Download as docx, pdf, or txt
You might also like
- Ebook - The Great Neuropathy HoaxDocument48 pagesEbook - The Great Neuropathy HoaxJu Ri100% (7)
- Internal Medicine: Over 200 Case StudiesFrom EverandInternal Medicine: Over 200 Case StudiesRating: 4.5 out of 5 stars4.5/5 (18)
- Neurology High Yield Notes For Step 1Document25 pagesNeurology High Yield Notes For Step 1Lucykesh100% (8)
- Optic Nerve Atrophy and HomoeopathyDocument21 pagesOptic Nerve Atrophy and HomoeopathyDr. Rajneesh Kumar Sharma MD Hom100% (1)
- Long Cases Key TopicsDocument109 pagesLong Cases Key TopicsXu PeihaoNo ratings yet
- Klinik ÖzetDocument10 pagesKlinik ÖzetEllaNo ratings yet
- Med-Lgis-Diabetes Mellitus Complications-Dr. Saima Ambreen Mu1 HFHDocument47 pagesMed-Lgis-Diabetes Mellitus Complications-Dr. Saima Ambreen Mu1 HFHHassan Latif SheikhNo ratings yet
- Chronic Myeloproliferative Disorders: Matthew G. Yap, MD, FPCP, FPSHBT, FpsmoDocument42 pagesChronic Myeloproliferative Disorders: Matthew G. Yap, MD, FPCP, FPSHBT, FpsmoDon RaulNo ratings yet
- Uworld NotesDocument7 pagesUworld NotesJorge L CastelarNo ratings yet
- Screening For Micro and Macrovascular ComplicationDocument38 pagesScreening For Micro and Macrovascular ComplicationRoby KieranNo ratings yet
- Rhabdomyolysis - PACTDocument2 pagesRhabdomyolysis - PACTSanj.etcNo ratings yet
- Internal MedicineDocument10 pagesInternal Medicine96k7z7khz7No ratings yet
- Diabetes Mellitus ComplicationsDocument64 pagesDiabetes Mellitus ComplicationsAdria Putra FarhandikaNo ratings yet
- Anemias: Disorders of The Red Blood CellsDocument32 pagesAnemias: Disorders of The Red Blood CellsDthird Mendoza ClaudioNo ratings yet
- 1) DM, Cellulits, ACSDocument22 pages1) DM, Cellulits, ACSNu JoeNo ratings yet
- Chronic Kidney Disease. GolwallaDocument8 pagesChronic Kidney Disease. GolwallaAbdul QuyyumNo ratings yet
- Nephrotic and Nephritic Syndrome: Med5010 LectureDocument65 pagesNephrotic and Nephritic Syndrome: Med5010 LectureFreeburn Simunchembu100% (1)
- (Study Group) Diabetic Nephropathy, Hypertensive NephropathyDocument7 pages(Study Group) Diabetic Nephropathy, Hypertensive NephropathyZarif IzzuddinNo ratings yet
- Post PregnantDocument27 pagesPost PregnantShreyas RavishankarNo ratings yet
- Remembered Topics Step 2 2005 PDFDocument0 pagesRemembered Topics Step 2 2005 PDFRuchi Jhoom PatelNo ratings yet
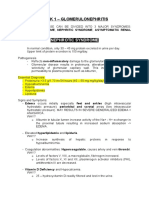
- Week 1 - Glomerulonephritis: Nephrotic SyndromeDocument5 pagesWeek 1 - Glomerulonephritis: Nephrotic SyndromeDapot SianiparNo ratings yet
- Complications of Diabetes MellitusDocument49 pagesComplications of Diabetes MellitusSiddiq Blackhell CakepNo ratings yet
- Nephrotic/Nephritic Syndrome: AK. Soyibo Department of Medicine Review ClassDocument143 pagesNephrotic/Nephritic Syndrome: AK. Soyibo Department of Medicine Review ClassKay BristolNo ratings yet
- Anaemia: by Swaathi R Final Year MbbsDocument33 pagesAnaemia: by Swaathi R Final Year MbbsGopi NathNo ratings yet
- DKA To CRFDocument4 pagesDKA To CRFMark Anthony YabresNo ratings yet
- Complications of Diabetes MellitusDocument49 pagesComplications of Diabetes MellitusJennifer WootenNo ratings yet
- Renal Chart 2Document21 pagesRenal Chart 2fortheloveofmedicineNo ratings yet
- LP 3 Metabolismul GlucidicDocument32 pagesLP 3 Metabolismul GlucidicLupu AlexandruNo ratings yet
- Diabetes - Lecture: Prof. Dr. Doina CatrinoiuDocument131 pagesDiabetes - Lecture: Prof. Dr. Doina CatrinoiuPantea Constantin AlinNo ratings yet
