Download as docx, pdf, or txt
You might also like
- July 23, 2009 Through August 24, 2009 JPMorgan Chase BankDocument4 pagesJuly 23, 2009 Through August 24, 2009 JPMorgan Chase BankMaria Blackburn33% (3)
- Astm C469 - C469M - 14Document5 pagesAstm C469 - C469M - 14adil Rahman hassoon100% (1)
- LayersDocument561 pagesLayersionut1ilie-1100% (1)
- Tooth WhiteningDocument165 pagesTooth Whiteningionut1ilie-1100% (2)
- Sofitel Philippine Plaza Manila Cultural Orientations FrameworkDocument3 pagesSofitel Philippine Plaza Manila Cultural Orientations FrameworkApril Jane EvangelistaNo ratings yet
- ChE 140 1.01 IntroductionDocument30 pagesChE 140 1.01 IntroductionJelor GallegoNo ratings yet
- The Genetic Basis of Dental Anomalies and Its Relation To OrthodonticsDocument5 pagesThe Genetic Basis of Dental Anomalies and Its Relation To Orthodonticsyuniarita eka putriNo ratings yet
- Genetics of Dentofacial and Orthodontic AbnormalitiesDocument6 pagesGenetics of Dentofacial and Orthodontic AbnormalitiesMariana SantosNo ratings yet
- Managing Congenitally Missing Lateral Incisors With Single Tooth ImplantsDocument7 pagesManaging Congenitally Missing Lateral Incisors With Single Tooth Implantsshatz_014No ratings yet
- 954 1638 1 SM PDFDocument6 pages954 1638 1 SM PDFIndah AmaliaNo ratings yet
- Tmp50e TMPDocument11 pagesTmp50e TMPFrontiersNo ratings yet
- Article Genetics PDFDocument5 pagesArticle Genetics PDFAkshatNo ratings yet
- Butlers Field Theory PDFDocument7 pagesButlers Field Theory PDFsuchitra100% (1)
- A Curriculum Vitae of Teeth Evolution, Generation, RegenerationDocument18 pagesA Curriculum Vitae of Teeth Evolution, Generation, RegenerationDulce MartinezNo ratings yet
- Nibali Development of The Gingival Sulcus 2017 AcceptedDocument14 pagesNibali Development of The Gingival Sulcus 2017 AcceptedLily BrostNo ratings yet
- The Structure of Dental Plaque - Listgarten (1994)Document14 pagesThe Structure of Dental Plaque - Listgarten (1994)madiesNo ratings yet
- A Review On Non-Syndromic Tooth Agenesis Associated With PAX9 MutationsDocument7 pagesA Review On Non-Syndromic Tooth Agenesis Associated With PAX9 Mutationssümeyra akkoçNo ratings yet
- Hypodontia: An Update On It 'S Etiology, Classification, and Clinical ManagementDocument23 pagesHypodontia: An Update On It 'S Etiology, Classification, and Clinical Managementionut1ilie-1No ratings yet
- 08-The Heritability of Malocclusion-Part 2 The Influence of Genetics in Malocclusion PDFDocument9 pages08-The Heritability of Malocclusion-Part 2 The Influence of Genetics in Malocclusion PDFFadi Al Hajji100% (1)
- Patterns of Heritability Across The Human Diphyodont Dental Complex: Crown Morphology of Australian Twins and FamiliesDocument15 pagesPatterns of Heritability Across The Human Diphyodont Dental Complex: Crown Morphology of Australian Twins and FamiliesJOHN MARIO PINTO RAMIREZNo ratings yet
- Management of Patient With Hypodontia: Review of Literature and Case ReportDocument16 pagesManagement of Patient With Hypodontia: Review of Literature and Case ReportAnonymous v2aJxfe9RzNo ratings yet
- Morphological Variation of The Maxillary Lateral Incisor: SciencedirectDocument8 pagesMorphological Variation of The Maxillary Lateral Incisor: SciencedirectKanish AggarwalNo ratings yet
