MD Second Year Residentlady cuison100% (2)
- CariologyDocument6 pagesCariologyNadia Khalil100% (1)
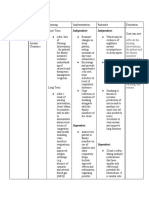
- Independent: IndependentDocument5 pagesIndependent: IndependentEspiritu, ChriscelNo ratings yet
- Yintang (M-Hn-3) : Hall of ImpressionDocument1 pageYintang (M-Hn-3) : Hall of Impressionray72roNo ratings yet