- Diabetic Retinopathy - Aetiopathogenesis, Clinical Presentation andDocument83 pagesDiabetic Retinopathy - Aetiopathogenesis, Clinical Presentation andOlayemi Olorundare0% (1)
- Bone Marrow FailureDocument39 pagesBone Marrow FailureRahulNo ratings yet
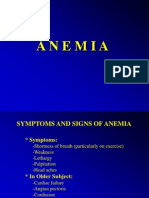
- Anemia (Syptoms and Signs)Document17 pagesAnemia (Syptoms and Signs)Primarini RiatiNo ratings yet
- Nephrotic Syndrome: Prepared by Dr. Kawsar Ahmed Intern Dr. (TMMCH)Document26 pagesNephrotic Syndrome: Prepared by Dr. Kawsar Ahmed Intern Dr. (TMMCH)GENERAL sharpNo ratings yet
- Pathoma Notes Part 2 - TPDocument48 pagesPathoma Notes Part 2 - TPJey DeeNo ratings yet
- Acute and Chronic Kidney DiseaseDocument20 pagesAcute and Chronic Kidney DiseaseCabdi WaliNo ratings yet
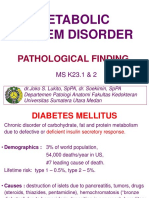
- Patologi Pankreas Endokrin & AdrenalDocument69 pagesPatologi Pankreas Endokrin & AdrenalSonia Afika AzizaNo ratings yet
- Disease of Myocardium and PericardiumiDocument49 pagesDisease of Myocardium and PericardiumiDeepika LamichhaneNo ratings yet
- Cardiovascular PathologyDocument182 pagesCardiovascular PathologyPavan chowdaryNo ratings yet
- Internal MedicineDocument168 pagesInternal Medicinebolt boltNo ratings yet
- Diabetes Mellitus Study GuideDocument5 pagesDiabetes Mellitus Study Guiderr5633No ratings yet
- HP Pathologies SummaryDocument10 pagesHP Pathologies SummaryMiki AberaNo ratings yet
- AnaemiaDocument83 pagesAnaemiaMohammad_Islam87100% (2)
- Complications of Diabetes Mellitus: DR Shamila de Silva Department of Medicine - 2009Document41 pagesComplications of Diabetes Mellitus: DR Shamila de Silva Department of Medicine - 2009rikarzNo ratings yet
- Imed Block Stations: 1. Cxray - Pleural Effusion-Interpret X RayDocument13 pagesImed Block Stations: 1. Cxray - Pleural Effusion-Interpret X RayCaroline RatuNo ratings yet
- Blok Sistem Metabolik RevisiDocument53 pagesBlok Sistem Metabolik RevisiRobith LubisNo ratings yet
- Chronic Renal FailureDocument54 pagesChronic Renal FailureAkia Cayasan BayaNo ratings yet
- Noel A. Villanueva, MD, FPCP, FPSNDocument62 pagesNoel A. Villanueva, MD, FPCP, FPSNagilNo ratings yet
- Lab InvestigationDocument3 pagesLab InvestigationArunkumarmenganeNo ratings yet
- Lec6.nephrotic SyndromeDocument24 pagesLec6.nephrotic SyndromeMAD Bl00DNo ratings yet
- Komplikasi Kronik DMDocument26 pagesKomplikasi Kronik DMsarelriskyNo ratings yet
- UWorld Cards July 14Document7 pagesUWorld Cards July 14smian08No ratings yet
- Management of Acute Kidney InjuryDocument31 pagesManagement of Acute Kidney InjurysumitNo ratings yet
- Complications of Diabetes Mellitus-UpdateDocument48 pagesComplications of Diabetes Mellitus-UpdateAnditha Namira RS100% (1)
- Chronic Kidney DiseaseDocument39 pagesChronic Kidney DiseaseMohmmadRjab SederNo ratings yet
- Diabetes MellitusDocument37 pagesDiabetes MellitusenriNo ratings yet
- PancreasDocument46 pagesPancreasgzrgythpyjNo ratings yet
- Take Home Exam - Ali, Habiba L.Document5 pagesTake Home Exam - Ali, Habiba L.hally_lipNo ratings yet
- Cute and Hronic: Renal FailureDocument31 pagesCute and Hronic: Renal FailureEhab S. AlHarbiNo ratings yet
- Fast Facts: Deficiencia de piruvato quinasa para pacientes y familiares: Una enfermedad genética rara que afecta a los glóbulos rojos Información + Asumir el control = El mejor resultadoFrom EverandFast Facts: Deficiencia de piruvato quinasa para pacientes y familiares: Una enfermedad genética rara que afecta a los glóbulos rojos Información + Asumir el control = El mejor resultadoNo ratings yet