- Supernumerary Teeth: Review of The Literature and A Survey of 152 CasesDocument11 pagesSupernumerary Teeth: Review of The Literature and A Survey of 152 CasesfatimahNo ratings yet
- Cobourne (1999) The Genetic Control of Early OdontogenesisDocument0 pagesCobourne (1999) The Genetic Control of Early OdontogenesisMaja Maja BułkaNo ratings yet
- Review Article: Hypodontia: An Update On Its Etiology, Classification, and Clinical ManagementDocument9 pagesReview Article: Hypodontia: An Update On Its Etiology, Classification, and Clinical Managementionut1ilie-1No ratings yet
- Microleakage PDFDocument16 pagesMicroleakage PDFbyyou0% (1)
- Review Article: Hypodontia: An Update On Its Etiology, Classification, and Clinical ManagementDocument10 pagesReview Article: Hypodontia: An Update On Its Etiology, Classification, and Clinical ManagementUlfa RahmaNo ratings yet
- Dentists and Preventive Oral Health Care: February 2012Document27 pagesDentists and Preventive Oral Health Care: February 2012Mike Lawrence CadizNo ratings yet
- Genetics in OrthodonticsDocument56 pagesGenetics in OrthodonticsSadhu AbhijeetNo ratings yet
- Dental Development and Craniofacial Morphology in School-Age ChildrenDocument4 pagesDental Development and Craniofacial Morphology in School-Age ChildrenAyman RaoNo ratings yet
- Dental Follicle Role in Development of Odontogenic Cysts and TumoursDocument9 pagesDental Follicle Role in Development of Odontogenic Cysts and TumoursCamila CastiblancoNo ratings yet
- Genes For TeethDocument14 pagesGenes For TeethAhmadH.MahdiNo ratings yet
- The Nature and Mechanisms of Dental Fluorosis in Man: Et Al.Document9 pagesThe Nature and Mechanisms of Dental Fluorosis in Man: Et Al.mageshwariNo ratings yet
- Sıddık Malkoç Faruk Ayhan Başçiftçi Metin Nur Bülent ÇatalbaşDocument5 pagesSıddık Malkoç Faruk Ayhan Başçiftçi Metin Nur Bülent ÇatalbaşRazvan SalageanNo ratings yet
- 8.full BioDocument12 pages8.full BioDilla Novia AmrilaniNo ratings yet
- Anodontia An Update On Ethiology PDFDocument31 pagesAnodontia An Update On Ethiology PDFcareNo ratings yet
- Hypodontia: An Update On Its Etiology, Classification and Clinical ManagementDocument31 pagesHypodontia: An Update On Its Etiology, Classification and Clinical ManagementcareNo ratings yet
- Grand Challenges in Comparative Tooth Biology: SymposiumDocument18 pagesGrand Challenges in Comparative Tooth Biology: SymposiumSamuelHpNo ratings yet
- Dentoskeletal Features Associated With Unilateral or Bilateral Palatal Displacement of Maxillary CaninesDocument8 pagesDentoskeletal Features Associated With Unilateral or Bilateral Palatal Displacement of Maxillary Canineskh jhNo ratings yet
- Teeth, Genes, and GenealogyDocument4 pagesTeeth, Genes, and GenealogyPablo BenitezNo ratings yet
- ElA FKG-UI1Document12 pagesElA FKG-UI1mahaaNo ratings yet
- Arch Form Children 08 00514Document11 pagesArch Form Children 08 00514ebruNo ratings yet
- The Epidemiology of Supernumerary Teeth and The Associated Molecular MechanismDocument21 pagesThe Epidemiology of Supernumerary Teeth and The Associated Molecular MechanismCalvintNo ratings yet
- Mesiodens Etiology, Prevalence, Diagnosis and ManagementDocument4 pagesMesiodens Etiology, Prevalence, Diagnosis and ManagementsyedNo ratings yet
- Reiterative Signaling and Patterning During MammalianDocument11 pagesReiterative Signaling and Patterning During MammalianJhon Mario Pinto RamirezNo ratings yet