- 194 Surgical Cases PDFDocument160 pages194 Surgical Cases PDFkint100% (4)
- Types of PainDocument1 pageTypes of PainTracy100% (3)
- Amitriptyline Information Booklet Jan2022Document7 pagesAmitriptyline Information Booklet Jan2022Roger MundiNo ratings yet
- Catalogo MiS EN PDFDocument12 pagesCatalogo MiS EN PDFAnt Son MINo ratings yet
- MEHU130 - U2 - T43 - Nefropatia DiabeticaDocument110 pagesMEHU130 - U2 - T43 - Nefropatia DiabeticaStefani AtlleNo ratings yet
- UWorld Notes Step 2 CKDocument11 pagesUWorld Notes Step 2 CKSamah Khan67% (3)
- Crat 211 - DM TransDocument4 pagesCrat 211 - DM TransLovely GopezNo ratings yet
- Type 1 Diabetes Mellitus Clinical Presentation - History, Physical Examination, ComplicationsDocument6 pagesType 1 Diabetes Mellitus Clinical Presentation - History, Physical Examination, ComplicationsTrifosa Ika Septiana EryaniNo ratings yet
- Classification of PainDocument3 pagesClassification of Painfeby alexesNo ratings yet
- IWII CD 2022 Web 1Document57 pagesIWII CD 2022 Web 1Elton RlNo ratings yet
- Pain 3Document3 pagesPain 3Ka Yi MonicaNo ratings yet
- Diabetes (12. Retinopatía, Neuropatía y Cuidado de Los Pies - Estándares de Atención Médica en La Diabetes - 2022)Document10 pagesDiabetes (12. Retinopatía, Neuropatía y Cuidado de Los Pies - Estándares de Atención Médica en La Diabetes - 2022)Antony Yamid Bolaños VillarrealNo ratings yet
- Clinical and Biochemiical Manifestations of Vitamin B12 Deficiency in Type 2 Diabetic Patients Treated With Metformin - A Comparative StudyDocument8 pagesClinical and Biochemiical Manifestations of Vitamin B12 Deficiency in Type 2 Diabetic Patients Treated With Metformin - A Comparative StudyIJAR JOURNALNo ratings yet
- Komplikasi Diabetes (Akut Dan Kronik) : Luh Gede Sri YennyDocument50 pagesKomplikasi Diabetes (Akut Dan Kronik) : Luh Gede Sri YennyArya WinataNo ratings yet
- Uniuyo Physiology Final Project (CHAPTER 1&2)Document41 pagesUniuyo Physiology Final Project (CHAPTER 1&2)Itoro UdohNo ratings yet
- Diabetic FootDocument68 pagesDiabetic FootNadzira KarimaNo ratings yet
- Manajemen Nyeri Neuropati Pada Pasien Diabetes Melitus Tipe 2: Studi LiteraturDocument7 pagesManajemen Nyeri Neuropati Pada Pasien Diabetes Melitus Tipe 2: Studi LiteraturFaridah HakimNo ratings yet
- Fact Sheet Painful Peripheral NeuropathyDocument6 pagesFact Sheet Painful Peripheral Neuropathyasdar fajrinNo ratings yet
- Diabetic NeuropathyDocument10 pagesDiabetic NeuropathyIrma Sari RasyidNo ratings yet
- Acupuncture and Cancer Pain: Yan Cui Magram and Gary E. DengDocument4 pagesAcupuncture and Cancer Pain: Yan Cui Magram and Gary E. DengirmaNo ratings yet
- Immune Mediated Neuromuscular Diseases PourmandDocument179 pagesImmune Mediated Neuromuscular Diseases PourmandMihaela BocaNo ratings yet
- Drug Index Updated2Document113 pagesDrug Index Updated2tam meiNo ratings yet
- ExamDocument50 pagesExamSyeda Eshaal JavaidNo ratings yet
- Tingling and NumbnessDocument67 pagesTingling and NumbnessAradhanaRamchandaniNo ratings yet
- Pty 304 PDDocument135 pagesPty 304 PDSuman RazaNo ratings yet
- Capsaicina Tópica en El Tratamiento Del Dolor Neuropático: RevisiónDocument13 pagesCapsaicina Tópica en El Tratamiento Del Dolor Neuropático: RevisiónJAVIER RODRIGUEZNo ratings yet
- Sudden Visual Loss - PPTX, MergencyDocument31 pagesSudden Visual Loss - PPTX, MergencyArsyil Ardiman MirwanNo ratings yet
- Entrapment Neuropathies Conversion-GateDocument76 pagesEntrapment Neuropathies Conversion-GateRam ReddyNo ratings yet