- Alteracion de La Erupcion de MolaresDocument9 pagesAlteracion de La Erupcion de MolaresCARLOS DARIO MERINO BUSTAMANTENo ratings yet
- Tongue Crenation Scalloped Tongue - Case Report PDFDocument4 pagesTongue Crenation Scalloped Tongue - Case Report PDFRiri GustiawarmanNo ratings yet
- The Genetic Basis of Normal and Abnormal Craniofacial Development. Acta Odontol Scand, 56 321-325, 1998Document6 pagesThe Genetic Basis of Normal and Abnormal Craniofacial Development. Acta Odontol Scand, 56 321-325, 1998Muhammad AsimNo ratings yet
- Development of OcclusionDocument17 pagesDevelopment of OcclusionIJAR JOURNALNo ratings yet
- MoleculaDocument114 pagesMoleculaDilla Novia AmrilaniNo ratings yet
- Management of Temporomandibular Disorder Associated With BruxismDocument3 pagesManagement of Temporomandibular Disorder Associated With Bruxismmdaniel74No ratings yet
- Genetics in Pediatric Dentistry - A Review: Drifzah, DR - Divyaprahlad, DR - Priya Subramaniam, DR - Kinjal ShahDocument9 pagesGenetics in Pediatric Dentistry - A Review: Drifzah, DR - Divyaprahlad, DR - Priya Subramaniam, DR - Kinjal Shahanusha guptaNo ratings yet
- Frankel Expansion de ArcoDocument13 pagesFrankel Expansion de ArcoLisdany BecerraNo ratings yet
- Hipoplasia EstatusDocument15 pagesHipoplasia EstatusAleida Cetina BastidaNo ratings yet
- Scot 1988Document28 pagesScot 1988Freddy Campos SotoNo ratings yet
- Butler's Field TheoryDocument5 pagesButler's Field Theorypveginadu100% (1)
- Factors Influencing Permanent Teeth Eruption. Part One - General FactorsDocument6 pagesFactors Influencing Permanent Teeth Eruption. Part One - General FactorsestherNo ratings yet
- 6.microbiota of Deciduous Endodontic InfectionsDocument11 pages6.microbiota of Deciduous Endodontic InfectionsMihaela TuculinaNo ratings yet
- Stem Cell Based Tooth Regeneration - An Alternative Approach To Implant DentistryDocument6 pagesStem Cell Based Tooth Regeneration - An Alternative Approach To Implant DentistryInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Dental Tissue Regeneration - A Mini-ReviewDocument10 pagesDental Tissue Regeneration - A Mini-ReviewUngureanu AndreiNo ratings yet
- Mccollum 2001Document7 pagesMccollum 2001punthadewaNo ratings yet
- Fcell 11 1174579Document23 pagesFcell 11 1174579Biologija BiologyNo ratings yet
- Tongue Crenation Scalloped Tongue - Case ReportDocument4 pagesTongue Crenation Scalloped Tongue - Case Reportceceu nahhNo ratings yet
- Tongue Crenation Scalloped Tongue - Case ReportDocument4 pagesTongue Crenation Scalloped Tongue - Case ReportCleverys Qisthi PhiennaNo ratings yet
- AdvHumBiol 2016 6 3 112 195316Document9 pagesAdvHumBiol 2016 6 3 112 195316yunitaananda39No ratings yet
- Vertise Flow CompositeDocument24 pagesVertise Flow Compositeionut1ilie-1No ratings yet
- Pancreas: Cynthia D. Guy, MD Associate Professor of Pathology DumcDocument56 pagesPancreas: Cynthia D. Guy, MD Associate Professor of Pathology Dumcionut1ilie-1No ratings yet
- Hypodontia: An Update On It 'S Etiology, Classification, and Clinical ManagementDocument23 pagesHypodontia: An Update On It 'S Etiology, Classification, and Clinical Managementionut1ilie-1No ratings yet
- Review Article: Hypodontia: An Update On Its Etiology, Classification, and Clinical ManagementDocument9 pagesReview Article: Hypodontia: An Update On Its Etiology, Classification, and Clinical Managementionut1ilie-1No ratings yet
- Boala ParkinsonDocument16 pagesBoala Parkinsonionut1ilie-1100% (1)
- Curs Proteine 2014Document77 pagesCurs Proteine 2014ionut1ilie-1100% (1)
- Economics SBADocument24 pagesEconomics SBAJamol benjaminNo ratings yet
- An Empirical Analysis of The Antecedents and Performance Consequences of Using The Moodle PlatformDocument5 pagesAn Empirical Analysis of The Antecedents and Performance Consequences of Using The Moodle Platformsamas7480No ratings yet
- WaterproofingDocument7 pagesWaterproofingNeda Shakil100% (1)
- Questionmark PerceptionDocument4 pagesQuestionmark PerceptionRenatoNo ratings yet
- CAEG Question Bank With SolutionsDocument24 pagesCAEG Question Bank With Solutionssksnjgaming100% (1)
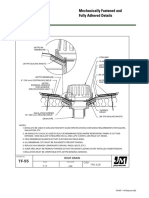
- JM Mechanically Fastened and Adhered Details UltraGard TPO Roof Drain New Construction Detail Drawing B18270Document1 pageJM Mechanically Fastened and Adhered Details UltraGard TPO Roof Drain New Construction Detail Drawing B18270michael jan tubongbanuaNo ratings yet
- SAp QM OverviewDocument80 pagesSAp QM OverviewAlfonso Herrera RojasNo ratings yet
- The Featinian Issue 2 2011-2012Document12 pagesThe Featinian Issue 2 2011-2012Saxs Gabrielle Peralta SantosNo ratings yet
- UGCNETDEC AdmitCardDocument1 pageUGCNETDEC AdmitCardAkshay RajNo ratings yet
- History: The History of The Hospitality Industry Dates All The WayDocument10 pagesHistory: The History of The Hospitality Industry Dates All The WaySAKET TYAGINo ratings yet
- Steam TurbineDocument16 pagesSteam TurbineVinayakNo ratings yet
- Sporlan TXV CatalogDocument40 pagesSporlan TXV CatalogDavid EllisNo ratings yet
- 2 Grade English ReaderDocument176 pages2 Grade English ReaderaniteshsannigrahiNo ratings yet
- Cores - TabelaDocument5 pagesCores - TabelahelberfuzerNo ratings yet
- EDFD 211: Psychological Foundations in Education First Semester SY 2016-17 Course DescriptionDocument4 pagesEDFD 211: Psychological Foundations in Education First Semester SY 2016-17 Course DescriptionLeezl Campoamor OlegarioNo ratings yet
- Jeppview For Windows: General Information Communication Information General InformationDocument34 pagesJeppview For Windows: General Information Communication Information General InformationAviation WithvoiceNo ratings yet
- Sika Backing FillerDocument2 pagesSika Backing FillerErdenebileg SangidorjNo ratings yet
- Combustion Products From Ventilation Controlled Fires - Thesis PDFDocument321 pagesCombustion Products From Ventilation Controlled Fires - Thesis PDFYuri SanchezNo ratings yet
- EntropyDocument21 pagesEntropycusgakungaNo ratings yet
- 4 - 20140515034803 - 1 Coase, R.H. 1937 The Nature of The FirmDocument24 pages4 - 20140515034803 - 1 Coase, R.H. 1937 The Nature of The FirmFelicia AprilianiNo ratings yet
- Technical SubmittalDocument121 pagesTechnical SubmittalSyed Sabir Ahmed100% (1)
- VR8304 Intermittent Pilot Combination Gas Control: ApplicationDocument8 pagesVR8304 Intermittent Pilot Combination Gas Control: ApplicationGregorio Mata MartínezNo ratings yet
- Quantum Tunneling and Spin 14Document14 pagesQuantum Tunneling and Spin 14plfratarNo ratings yet
- HITO 2004 Annual ReportDocument15 pagesHITO 2004 Annual ReportHITONo ratings yet
- Manuel Resume 17Document2 pagesManuel Resume 17api-286125655No ratings yet
- ILRAP HandbookDocument40 pagesILRAP Handbooknaren_3456No ratings yet